




Equine granulocytic anaplasmosis is a febrile disease of horses caused by the tick-transmitted bacterium Anaplasma phagocytophilum. The disease can produce a high fever, which is responsive to tetracycline-class drugs. Equine and canine infections serve as sentinels for human risk because the same tick species can transmit the pathogen to any of these host species.
Equine granulocytic anaplasmosis (EGA) is an infectious, noncontagious, seasonal disease, originally seen in the USA in northern California but now recognized in many states where the tick vectors occur; it is also seen in Europe, Africa, and South America.
Etiology, Epidemiology, and Transmission of Equine Granulocytic Anaplasmosis
The causal rickettsial agent of EGA in horses was initially termed Ehrlichia equi, but based on DNA sequence relationships, the taxonomy of the organism was reclassified, and it is now referred to as Anaplasma phagocytophilum. The organism has a wide host range; naturally occurring infections have been seen in horses, burros, dogs, llamas, rodents, and people (in whom the disease is designated human granulocytic anaplasmosis, HGA). Cases in people are most common in the upper midwestern and northeastern states in the USA and occur in many other countries worldwide.
A phagocytophilum frequently infects horses in some areas where the tick vector (Ixodes sp) is present. The geographic distribution mirrors that of cases in people.
A phagocytophilum is present in cytoplasmic vacuoles of neutrophils and occasionally eosinophils during the acute phase of infection. Blood smears stained with Giemsa or Wright-Leishman stains reveal one or more loose aggregates (morulae or inclusion bodies, 1.5–5 mcm in diameter) of blue-gray to dark blue coccoid, coccobacillary, or pleomorphic organisms within the cytoplasm of neutrophils.
The infection can be transmitted experimentally to susceptible horses by whole blood from infected horses or from people with HGA. The incubation period is 1–3 weeks. I pacificus (the western black-legged tick), I scapularis, I ricinus, and I persulcatus can transmit A phagocytophilum to horses. The disease is seasonal in California, occurring in the late fall, winter, and spring.
There is no zoonotic risk of EGA infection to people via horses. Both people and horses are exposed through tick bites, so equine cases in an area serve as sentinels for human risk.
Clinical Findings of Equine Granulocytic Anaplasmosis

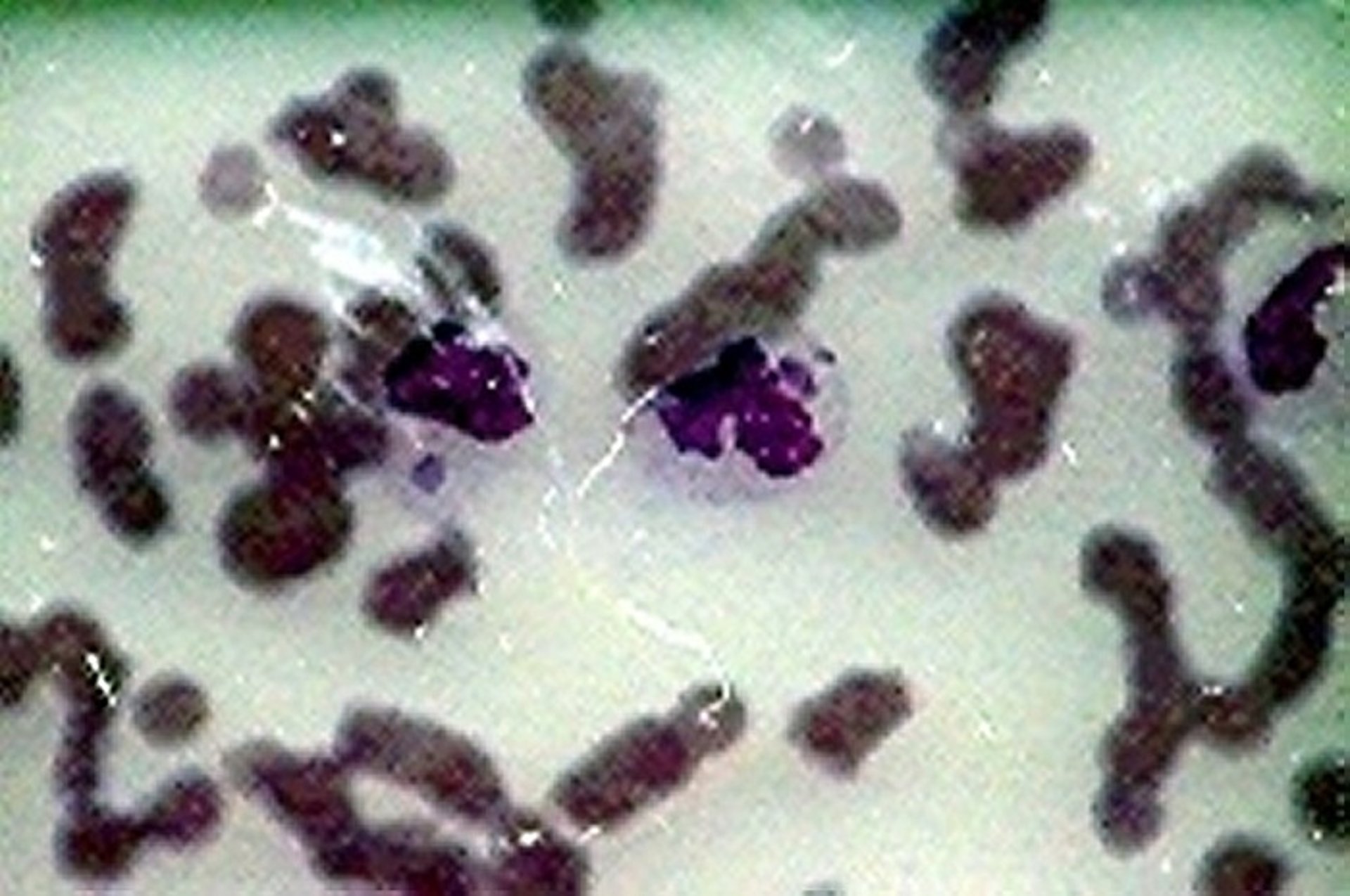
Courtesy of Dr. John W. Harvey.
Severity of signs of EGA varies with age of the horse and duration of the illness. Signs may be mild. Horses < 1 year old may have a fever only; horses 1–3 years old may develop fever, depression, mild limb edema, and ataxia. Adults, and particularly geriatric horses, may exhibit fever, partial anorexia, depression, reluctance to move, limb edema, petechiation, and icterus. The fever, which is highest after about 5 days of infection, is typically 103°–104°F (39.5°–40°C) but can be as high as 107°–108°F (41.7°–42.2°C). The fever can persist for 6–12 days. Signs become more severe over several days.
Rarely, myocardial vasculitis may cause transient ventricular arrhythmias. Other clinical presentations for acute infection have included recumbency and severe myopathy. Any concurrent infection (eg, a leg wound or respiratory infection) can be exacerbated. Cytoplasmic inclusion bodies are few during the first 48 hours and increase to 5%–40% of circulating neutrophils during peak bacteremia. Affected horses typically have leukocytopenia or pancytopenia with moderate to severe thrombocytopenia.
Lesions
Gross petechiation, ecchymoses, and edema develop in the subcutis and fascia. Vasculitis is regional, with the subcutis and fascia of the legs predominantly affected.
Diagnosis of Equine Granulocytic Anaplasmosis
Clinical findings, PCR, and serology
Horses should be considered suspect for EGA if they live in or have a travel history to an endemic area and present with acute fever and related clinical signs, particularly during seasons of high tick activity. Differential diagnoses include viral encephalitis, primary liver disease, equine infectious anemia, purpura hemorrhagica, and viral arteritis. A blood sample should be evaluated for complete blood counts, and the buffy coat can be enriched for neutrophils. Demonstration of the characteristic cytoplasmic inclusion bodies in neutrophils is diagnostic. However, inclusion bodies are difficult to see in the first day or two of fever, and the cytologist must differentiate the Anaplasma from other neutrophil inclusions.
PCR is the optimal test for EGA and can detect A phagocytophilum DNA in unclotted blood or buffy coat smears.
An indirect fluorescent antibody test may be negative early in the disease, whereas many horses in endemic areas may test positive, indicating exposure but not necessarily active disease. A four-fold rise in antibody titers to A phagocytophilum over 2–4 weeks can retrospectively confirm a diagnosis.
Treatment and Control of Equine Granulocytic Anaplasmosis
Antibiotics and supportive care
Oxytetracycline is extremely effective against A phagocytophilum. Delivery of diluted oxytetracycline in saline can reduce GI adverse reactions to the drug. Penicillin, chloramphenicol, and streptomycin have no inhibitory effect. Horses treated early in infection for short durations may relapse within the following few weeks.
Horses with severe ataxia and edema may benefit from short-term corticosteroid treatment (dexamethasone, 20 mg/day, for 2–3 days), fluid therapy, and pain management. The risk of laminitis appears to be very low; no laminitis has occurred in clinical cases or experimental infections.
Recovered horses are solidly immune for ≥2 years and are not believed to be carriers. Persistence of infection has been suggested with some European strains, but further verification is required. Tick control measures are mandatory for control of disease. There is no vaccine.
Key Points
Equine granulocytic anaplasmosis is a seasonal, tickborne bacterial disease of horses caused by an agent that can be transmitted to numerous other host species (via the tick), including people.
The causative agent targets horse neutrophils, and infection can produce severe fever, ataxia, and thrombocytopenia.
Antibiotics and supportive care are highly effective treatments for affected horses.
For More Information
Also see pet health content regarding equine granulocytic anaplasmosis.




