




Inappropriate or excessive activity of the adaptive immune system can lead to damaging immune responses collectively called hypersensitivities. In general, inappropriate innate immune responses do this by triggering inflammation that leads to collateral damage to nearby tissues or organs or by producing vastly excessive amounts of inflammatory cytokines.
One simple classification divides these hypersensitivity reactions into four types. Each involves very different mechanisms. Type I hypersensitivity is mediated by IgE antibodies and mast cells; type II by IgG and/or IgM antibodies and complement; type III by immune complexes, complement, and neutrophils; and type IV by T lymphocytes.
Type I Hypersensitivity Diseases
Type I, or immediate hypersensitivity, encompasses IgE-mediated responses to foreign antigens and are collectively called allergic diseases. These reactions may be minor and local or may be severe and generalized. In its most extreme form, type 1 hypersensitivity or allergy is expressed as a lethal shock syndrome called anaphylaxis. Anaphylaxis is an acute systemic manifestation of the interaction of an antigen (allergen) binding to IgE on mast cells and basophils. The antigen binding triggers the mast cell to release a complex mixture of inflammatory mediators, including the following:
histamine
leukotrienes
eosinophil chemotactic factors
platelet activating factor
kinins
serotonin
proteases
cytokines
Many of these molecules directly affect the vascular system, causing varying combinations of vasodilation, increased vascular permeability, and vasoconstriction. Other mediators attract eosinophils to the reaction site. These eosinophils also contribute to the inflammatory process, especially in cats.
The severity of anaphylaxis depends on the amount and type of antigen, the amount of IgE produced, and the route of exposure. If the animal has been previously sensitized by exposure to an allergen (antigen) and produces high levels of IgE antibodies, then injection of the sensitizing antigens directly into the bloodstream can result in anaphylactic shock and related allergic reactions such as hives and facial-conjunctival edema. If the sensitizing allergen enters through the mucous membranes or the skin, allergic reactions tend to be more localized. Antigens that can trigger anaphylactic and allergic reactions are numerous and include the venom of stinging and biting insects, some vaccines, drugs, foods, and foreign blood products.
Systemic Anaphylaxis in Animals
Anaphylactic shock, or systemic anaphylaxis, occurs in sensitized animals within seconds to minutes after exposure to the allergen. In most domestic species, the lungs are the primary target organs, and the portal-mesenteric vasculature is a secondary target; this is reversed in dogs. Mast cell degranulation releases large amounts of histamine and other mediators that cause constriction of bronchial airways or pulmonary veins, pooling of blood, and edema in the pulmonary vascular bed, resulting in dyspnea and severe respiratory distress. Mast cell degranulation in the portosystemic vasculature causes venous dilation and pooling of blood in the intestine and liver.
Clinical signs may be localized or generalized and include the following:
restlessness and excitement
pruritus around the head or site of exposure
facial edema
salivation
lacrimation
vomiting
abdominal pain
diarrhea
dyspnea
cyanosis
shock
incoordination
collapse
convulsions
death
In dogs, the major organ affected during anaphylaxis is the liver, and clinical signs are associated with constriction of hepatic veins, resulting in portal hypertension and visceral pooling of blood. GI signs rather than respiratory signs are more prominent in dogs. Immediate treatment, in addition to treating respiratory distress, consists of the systemic administration of epinephrine. Additional treatments include intravenous fluids to control shock and corticosteroids if needed. Ancillary support of blood pressure and respiration may also be necessary.
Urticarial reactions (hives) of the skin and subcutis and acute edema of the lips, conjunctiva, and skin of the face (facial-conjunctival angioedema) are less severe forms of type I hypersensitivity. Hives may not be associated with other clinical abnormalities. Facial-conjunctival edema is more severe and can be associated with mild to moderately severe systemic anaphylaxis in cats.
Urticarial reactions and facial-conjunctival edema occur in most species and usually resolve spontaneously within 24 hours. They are often intensely pruritic and can be masked by self-inflicted trauma.
Localized Allergic Reactions in Animals
Allergic rhinitis, manifested by serous nasal discharge and sneezing, is less common in domestic animals than in humans. Often, it is seasonal, correlating with pollen exposure. Nonseasonal rhinitis may be associated with exposure to ubiquitous allergens, such as molds, animal danders, bedding, and feeds.
Equine asthma is a response to chronic exposure to molds present in hay and poorly ventilated stables. The airways may be infiltrated with eosinophils or neutrophils depending on the nature of the hypersensitivity response. Summer snuffles is a seasonal allergic rhinitis occurring in Guernsey or Jersey cattle placed on certain types of flowering pastures in late summer and early autumn.
Allergic rhinitis can be diagnosed tentatively by the following:
identification of eosinophils in the nasal exudate
demonstration of a favorable response to antihistamines
disappearance of clinical signs when the offending allergen is removed
occasionally, its seasonal nature
Skin testing is not an accurate means of identifying the causes of nasal allergies in animals.
Chronic allergic bronchitis has been diagnosed in dogs. A dry, harsh, hacking cough that is easily precipitated by exertion or by pressure on the trachea is a characteristic clinical sign. The disease may be seasonal. It is not usually associated with other clinical signs of illness. The bronchial exudate is rich in eosinophils and free of bacteria. Chest radiographs are normal, and patients may have a low-grade eosinophilia.
The condition is treated with bronchodilators and expectorants (theophylline and potassium iodide or guaifenesin). Glucocorticoids will alleviate clinical signs, especially when their use can be limited to certain seasons or to low-dose, alternate-day treatment. Avoidance of the offending allergen(s) usually is not possible.
Allergic bronchiolitis is common in cats. It is manifested by a low-grade cough, wheezing, some dyspnea, and increased peribronchiolar density on radiographs. Allergic bronchiolitis may be mistaken for other conditions, such as lungworm disease (see allergic bronchiolitis radiograph).


Courtesy of Dr. Ronald Green.
Early in the course of the disease, clinical signs can be decreased by treatment with anti-inflammatory drugs; however, if the disease increases in severity, moderate to high dosages of corticosteroids may be necessary. The offending allergen usually is not identified.
Pulmonary infiltration with eosinophilia occurs most frequently in dogs. It is associated with diffuse inflammatory infiltrates in the lungs and a pronounced peripheral eosinophilia; frequently, serum globulins are increased. Unlike with allergic bronchitis, affected animals are often dyspneic or tire easily with exercise. The bronchial exudate contains numerous eosinophils. The offending allergen is rarely identified. Glucocorticoids are the treatment of choice. A similar syndrome is also associated with resident or migratory parasitic infections of the lungs in young animals.
Allergic asthma occurs most frequently in cats, in which the clinical signs are similar to those in humans. It occurs more frequently in summer and in some cats can be triggered by going outdoors. Indoor cats can also get asthma, often in response to dust mite allergens. Individual attacks can be transient and mild or can be protracted and severe (status asthmaticus). Mild attacks may manifest as wheezing and coughing; in severe attacks, the following may occur:
expiratory dyspnea
hyperinflation of the lungs
aerophagia
cyanosis
frantic attempts to obtain air
Eosinophils are found in bronchial wash fluids of asthmatic cats. Chronic asthma in cats is treated with inhaled or systemic glucocorticoids and bronchodilators (fluticasone, prednisolone, albuterol, theophylline).
Intestinal allergies (food allergies) are principally observed in dogs and cats.
Allergic gastritis manifests by vomiting, which occurs 1 to > 12 times weekly within 1–2 hours of eating. The vomitus may be tinged with bile. In cats, vomiting may be the sole clinical sign; dogs may also have intermittent loose feces. Cats and dogs with allergic gastritis are usually healthy except for vomiting.
Allergic enteritis is associated with a mild inflammation of the small intestine but with little or no eosinophilia. Feces usually are normal in volume and frequency but vary from semiformed to watery. They may be extremely odorous, especially in cats.
Affected animals may be excessively thin despite good appetite. Skin lesions and poor coat are commonly associated with food allergies in cats but less commonly in dogs. The allergy often develops after episodes of viral, bacterial, or protozoal enteritis, a phenomenon known as allergic breakthrough.
Eosinophilic enteritis, the most severe form of allergic intestinal disease, manifests by moderate to severe inflammation of the intestines and a pronounced eosinophilia. Diarrhea, weight loss, and poor coat condition are usually evident.
The prevalence of allergic colitis is greater in cats than in dogs, although in general it is not common. In dogs, it is often associated with frequent defecation and soft, mucus-laden, and sometimes bloody feces; in cats, it most frequently manifests by more normal feces coated or spotted with fresh blood.
Atopic dermatitis is a complex, pruritic, chronic skin disorder that occurs in many species but has been studied mostly in dogs. Some dogs with atopic dermatitis may have a genetic predisposition that leads to excessive production of IgE antibodies. It has been estimated that ~10% of all dogs suffer from atopy, with a breed predisposition in terriers, Dalmatians, and retrievers.
There is increasing evidence that dogs with atopic dermatitis have a skin barrier defect and that most allergens enter through the skin. Atopic dogs often chew at their feet and axillae. Excessive sweating is especially noticeable in hairless areas. The severity of the skin lesions is greatly increased by licking, scratching, flea infestation, and secondary bacterial or yeast (Malassezia) infection. Atopic skin lesions in cats are either miliary (small scabs) and widespread or are larger and more localized. Localized lesions are often pruritic.
In cats, food allergens probably are a more common cause of pruritic skin lesions than are inhaled allergens.
Sweet itch is a seasonal allergic dermatitis of horses associated with certain insect bites, especially night-feeding Culicoides (midges). Intensely pruritic lesions appear along the dorsum from the ears to tail head and perianal area. Similar allergic skin reactions to mosquito bites occur around the ears and face of cats and dogs.
Type II Hypersensitivity Reactions
Type II hypersensitivity reactions result when antibodies attack normal cells. These bound antibodies can then activate the classical complement pathway, resulting in cell lysis, or phagocytosis. One source of these antibodies is cross-reactions. Cross-reactive antibodies can develop during infections. These cross-reactive antibodies directed toward an infectious agent may also bind to normal tissue antigens and trigger antibody-mediated cytotoxicity.
Pathogens such as Babesia or Haemobartonella, which parasitize red cells, trigger an immune response that destroys those cells as part of the protective mechanism. Antibodies against antimicrobials may also cause cell destruction if the drug metabolites bind to erythrocytes. As a result, the cells are destroyed by antidrug antibodies and complement.
The most common manifestations of type II hypersensitivity involve blood cells. These include immune-mediated hemolytic anemia if RBCs are involved, leukopenia involving WBCs, and thrombocytopenia involving platelets. Under some circumstances, a cytotoxic attack on vascular epithelial cells will result in a vasculitis with local vascular leakage.
Bovine Neonatal Pancytopenia in Animals
In 2007, a hemorrhagic disease affecting calves appeared in Europe; later, it came to be known as bovine neonatal pancytopenia. Upon investigation it was found to result from the use of a bovine viral diarrhea vaccine.
The vaccine virus was grown in bovine kidney cells. As a result, it stimulated an antibody response in some vaccinated cows directed against the cell’s major histocompatibility complex (MHC) molecules (1). These antibodies were subsequently concentrated in their colostrum. When the affected cows suckled their calves, the ingested antibodies attacked and destroyed the calves' bone marrow stem cells, resulting in a massive pancytopenia. In the absence of platelets, uncontrolled hemorrhage occurred. The offending vaccine has since been withdrawn.
Type III Hypersensitivity Reactions
A type III hypersensitivity reaction is the deposition of antigen-antibody complexes (immune complexes) in tissues or small blood vessels, which activate complement in situ and cause acute inflammation. This activation results in the production of peptides (complements 3a and 5a [C3a and C5a]) that are chemotactic for neutrophils.
The neutrophils are unable to ingest any complexes that are bound to the blood vessel walls, and they release their granule contents in the tissue. These granules contain enzymes and oxidants that cause severe tissue damage. The most frequently affected sites of immune complex deposition are the joints, skin, kidneys, lungs, and brain.
A prerequisite for the development of immune complex disease is the persistent presence of soluble antigen and antibody. These form insoluble immune complexes that become trapped on the basement membrane of small blood vessels. These antigens may persist for a number of reasons, including chronic infections and certain cancers, especially lymphoreticular neoplasms.
Chronic antigen exposure may also occur with inhaled antigens, and, in such cases, immune complexes can form in the alveolar walls. Lastly, some animals respond to self-antigens, which then act as a source of chronic antigenic exposure. In many cases, the origin of the antigen within these immune complexes cannot be determined.
The location of the immune complexes is largely determined by the route through which antigen enters the body. Inhaled antigens give rise to a pneumonitis, antigens that enter through the skin cause local skin lesions, and antigens that access the bloodstream form immune complexes that are deposited in renal glomeruli or joints.
Clinical signs are therefore variable but may include the following:
fever
cutaneous signs and vasculitis (such as erythema multiforme)
polyarthritis (shifting-leg lameness or painful, swollen joints)
Other clinical signs may include ataxia; behavior changes; renal insufficiency (proteinuria, isosthenuria, polydipsia, polyuria), or nonspecific clinical signs such as vomiting, diarrhea, or abdominal pain.
Diagnosis is based on the exclusion of more common causes of clinical signs. Supporting evidence to confirm the diagnosis may be gathered in several ways:
establishing a temporal relationship if a drug or infectious agent is suspected as the cause
identifying chronic infections or malignancies
performing histopathologic and immunohistochemical examinations of biopsies to identify immune-mediated vasculitides or nephritis
Treatment should include supportive care, removal of the causative agent, or treatment of the underlying disorder, such as the following:
appropriate antimicrobial treatment for bacterial infections
surgical drainage of abscesses or infected tissue
treatment for heartworm disease
withdrawal of the offending drugs
Immunosuppressive therapy may be needed to prevent the continued deposition of immune complexes.
Membranoproliferative Glomerulonephritis in Animals
Membranoproliferative glomerulonephritis is caused by immune complexes that form within the bloodstream and are then filtered out in the glomeruli. In effect, the insoluble complexes collect on the glomerular basement membrane. Depending on their size, they may be deposited on the subendothelial or subepithelial surface of the membrane. Secondary glomerulonephritis occurs as an adverse effect of chronic infectious, neoplastic, or immunologic disorders. Animals with idiopathic glomerulonephritis (> 50% of cases) may develop clinical signs of renal failure if sufficient glomeruli are destroyed.
Hypersensitivity Pneumonitis in Animals
Hypersensitivity pneumonitis is most common in cattle and horses exposed over a long time to antigenic dusts. When inhaled antigens meet circulating antibodies in the walls of the lung alveoli, immune complexes form in the alveolar walls and trigger acute inflammation. The most commonly encountered antigens of this type are those contained in the spores of thermophilic actinomycetes from moldy hay. Inhalation of these spores causes farmer's lung disease in humans and a similar condition in cattle.
Hypersensitivity pneumonitis is characterized by the onset of respiratory distress 4–6 hours after exposure to moldy hay. The most effective treatment is removal of the source of the antigen; otherwise, treatment with corticosteroids may help.
Vasculitis in Animals
Vasculitis mediated by immune complexes occurs in animals, especially dogs and horses. Lesions are most prevalent in the dermis of the distal limbs and mucous membranes of the mouth, particularly the palate and tongue (dogs) and lips (horses). Involvement of the nose, ears, eyelids, cornea, and perineum is less common. Early lesions develop as reddened areas that rapidly form shallow erosions. A scab may form over dermal erosions. Edema of the limbs is common in horses and a less frequent but equally striking clinical sign in dogs.
Vasculitis is a feature of systemic lupus in some animals but is often idiopathic. Drug-induced vasculitis has been well recognized in dogs. The vasculitis is detected on histopathologic and immunohistopathologic examination of superficial and deep biopsies taken from the margins of lesions.
Vasculitis is treated by withdrawal of offending drugs and, if necessary, by immunosuppressive therapy. Glucocorticoids used alone or in combination with other agents such as azathioprine or cyclosporine may be used to treat non-drug-induced cases.
Periarteritis Nodosa in Animals
Periarteritis nodosa, or necrotizing polyarteritis, is a rare disease of domestic animals caused by deposition of immune complexes and inflammation in the walls of small and medium-sized arteries. Among farm animals, it is most common in pigs, usually associated with erysipelas and streptococcal infections, and is attributed to a type III reaction to these bacteria or to their vaccines. Lesions are rarely clinically obvious and are usually found on necropsy.
Periarteritis nodosa has been reported in cats, although it may be mistaken for the noneffusive form of feline infectious peritonitis.
Cutaneous and Renal Vascular Glomerulopathy in Animals
Cutaneous and renal vascular glomerulopathy is a canine disease of unknown etiology. It was first reported in racing Greyhounds in Alabama in the 1980s, hence its colloquial name, Alabama rot. Affected dogs develop ulcers in the mouth, distal limbs, belly, and muzzle, along with a fever and anorexia. Some affected dogs develop acute kidney damage leading to renal failure, as well as a thrombotic microangiopathy resulting in a thrombocytopenia, hemolytic anemia, and eventually multiorgan damage.
The etiology of cutaneous and renal vascular glomerulopathy is unknown. The disease is restricted to certain litters of Greyhounds and Great Danes. The disease trigger is believed to be an infectious or environmental factor that has yet to be identified.
Immune-Mediated Arthritis in Animals
Canine Rheumatoid Arthritis
Canine rheumatoid arthritis is rare in dogs and results from excessive, uncontrolled inflammation around joints that causes joint and bone erosion. It appears to be mediated by immune complex deposition in the synovia that results in the development of a nonsuppurative, proliferative synovitis. This is followed by joint erosion and eventually leads to fibrous ankylosis.
The disease manifests initially as a shifting lameness with soft tissue swelling around involved joints. Within weeks or months, the disease localizes in individual joints, and characteristic radiographic changes develop. The earliest radiographic changes consist of soft tissue swelling and a loss of trabecular bone density in the area of the joint. Lucent, cystic areas may be present in the subchondral bone.
The most prominent lesion is the growth of fibroinflammatory tissue called pannus that causes a progressive erosion of cartilage and subchondral bone in the area of synovial attachments, resulting in loss of articular cartilage and collapse of the joint space. Angular deformities often occur, and luxation of the joint is a frequent sequel. Deformities are most frequent in the carpal, tarsal, and phalangeal joints and less frequent in the elbow and stifle.
An erosive arthritis has also been recognized in cats. It tends to occur in older male cats and frequently is associated with infection with feline syncytia-forming virus. The development of this disease in cats is much more insidious than in dogs.
Canine rheumatoid arthritis responds poorly to systemic glucocorticoids alone. Immunosuppressive agents such as azathioprine, mycophenolate mofetil, cyclosporine, and leflunomide are used with glucocorticoids to treat this disorder; NSAIDs (carprofen, deracoxib, etodolac, firocoxib, grapiprant, or meloxicam) may bring relief but should not be combined with glucocorticoids without a washout period between drugs.
Idiopathic Polyarthritis
A nonerosive polyarthritis of unknown etiology is most common in large dogs, particularly German Shepherd Dogs, Doberman Pinschers, retrievers, spaniels, and pointers. In toy breeds, it is most frequent in Toy Poodles, Yorkshire Terriers, and Chihuahuas, or mixes of these breeds. There is no evidence of a primary chronic infectious disease process or of systemic lupus erythematosus. Arthritis is often the sole manifestation. It is commonly associated with the simultaneous presence of respiratory or GI disease and some neoplasia.
Diagnosis is based on the history of cyclic fever that is unresponsive to antimicrobials, malaise, anorexia, and stiffness or lameness. Bony changes are not evident on radiographs until the disease is well established. Even then, radiographic changes are mild and can mimic degenerative joint disease. Synovial fluid contains leukocytes but is sterile.
Treatment for nonerosive polyarthritis is with daily high-dose glucocorticoids followed by low-dose, alternate-day treatment. Treatment usually can be discontinued after 3–5 months. Dogs that do not respond well to such regimens (> 50%) may be treated with more potent immunosuppressive drugs, such as azathioprine, mycophenolate mofetil, cyclosporine, and leflunomide in addition to glucocorticoids. Gold salts help augment treatment with glucocorticoids in some animals.
Plasmacytic-Lymphocytic Synovitis in Dogs
Plasmacytic-lymphocytic synovitis is possibly a variant of rheumatoid arthritis. It occurs in medium-sized and large dogs. Although multiple joints often are involved, the disease commonly affects the stifle joint. The most common clinical signs are hindlimb lameness and anterior drawer motion of the stifles. Lymphocytes, plasma cells, and neutrophils are present in the synovial fluid, although in some cases the fluid is essentially normal. Examination of the joint shows synovial proliferation and stretching or rupture of the cruciate ligaments. Treatment is as for canine rheimatoid arthritis, discussed above.
Other Type III Reactions
Purpura hemorrhagica of horses is a severe nonthrombocytopenic purpura that often follows a Streptococcus equi infection or vaccination; it occurs when immune complexes of antibody and streptococcal antigen are deposited in vascular basement membranes (see photographs showing edema, ocular lesions, and muzzle with purpura hemorrhagica).


Courtesy of Dr. Thomas Lane.


Courtesy of Dr. Thomas Lane.


Courtesy of Dr. Sameeh M. Abutarbush.
Anterior uveitis ("blue eye") is an immune complex–mediated reaction that frequently occurs in the recovery stage of infectious canine hepatitis. It results from the deposition of immune complexes containing canine adenovirus 1 in the anterior chamber of the eye and cornea.
Equine recurrent uveitis is associated with immunologic responses to Leptospira and Onchocerca spp. This periodic ophthalmia results from autoimmune attack. Antibodies directed against some serovars of Leptospira will cross-react with retinal antigens and trigger severe ophthalmia and retinitis.
Type IV Hypersensitivity Reactions
Type IV hypersensitivity reactions, or cell-mediated inflammatory reactions, occur when antigen triggers local cell-mediated responses. Multiple cytokines are produced, as well as activated macrophages and cytotoxic T cells. The infiltration of mononuclear cells and the release of inflammatory molecules by these cells result in intense local inflammation.
The antigens usually responsible for the development of type IV reactions include intracellular bacteria or parasites, some viruses, reactive chemicals, and (in certain situations) cellular autoantigens.
Allergic contact hypersensitivity is a cell-mediated inflammatory and pruritic response resulting from chemicals reacting with and modifying normal dermal proteins. The modified proteins trigger a cell-mediated immune response, which causes inflammation and damages the skin (eg, poison oak and poison ivy reactions in humans). This reaction has been described in dogs, cattle, and horses and usually occurs as a result of contact with sensitizing chemicals incorporated in plastic food dishes, plastic collars, and drugs placed on the skin. The lesions commonly occur in the skin (allergic contact dermatitis) because the antigen comes into contact with the skin. Examples of antigens that cause type IV responses are metals such as nickel and chemicals that may be on lawns or carpets (these can cause contact dermatitis on the ventral abdomen of dogs that lie on their ventrum on such surfaces).
The diagnosis of a type IV hypersensitivity reaction is based on eliminating other causes of disease and on histology. The goals of treatment are to identify and eliminate the source of antigen responsible for the reaction and to provide anti-inflammatory or immunosuppressive therapy as required.
Granulomatous Reactions in Animals
T-cell–mediated granulomatous reactions may also occur around persistent infectious foci. These reactions to microorganisms, such as mycobacteria, Coccidioides spp, Blastomyces spp, and Histoplasma spp, and possibly feline infectious peritonitis virus, may be a result of chronic cell-mediated immune reactions and localized macrophage activation.
Although cell-mediated immunity effectively controls these types of infections in most animals, for poorly understood reasons, these same mechanisms are only partially effective in others. These granulomatous reactions are characterized by the development of a fibrous stroma and an infiltration of macrophages, giant cells, and lymphocytes around the persistent antigen.
Lymphocytic Choriomeningitis in Animals
Lymphocytic choriomeningitis, a viral infection of mice, results from the destruction of virus-infected cells by T cells, leading to CNS damage and a choriomeningitis.
Old-Dog Encephalitis in Animals
Old-dog encephalitis may also result from cell-mediated immune mechanisms in middle-aged dogs directed against cells persistently infected with canine distemper virus. The initiating canine distemper virus infection may have been clinically inapparent and may precede the development of encephalitis by many years.
Autoimmune Diseases
Along with immunodeficiencies and hypersensitivities, the third type of immunologically mediated disease involves the development of autoimmunity. Autoimmune diseases result when an immune response is directed against normal cellular components.
These diseases may be divided into organ-specific diseases, affecting a single body organ or tissue, and diseases directed against widespread antigens and affecting multiple organ systems.
Autoimmune Thyroiditis in Dogs
Autoimmune thyroiditis in dogs is characterized by destruction of the thyroid gland by an autoimmune process that has both humoral (type II) and cell-mediated (type IV) components. It is particularly prevalent in Doberman Pinschers, Beagles, and Golden Retrievers. Hypothyroidism may be the sole manifestation of the disease.
Autoimmune Adrenalitis in Dogs
Autoimmune adrenalitis has been reported in dogs. The adrenal glands are slowly destroyed by a plasmacytic-lymphocytic infiltrate. When sufficient glandular tissue is destroyed, the dogs develop Addison disease (adrenocortical insufficiency). The condition is sometimes associated with autoimmune thyroiditis.
Dogs may also suffer autoimmune attacks on their parathyroids and their pancreatic islets. Some dogs, such as Italian Greyhounds, may suffer from polyendocrine diseases.
Immune-Mediated Hemolytic Anemia and Thrombocytopenia in Animals
The production of autoantibodies against erythrocyte or platelet antigens results in anemia or thrombocytopenia.
Antibodies and complement attach to RBCs either directly or indirectly via an absorbed antigen and then mediate RBC destruction, resulting in a severe anemia. Concurrent thrombocytopenia occurs in 60% of cases.
Immune-mediated hemolytic anemia (IMHA) can be associated with systemic lupus erythematosus or with lymphoreticular malignancies. Drugs or infections may trigger episodes of hemolytic anemia or thrombocytopenia in many species. More often than not, the initiating cause is unknown.
IMHA occurs in several clinical forms: peracute, acute or subacute, chronic, cold agglutinin disease, and red cell aplasia. Most cases are treatable; however, relapses are common.
Peracute IMHA occurs mainly in middle-aged large-breed dogs. Affected dogs are acutely lethargic and have a rapid decrease in PCV within 24–48 hours, with bilirubinemia, variable icterus, and sometimes hemoglobinuria. Initially, the bone marrow is nonresponsive; however, it may respond within 3–5 days. Thrombocytopenia may also be present. Antiglobulin tests are often negative, and spherocytes may or may not be present, but tube or slide agglutination of RBCs is marked. The autoagglutination is not dispersed by saline dilution, hence the term "hemolytic anemia with in-saline agglutinins." The serum usually contains autoantibodies that cause agglutination of most donor RBCs.
The prognosis of peracute IMHA is poor, even with prompt and vigorous treatment. The most effective treatment involves immediate use of high dosages of glucocorticoids plus an immunosuppressive drug (cyclosporine, mycophenolate mofetil, leflunomide), together with a compatible blood transfusion. Even without transfusion, heparinization may be beneficial for the first 2 weeks or more. Administration of IV immunoglobulin (IVIG) may be of benefit to dogs that do not respond to treatment with a combination of glucocorticoids and immunosuppressive drugs (2, 3, 4).
Acute IMHA is the most common form of the disease, with a breed predilection in Cocker Spaniels. Initial clinical signs are pallor, fatigue, and less commonly, icterus. Hepatosplenomegaly is a prominent clinical sign. The WBC count may be increased due to bone marrow hyperplasia. Autoagglutination of RBCs is uncommon, and the antiglobulin test is generally positive. These patients usually respond well to treatment with glucocorticoids. If a favorable response is not observed within 7–10 days, immunosuppressive drugs (cyclosporine, mycophenolate mofetil, or leflunomide) may be added to the regimen, as well as a third tier of treatment with IVIG for dogs not responding to combination immunosuppressant therapy alone.
Chronic IMHA differs from the acute form in that the PCV falls to a constant level and remains there for weeks or months. The bone marrow is either normal or hyperresponsive, and antiglobulin tests are often negative. Chronic IMHA is relatively more common in cats than in dogs. Usually, the anemia is responsive early in the course of disease but responds minimally or not at all by the time it becomes severe. Initial treatment is with glucocorticoids; if there is no response within 2 weeks, cytotoxic drugs may be added to the regimen.
Cold agglutinin disease is an IMHA of dogs and horses. Its cause is usually unknown; however, it may be secondary to infection, other autoimmune diseases, or neoplasia. The IgM autoantibodies can be agglutinating or nonagglutinating. Complete agglutination does not occur at body temperature but only when the blood is chilled; thus, it is observed more frequently in colder climates and seasons. Initial clinical signs may be of a hemolytic disease; in the agglutinating type, vascular thrombosis may lead to necrosis of the nose, tips of the ears and tail, digits, scrotum, and prepuce. Diagnosis is based on a reversible autoagglutination that occurs only at 4°C. The direct antiglobulin reaction is usually negative for IgG, frequently positive for C3, and usually positive for IgM if the reaction is performed in the cold. In the absence of an obvious initiating cause, such as infection or neoplasia, the disease is best controlled with high doses of glucocorticoids. However, mortality is high.
Red cell aplasia is most common in dogs. It occurs in two forms: one in postweanling to adolescent puppies and the other in adults. Unlike in IMHA, the bone marrow shows a selective depression of erythroid elements; granulocytes and platelets are unaffected. The immune attack is directed against erythroid stem cells; therefore, the peripheral anemia is unresponsive. The antiglobulin test is usually negative. Treatment is usually as for chronic IMHA; however, recovery may be very slow.
Immune-mediated thrombocytopenia is common in dogs. It occurs more often in females than males. The most frequent clinical signs are hemorrhages of the skin and mucous membranes. Melena, epistaxis, and hematuria may be accompanying features and can cause profound anemia. Hemolytic anemia and thrombocytopenia sometimes occur together.
Immune-mediated thrombocytopenia usually is diagnosed on the basis of low peripheral platelet counts despite a pronounced megakaryocytosis in the marrow. Occasionally, megakaryocytes may be selectively absent from the marrow. Tests for antiplatelet antibodies are difficult to conduct, so diagnosis is usually made on clinical presentation and response to treatment.
Patients with immune-mediated thrombocytopenia that show only petechial and ecchymotic hemorrhages, with no appreciable blood loss and megakaryocytes in the marrow, may be treated initially with glucocorticoids. The clinical signs should abate and the platelet count begin to rise after 5–7 days.
If the platelet count has not increased substantially in 7–10 days, mycophenolate mofetil, cyclosporine, leflunomide, or vincristine can be added to the glucocorticoid regimen. Cyclosporine should be used carefully in combination with vincristine because it interferes with metabolism of vincristine and may increase the likelihood of neutropenia and other adverse effects.
In animals with megakaryocytes in the marrow and severe blood loss, a more rapid response to treatment is desirable. Such patients are treated with a single injection of vincristine combined with daily glucocorticoids; a favorable response usually occurs after 3–5 days. If the blood loss is life-threatening, platelet-rich whole blood should be administered. If the platelet count has risen by day 7, remission is maintained on glucocorticoids alone. If there is no response after 7 days, a second dose of vincristine is administered. If the platelet count is still low after 2 weeks, vincristine is discontinued and a potent immunosuppressive agent such as mycophenolate mofetil, cyclosporine, or leflunomide is added.
Animals with thrombocytopenia and no megakaryocytes respond much more slowly to glucocorticoids, or to glucocorticoids and vincristine. Preferred treatment for these patients is with prednisolone and an immunosuppressive agent such as mycophenolate mofetil, azathioprine, cyclosporine, or leflunomide. A response should not be expected earlier than 1–2 weeks after beginning treatment.
Treatment may be discontinued in most animals with immune-mediated thrombocytopenia 1–3 months after the platelet count returns to normal.
Some patients have a persistent thrombocytopenia despite drug treatment, or they can be maintained in remission only with chronic, high-dose treatment. The alternatives are to allow the patient to live with the thrombocytopenia if clinical signs are minimal or to use longterm combination drug treatment with glucocorticoids and either vincristine, mycophenolate mofetil, cyclosporine, or leflunomide.
Splenectomy is another treatment option; it is seldom curative by itself but may allow use of lower and safer dosages of immunosuppressive drugs.
Autoimmune Skin Diseases in Animals
In many autoimmune skin diseases, affected animals make autoantibodies against the intracellular cement proteins in the epidermis. This promotes local proteolysis, leading to separation of the epidermal cells (acantholysis) and the development of vesicles (blisters) within the skin.
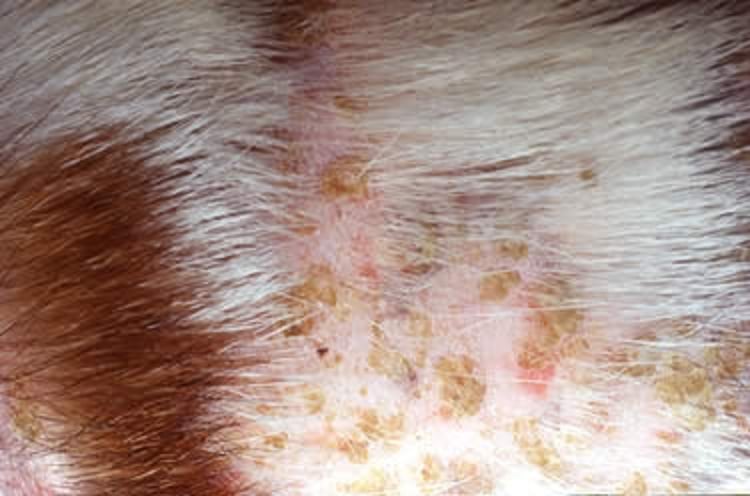
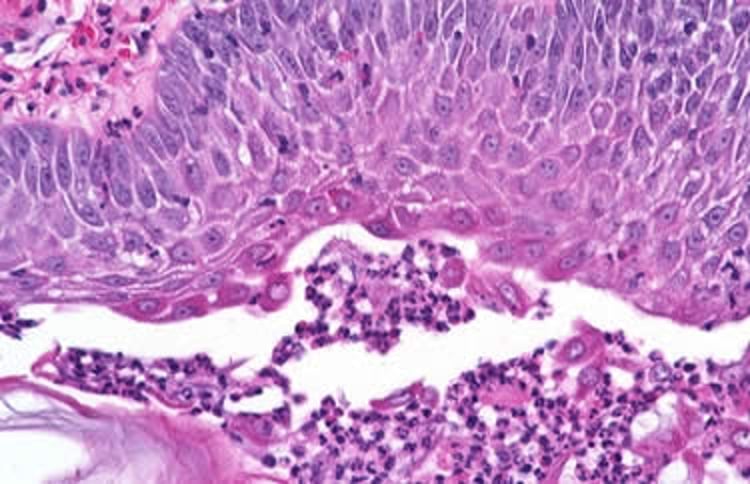
Pemphigus foliaceus is the most common of the ulcerative skin diseases, occurring more often in dogs than in cats and horses. It is characterized by the development of shallow erosions, ulcerations, and thick encrustations of the skin and mucocutaneous junctions (see pemphigus foliaceus photograph and photomicrograph). Autoantibodies in the skin attack the intracellular cement (desmoglein), resulting in its degradation and in the separation of the cornified and uncornified cell layers.
The absence of lesions in the mouth, and the widespread thick, crusty nature of the skin lesions, tend to differentiate pemphigus foliaceus from the much rarer pemphigus vulgaris.
Immunosuppression is required to treat the disease. High doses of glucocorticoids may be used initially; however, low-dose, alternate-day treatment is used once the disease is under control. More potent immunosuppressive drugs such as mycophenolate mofetil, cyclosporine, or leflunomide may be used with glucocorticoids in cases unresponsive to steroids alone. Patients that respond poorly to initial treatment or that require high dosages of drugs to control lesions have a poor longterm prognosis.

Courtesy of Dr. Robert Dunstan.

Courtesy of Dr. Robert Dunstan.
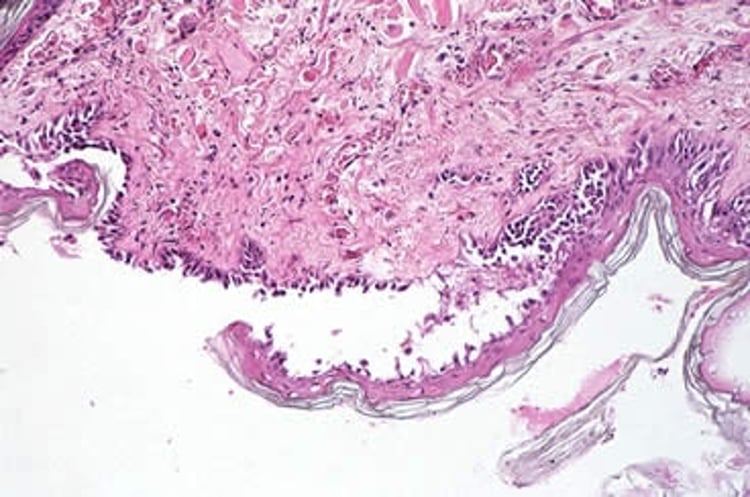
Pemphigus vulgaris is a less common autoimmune skin disease than pemphigus foliaceus. It is characterized by deep vesicle formation along the mucocutaneous junctions of the mouth, anus, prepuce, and vulva, and in the oral cavity (see pemphigus vulgaris photomicrograph). Other areas of the skin are only mildly involved. The vesicles develop as a result of suprabasal acantholysis. Secondary bacterial infection often causes complications. If untreated, the disease is often fatal. It is treated with high doses of glucocorticoids alone or in combination with other immunosuppressive drugs such as mycophenolate mofetil, cyclosporine, leflunomide, or gold salts. Pemphigus vulgaris is difficult to maintain in remission, and the longterm prognosis of affected animals is fair to poor.

Courtesy of Dr. Robert Dunstan.
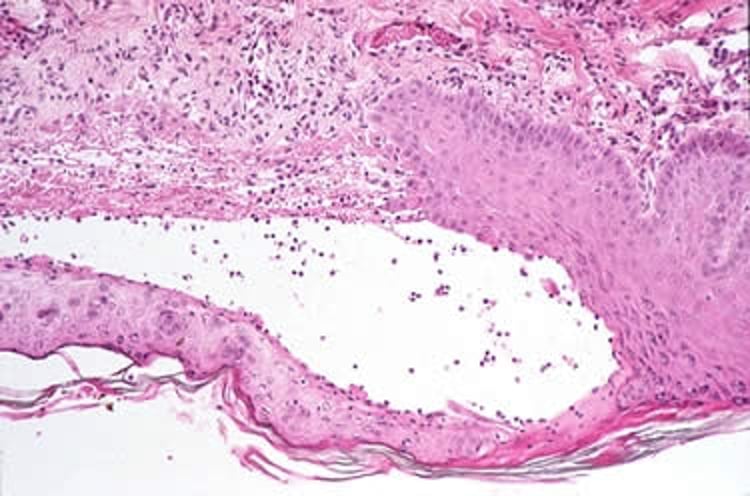
Bullous pemphigoid is a rare canine skin disease recognized most often in Collies and Doberman Pinschers. Lesions are often widespread but tend to be concentrated in the groin. The involved skin resembles a severe scald. Bullae also develop; they are subepidermal and may be full of eosinophils (see bullous pemphigoid photograph and photomicrograph). Autoantibodies against the basal lamina can be detected by immunofluorescence. The treatment of choice is prednisolone and azathioprine used in combination. Remission is frequent; however, continual drug treatment at relatively high dosages may be required to keep the disease under control. The longterm prognosis is poor.


Courtesy of Dr. Robert Dunstan.
Courtesy of Dr. Robert Dunstan.
Myasthenia Gravis in Animals
Myasthenia gravis is an autoimmune disease in which autoantibodies directed against the acetylcholine receptors of muscle cells cause receptor degradation or blockage and thus block neuromuscular transmission. The disease is characterized by extreme generalized muscle weakness and fatigue accentuated by mild exercise. Megaesophagus due to paralysis of esophageal muscles is a frequent primary or accompanying complaint in dogs. Thymomas are often associated with myasthenia gravis in humans but are less common in domestic species. Autoantibodies against the acetylcholine receptors can be detected in the serum of affected animals by an indirect immunofluorescence assay using normal muscle as a substrate.
Administration of a short-acting anticholinesterase drug (edrophonium chloride) produces a dramatic increase in muscle strength; unfortunately, this drug is no longer widely available. Treatment is with long-acting anticholinesterase drugs. Chronic immunosuppressive drug treatment for this disease is logical.
Meningitis of Unknown Origin in Animals
Three immune-mediated types of meningoencephalitis of unknown origin occur in dogs. These are necrotizing meningoencephalitis (NME), necrotizing leukoencephalitis (NLE), and granulomatous meningoencephalomyelitis (GME). The precise form of the disease may be established only by histopathologic examination.
NME has been reported to occur in Pugs, Papillons, Shih Tzu, Cotons de Tuléar, Maltese, Yorkshire Terriers, Pekinese, and Chihuahuas. It is characterized by lethargy and listlessness, followed by seizures with ataxia, head pressing, circling, blindness, and neck pain.
NLE has been reported in Yorkshire Terriers and French Bulldogs. Clinical signs are similar to those of NME, including listlessness, seizures, circling, ataxia, and blindness leading to death.
GME is most common in young adult Poodles and Terriers. Clinical signs include loss of vision, ataxia, nystagmus, seizures, listlessness, and apparent cervical pain. Some may develop a fever accompanied by vomiting or diarrhea.
A syndrome of meningitis, often associated with polyarthritis, occurs in young Akitas. The dogs show severe episodes of fever, depression, cervical pain and rigidity, and generalized stiffness. Affected dogs grow slowly and often appear unthrifty. The condition responds poorly to treatment with glucocorticoids and immunosuppressive drugs. Most affected dogs are euthanized as young adults. A milder and more drug-responsive form of the disease has been reported in older Akitas and may be associated with pemphigus foliaceus, uveitis, and plasmacytic-lymphocytic thyroiditis.
Keratitis Sicca in Dogs
Keratitis sicca is an autoimmune "dry eye" syndrome that occurs in dogs. It can occur in either a primary form or secondary to chronic use of sulfonamides. It results from immune-mediated destruction of the lacrimal glands and is similar to Sjögren syndrome of humans. Affected dogs may respond favorably to cyclosporine eye drops.
Multiorgan Autoimmunity
Systemic Lupus Erythematosus in Animals
Systemic lupus erythematosus (SLE) is a complex autoimmune disease that occurs in dogs. SLE is rare in cats and in large animals. It has two consistent immunologic features: disseminated immune complex disease and a tendency to produce multiple autoantibodies. Clinically, it reflects a combination of type II and III hypersensitivities.
Antinuclear antibodies (ANAs), or antibodies against nucleic acids, are the diagnostic hallmark of SLE; however, in many individuals, antibodies against RBCs, platelets, lymphocytes, clotting factors, and thyroglobulin are also present. The presence of ANAs can be diagnostic of the disease.
Either the immune complex or the autoantibody component of the disease tends to predominate in a given animal. Immune complex deposition may lead to the following:
synovitis and polyarthritis
dermal reactions
oral erosions and ulcers
myositis
neuritis
meningitis
arteritis
myelopathy
glomerulonephritis
pleuritis
Autoimmune hemolytic anemia, thrombocytopenia, or both are the most common presentations of SLE in animals. Glomerulonephritis is one of the major, life-threatening complications of SLE in cats.
SLE is characterized by the presence of ANAs, and tests for these or the associated lupus cells may help in diagnosis. However, some healthy animals may have ANAs, and not all animals with SLE have detectable ANAs in their blood. Diagnosis of SLE must therefore be based on the entire clinical syndrome—not just on the presence or absence of ANAs.
SLE usually can be treated with glucocorticoids. Initially, they are used in high daily doses, and when remission occurs, alternate-day, low-dose treatment is used. Drug treatment should be continued for 2–3 months after all clinical signs have resolved. Immunosuppressive agents, such as cyclosporine, mycophenolate mofetil, and leflunomide, are used in combination with glucocorticoids in patients with SLE that is difficult to control with glucocorticoids alone.
References
Deutskens F, Lamp B, Riedel CM, et al. Vaccine-induced antibodies linked to bovine neonatal pancytopenia (BNP) recognize cattle major histocompatibility complex class I (MHC I). Vet Res. 2011;42(1):97. doi:10.1186/1297-9716-42-97
Swann JW, Garden OA, Fellman, CL, et al. ACVIM consensus statement on the treatment of immune-mediated hemolytic anemia in dogs. J Vet Intern Med. 2019;33(3):1141–1172. doi:10.1111/jvim.15463
Bestwick JP, Sharman M, Whitley NT, et al. The use of high-dose immunoglobulin M-enriched human immunoglobulin in dogs with immune-mediated hemolytic anemia. J Vet Intern Med. 2022;36(1):78-85. doi:10.1111/jvim.16315
Kane B-K, Greer RM. Human intravenous immunoglobulin use for hematological immune-mediated disease in dogs. J Am Vet Med Assoc. 2023;261(7):1004-1010. doi:10.2460/javma.23.01.0043
For More Information
Also see pet health information regarding disorders involving anaphylactic reactions in dogs and anaphylactic reactions in cats.







