




Caseous lymphadenitis is a chronic, infectious disease that manifests clinically as abscesses of peripheral (external) and/or internal lymph nodes and organs. The characteristic purulent material is very thick and nonodorous. The peripheral form presents as abscesses of single or multiple palpable lymph nodes. The internal form typically manifests as chronic weight loss and ill thrift. Culture of active lesions for Corynebacterium pseudotuberculosis is diagnostically definitive. Affected animals are often culled. If treatment is pursued, it consists of consistent, sustained antimicrobial administration to decrease the numbers of active draining lesions, as well as isolation from other herdmates until lesions are dry and/or resolved.
Caseous lymphadenitis (CL) is a chronic, infectious disease due to Corynebacterium pseudotuberculosis. Although the prevalence of CL varies by region and country, it is found worldwide and is of major concern for small ruminant producers in North America.
CL is characterized by abscess formation in or near major peripheral lymph nodes (external form) or within internal organs and lymph nodes (internal form). Although both forms of CL occur in both sheep and goats, the external form is more common in goats, and the internal form is more common in sheep.
Economic losses from CL include death, condemnation, and trimming of infected carcasses; hide and wool loss; loss of sales for breeding animals; and premature culling of affected animals from the herd or flock.
Once established on a farm or region (endemic), CL is maintained primarily by contamination of the environment. This contamination results from active draining lesions, from nasal discharge or coughing by animals with the internal form of the disease, or from the ability of C pseudotuberculosis to survive harsh environmental conditions.
Because of the zoonotic potential of CL, care should be taken when handling CL-infected animals or purulent exudate from active, draining lesions.
Etiology and Pathogenesis of Caseous Lymphadenitis
C pseudotuberculosis is a gram-positive, facultative, intracellular coccobacillus. Two biotypes have been identified based on the ability of the bacteria to reduce nitrate: a nitrate-negative group that infects sheep and goats, and a nitrate-positive group that infects horses.
Isolates of C pseudotuberculosis from cattle are a heterogeneous group. All strains produce an exotoxin, called phospholipase D, that enhances dissemination of the bacteria by damaging endothelial cells and increasing vascular permeability.
C pseudotuberculosis has a second virulence factor, which is an external lipid coat that provides protection from hydrolytic enzymes in host phagocytes. The bacteria replicate in the phagocytes, which then rupture and release the bacteria. The ongoing process of bacterial replication, followed by attraction and subsequent death of inflammatory cells, forms the characteristic abscesses associated with CL.
To establish infection, C pseudotuberculosis must penetrate skin or mucous membranes. The most common site of entry is the skin after an injury that may result from shearing, tagging, tail docking, castration, or other environmental hazards. Contact with purulent material draining from open, active lesions is the most common source of bacteria through these breaches in the skin.
Although less common, entry across mucous membranes from inhalation or ingestion of the bacteria is another means of infection by C pseudotuberculosis.
After entering the body, the bacteria move to the lymph nodes via the regional draining lymphatic system. Internally, the bacteria establish infection not only in the lymph nodes but also in the viscera. The incubation period varies from 1 to 3 months, culminating in the development of encapsulated abscesses.
C pseudotuberculosis is hardy in the environment and can survive on fomites such as bedding and wood for 2 months and in soil for 8 months. The presence of organic material, shade, and moisture enhance survival of the organism.
Clinical Findings of Caseous Lymphadenitis
The hallmark clinical finding in cases of external caseous lymphadenitis is the development of abscesses in the region of peripheral lymph nodes. Common sites of development include the submandibular, parotid, prescapular, and prefemoral nodes. Less commonly, abscessation of supramammary or inguinal lymph nodes occurs, in addition to an occasional ectopic location along the lymphatic chain.


Courtesy of Dr. Kevin Washburn.


Courtesy of Dr. Kevin Washburn.


Courtesy of Dr. Kevin Washburn.
If left untreated, CL lesions eventually mature into open, draining abscesses. The purulent material from these lesions has no odor and varies in consistency from soft and pasty (more common in goats) to thick and caseous (more common in sheep). After natural draining, the skin lesion heals with scarring.
Recurrence of CL lesions is common, often months later. CL should be highly suspected in a sheep or goat with abscessation in regions previously affected by CL. Although other bacteria may cause abscessation in these locations (and in other animals), if there is any prior diagnosis of CL within a herd or flock, these cases should be handled as recurrent CL until proved otherwise.
The internal form of CL usually presents as chronic weight loss and failure to thrive. The presence of other clinical signs depends on the organs of involvement, which may include any of the major organ systems.

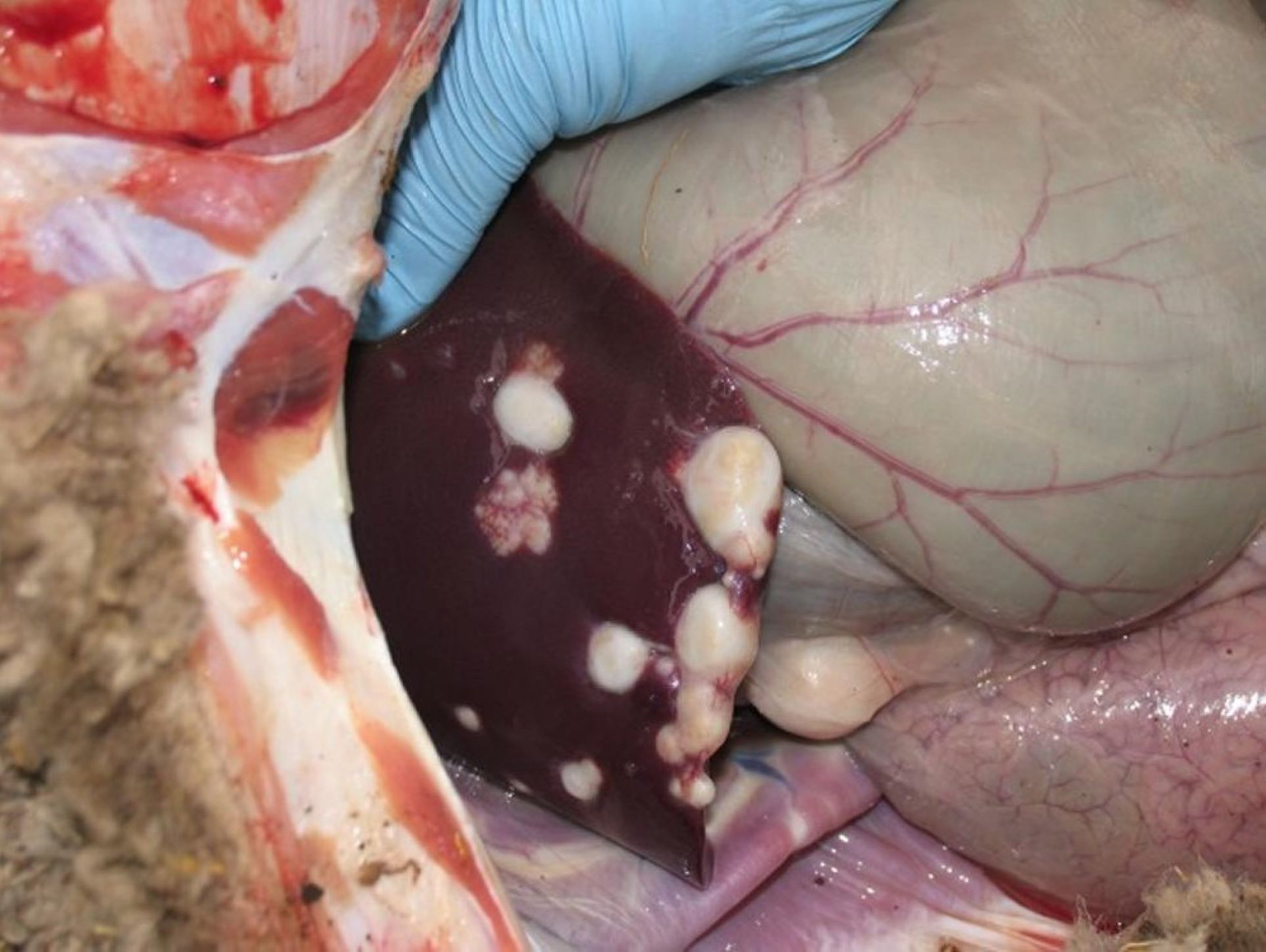
Courtesy of Dr. Kevin Washburn.


Courtesy of Dr. Sameeh Abutarbush.

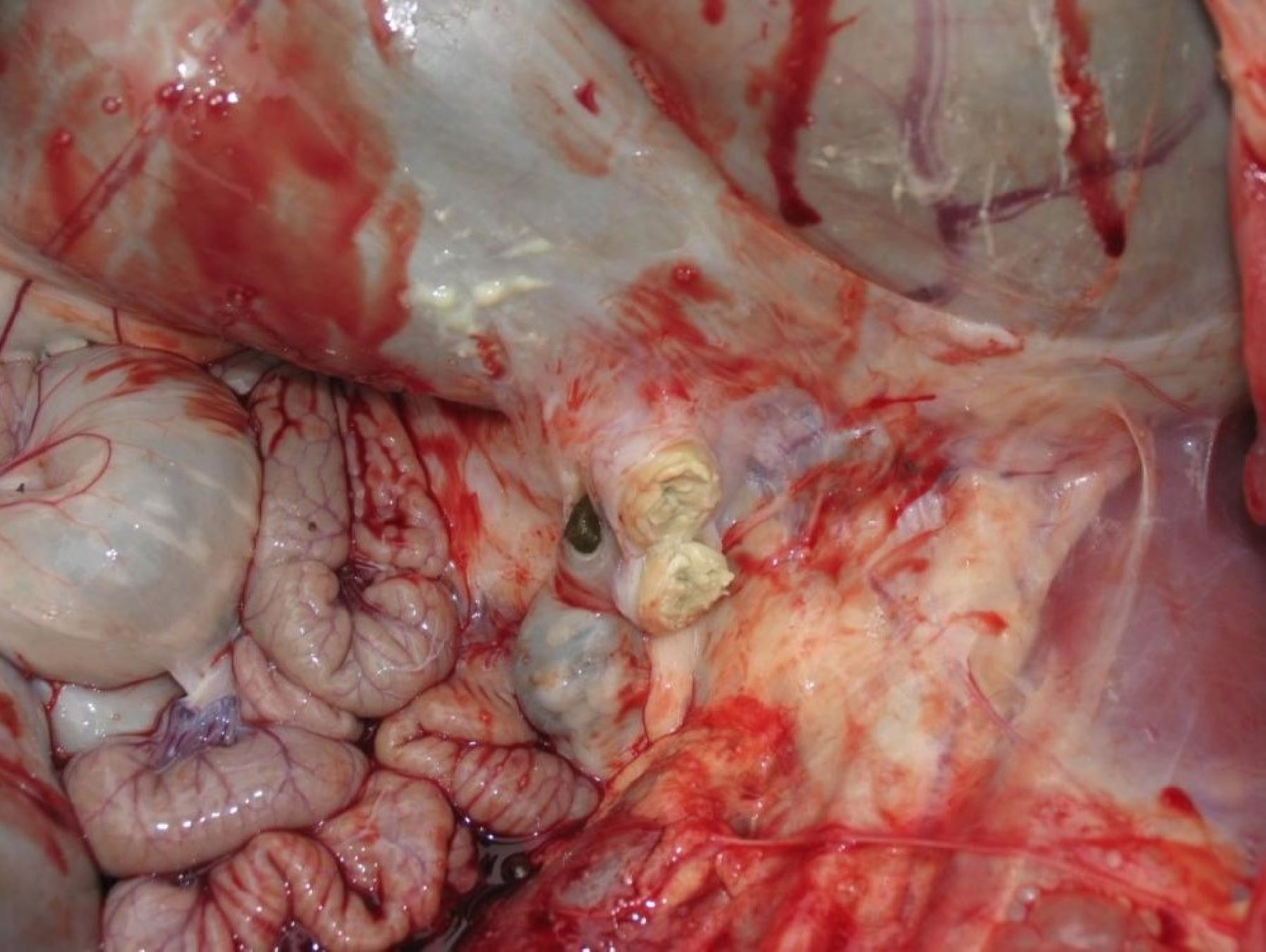
Courtesy of Dr. Kevin Washburn.
Lung abscessation is a common form of visceral involvement in internal CL; therefore, signs of chronic ill thrift with cough, purulent nasal discharge, fever, and tachypnea with increased lung sounds may be noted. The internal form is more common in sheep and has been termed “thin ewe syndrome.”
The incidence of abscesses and development of clinical signs with either the external or internal form of CL increase with age.
Diagnosis of Caseous Lymphadenitis
Physical examination of lesions associated with lymph nodes
Bacterial culture of suspected lesions
Serologic testing
The presence of an external abscess on a small ruminant is highly suggestive of caseous lymphadenitis, especially in the peripheral lymph nodes. However, definitive diagnosis is only by bacteriologic culture of purulent material from an intact abscess.


Courtesy of Dr. Kevin Washburn.
Although other pyogenic organisms, such as Trueperella pyogenes (formerly Arcanobacterium pyogenes), Staphylococcus aureus, Pasteurella multocida, and anaerobes such as Fusobacterium necrophorum, can cause abscessation, affected animals should be kept isolated pending culture results.
Animals with visceral abscesses pose a greater diagnostic challenge with CL.
Radiography and ultrasonography can be useful to detect internal lesions.
Culture of a transtracheal aspirate obtained from an animal with pneumonia can help determine whether CL is the cause.
Exclusion of other causes of chronic weight loss and ill thrift in the face of proper nutrition and good appetite, such as Johne’s disease, parasitism, and poor dentition, further raises suspicion.
If abscesses are not accessible for sampling and bacterial culture, definitive diagnosis of active cases of CL is challenging. Although many diagnostic tools are available, results of these tests must be interpreted with caution and with consideration of herd or flock history, the presence or absence of active infection within the herd or flock, and vaccination status.
A synergistic hemolysin inhibition (SHI) test that detects antibodies against the phospholipase D exotoxin is available at many diagnostic laboratories. Positive titers indicate past resolved CL infections, recent exposure, recent vaccination, or active lesions or their development. Titers of 1:256 or higher have been correlated in past studies with the presence of active, developing abscesses; in a more recent study, however, a high titer was poorly correlated with the presence or development of abscesses over an 18-month period (1).
When the status of an animal with a positive CL titer is in doubt, the titer should be repeated in 2–4 weeks.
If the titer is rising and clinical signs of abscesses are noted, then CL can be assumed to be the cause.
False-negative results are possible if testing is done in the first 2 weeks after exposure before the animal has seroconverted. In addition, animals with chronic, walled-off abscesses can have a false-negative result.
Colostrum-derived titers are usually present until 3–6 months of age, so the results of serologic testing of lambs or kids < 6 months old should be interpreted with caution.
Treatment and Control of Caseous Lymphadenitis
Treatment
Antimicrobials (intralesional and/or systemic)
Supportive care
Once a diagnosis of caseous lymphadenitis has been established, owner education stressing the persistent, recurrent nature of the disease is necessary.
The most practical management approach for commercial animals infected with CL is to cull them from the herd or flock. However, animals with draining abscesses should not be sent through sale barns until draining has ceased and the wound has healed.
Treatment of individual animals should be undertaken with the understanding that CL is not considered a curable disease. Animals with genetic or emotional value are treated mainly for aesthetic reasons and to limit their infectivity to the rest of the herd or flock.
Options for treating CL have included lancing and draining, surgical excision, formalin injection of lesions, systemic antimicrobials, and intralesional antimicrobials.
If external abscesses are lanced and drained, the cavity should be lavaged with dilute iodine solution and the animal isolated in an area that can be disinfected until the lesion stops draining and heals. Drainage material should be carefully collected and disposed of to minimize environmental contamination.
Dilute bleach and chlorhexidine solutions are effective disinfectants of hard surfaces and fomites. However, because the presence of organic material on these surfaces inactivates them, the surfaces should be cleaned before being disinfected.
Intact accessible abscesses can be surgically removed; however, this option is more expensive, and undetected abscesses are often present and continue to develop. Recurrence rates with either lancing or surgical removal are high.
The practice of injecting abscesses with formalin should be strongly discouraged, because the FDA bans extra-label use of potent carcinogens in food-producing animals.
The efficacy of treating CL with systemic antimicrobials and, more recently, intralesional antimicrobials has been investigated. Note, however, that the administration of any antimicrobial for treatment of CL is extra-label; therefore, strict adherence to published guidelines on withdrawal times and an established veterinarian-client-patient relationship are mandatory.
Longterm administration of procaine penicillin G and rifampin has been successful in some cases of CL. Penicillin alone, although effective in vitro, is unlikely to penetrate the capsule of developed abscesses; the same is true of many water-soluble or moderately lipid-soluble antimicrobials.
The highly lipid-soluble property of tulathromycin may be particularly helpful in cases of internal CL, when abscesses are not accessible for other forms of treatment.
Studies have shown that extra-label administration of either one dose of tulathromycin at 2.5 mg/kg, SC directly into the abscess cavity, or two doses of tulathromycin at 2.5 mg/kg, injected at the same time, one SC and one intralesionally, can resolve CL lesions without the abscess having to be lanced (2). Further, effective concentrations of tulathromycin can be achieved within walled-off abscesses that are due to C pseudotuberculosis after a single dose at 2.5 mg/kg, SC (2).
Another study by the same investigators found that one 20 mg/kg dose of oxytetracycline injected directly into tissue cages inoculated with C pseudotuberculosis eliminated bacterial growth in these chambers within 48 hours. However, a single 20-mg/kg dose of oxytetracycline, IM, did not eliminate the growth of C pseudotuberculosis in inoculated tissue cages (3).
Despite the efficacy of intralesional and parenteral administration of tulathromycin and oxytetracycline in many CL cases, recurrence remains a problem. Therefore, these drugs cannot be considered curative; however, they can be an acceptable alternative for managing cases of CL when culling from the herd or flock is not acceptable to the owner.
Control
Strict biosecurity measures
Elimination of diseased animals from the herd or flock
Vaccination
Disinfection of shearing equipment and other instruments used in production procedures (castration, ear tagging, etc) between animals
Removal of hazards in the environment that could potentially injure the skin
Prepurchase examination for lesions, serologic screening, and quarantine before introduction of new animals
Because of the nature of the causative organism, common means of exposure, chronicity of the disease, and difficulty in completely eliminating the organism from individual animals, control of CL focuses on strict biosecurity measures.
The overriding goals of any control program are to eliminate CL from the herd or flock and to decrease the number of new cases arising either from transmission of the disease within the farm or from introduction of the disease to the farm.
Ideally, animals identified as infected with CL should immediately be culled. If immediate removal is not possible, infected animals should be isolated from the rest of the herd or flock. Diligence in this practice will eventually result in decreased prevalence as animals that develop active cases are identified and removed, as long as no new animals incubating the disease are introduced to the premises.
When elimination through culling is not a viable option for the owner, control of CL is challenging at best. Dividing the herds or flocks into clean and infected groups and eliminating older and less genetically valuable animals over time is one control strategy.
Lambs and kids from dams infected with CL can be raised on pasteurized colostrum and milk away from infected animals. However, the internal form of CL and animals incubating the disease can still maintain infection within the "clean" group, thereby limiting the success of this approach.
Vaccination
Commercial CL vaccines are currently licensed for use in sheep and goats. These vaccines should be used only in the species for which they are labeled, because adverse reactions have been reported in goats administered vaccines labeled for sheep.
Rigidly adhering to vaccination schedules according to the manufacturer's labeling can help decrease the prevalence and incidence of CL within herds or flocks. However, the efficacy of these vaccines is not 100%, and vaccination will not clear infected animals.
Vaccination of young replacement animals should be considered, and older infected animals should be gradually culled as economics allow. Once CL has a low prevalence rate in the herd, vaccination should be stopped and all seropositive unvaccinated animals culled. In clean herds or flocks (those with no history of CL), vaccination is not recommended.
Prevention of Transmission
The risks of CL transmission among animals should be recognized when shearing or dipping, and management practices should be adjusted accordingly.
Animals with noted CL lesions should be shorn last.
Clipper blades should be disinfected between animals.
Shearers should understand the hazards associated with contacting purulent material and potentially acting as mechanical vectors, either on clothing or via equipment, for transmission of the bacteria to new animals.
Dipping-tank solutions should be kept as fresh as possible, because C pseudotuberculosis can survive within them and serve as a source of infection of freshly shorn sheep that have skin abrasions.
Owners should remove hazardous items (barbed wire, exposed nails, rough feeders) from the environment to decrease injury and potential CL transmission from these fomites.
Prevention of Introduction
One of the most common ways CL can be introduced into a previously disease-free herd or flock, or reintroduced to one in which CL has been decreased or eliminated, is through the addition of replacement animals. Often, animals from other farms that are clinically normal on arrival are incubating the disease and then manifest infection weeks to months later.
Purchasing animals from sources with unknown histories is hazardous to maintaining a clean herd or flock. Newly arrived animals should be examined thoroughly for clinical signs of CL, such as abscesses or scars near peripheral lymph nodes. They should remain isolated from the rest of the herd or flock until their serologic status is determined, and only animals that are seronegative with no evidence of present or past CL lesions should be allowed to enter the herd or flock.
Key Points
Caseous lymphadenitis is a chronic disease that is challenging to eliminate within an individual animal or herd.
The internal form of caseous lymphadenitis manifests as chronic weight loss, is difficult to definitively diagnose antemortem, and serves as a reservoir of infective animals within the herd or flock.
Culling affected animals is the best way to eliminate caseous lymphadenitis from the herd or flock.
When pursued, treatment includes abscess drainage, systemic and intralesional antimicrobials, and isolation.
Before introduction to the herd or flock, new animals should be examined, serologically tested for CL, and quarantined.
References
Washburn KE, Bissett WT, Waldron DF, Fajt VR. Serologic and bacteriologic culture prevalence of Corynebacterium pseudotuberculosis infection in goats and sheep and use of Bayesian analysis to determine value of assay results for prediction of future infection. J Am Vet Med Assoc. 2013;242(7):997-1002.
Washburn KE, Fajt VR, Lawhon SD, Adams LG, Tell LA, Bissett WT. Caprine abscess model of tulathromycin concentrations in interstitial fluid from tissue chambers inoculated with Corynebacterium pseudotuberculosis following subcutaneous or intrachamber administration. Antimicrob Agents Chemother. 2013;57(12):6295-6304. doi:10.1128/AAC.00936-13
Washburn KE, Fajt VR. Oxytetracycline concentrations in interstitial fluid from tissue chambers inoculated with Corynebacterium pseudotuberculosis after intramuscular or intrachamber administration in sheep. Am J Vet Res. 2019;80(6):586-594. doi:10.2460/ajvr.80.6.586







