

Cytology is a useful clinical tool for investigation of disease processes, and the techniques and their interpretation have developed into an entire discipline. This discussion is a brief guide to enable practitioners to prepare samples and undertake basic interpretation; it refers mostly to small animals, but the basic principles apply to all species.
Cytology should be considered a guide. Characteristics of the cells may not be sufficient in many instances to yield a definitive diagnosis or indicate the probable behavior of the lesion. These may require examination of the overall architecture of the tissue, for which cytology is not appropriate. If complex, expensive, or life-threatening therapy is being considered, then the diagnosis should if possible be confirmed by histology.
Techniques
Full cytologic interpretation requires a good quality sample. A substantial minority of samples collected by practitioners are unsuitable for full interpretation. The technique appears to be simple, but consistently obtaining good-quality samples requires practice. If samples are sent to a laboratory for interpretation, sending more than one is recommended. In addition, staining and examining one of the preparations in-house helps to monitor the quality of the samples taken and make a provisional diagnosis. This requires a good staining technique and a good quality microscope with a range of objectives, including oil immersion.
Staining:
The stains and techniques used for cytology preparations in a practice setting are the same as those used for hematology preparations. The traditional stains for cytology preparations are modified Wright stain (Wright-Giemsa) and May-Grunwald Giemsa. Over the past few years, good-quality rapid Romanowsky stains have been developed for cytology and hematology and are often used by veterinary diagnostic laboratories. Many different brands of rapid stain have been developed, so trying a number of products to see which stain is best suited to a practice is recommended. Poor preparations are not always the fault of the collection technique; the stain may be the problem. Stains deteriorate with use and require regular renewal. Many slides can be adjusted by returning a finished stained slide to the stain for deeper color reaction, or if overstained, can have some color removed by placing the slide in alcohol. Formalin-fixed cytology preparations must be stained with either H&E or Papanicolaou stain. If samples are sent to a laboratory for interpretation, the submission form should indicate whether formalin has been added.
Fine-needle Aspiration:
The aim of fine-needle aspiration is to obtain a high cell harvest with minimal artifactual damage or blood contamination. The basic sampling kit consists of 21- and 25-gauge needles and 3-, 5-, and 10-mL syringes. Precise technique and choice of equipment depends on physical characteristics of the lesion and whether blood contamination is a problem.
The basic technique uses a 25-gauge needle and a 10-mL syringe. The needle is inserted into the lesion and repeatedly redirected to sample a number of areas while applying a small amount of suction on the syringe. Suction is released before withdrawing the needle. If suction is continued on withdrawal, the cell sample is violently sucked into the barrel of the syringe, causing cell rupture. Sample size is often very small and may be present only within the lumen of the needle and not in the syringe. When the sample has been obtained, the syringe is removed, filled with air, reattached, and used to gently express the sample onto a clean, dry, glass slide. Expressing the sample forcefully will rupture cells. Another slide is placed on top of the sample and pulled lengthways to spread the sample to a monolayer. Additional pressure should not be applied, because this also may cause rupture of the cells. Thicker areas are not a concern; the edges will often be thin enough to examine individual, nonoverlapping cells. The sample should be air dried as quickly as possible to reduce the effects of shrinkage; a hair dryer can be used for this purpose, but heating the sample must be avoided.
This technique can be adapted to different situations. If blood contamination is a problem, the size of the syringe and amount of suction can be reduced or the syringe removed altogether. This is particularly a problem with bone marrow aspiration but is common with all cytology samples and is thought to be due to excessive suction on the syringe. If blood contamination is unavoidable, the blood can be centrifuged. However, if the sample is directly smeared, a feathered edge should be examined, because this is where the heavier cells from the tissue tend to congregate. Blood contamination can often be decreased with the use of a very fine needle (25 gauge); this increases the chance of collecting enough cells for interpretation.
An alternative technique uses a needle without a syringe; no difference in the cell harvest between these two techniques has been shown. The needle is inserted without the syringe and repeatedly redirected to sample different depths and directions within the lesion. The cells are detached by the cutting edge of the needle and enter the needle lumen by capillary action. After withdrawal of the needle, a syringe containing air is reattached and used to gently express the sample. This technique is also particularly useful to sample fragile cells, such as lymphoid cells from lymph nodes. A far better cell harvest is obtained from splenic lesions with this technique than by applying suction. In addition, there is greater sensitivity in placement of the needle, which is especially useful for small lesions.
Certain tissues tend to give a very low cell harvest. These are usually composed of mesenchymal cells (connective tissue) that tightly adhere to each other and therefore do not exfoliate easily. For these lesions, a larger bore needle and increased suction may be necessary. However, a needle with a bore >21 gauge tends to provide a tissue core more suitable for histologic interpretation than cytology.
Impression Smears:
Impression smears are often used for ulcerated surface lesions. They are of limited value, because they usually sample only the surface inflammatory exudate and rarely include cells from deeper tissues. A better use of this technique is at the time of biopsy to allow an immediate assessment of the lesion before fixation and processing of the tissue sample. The cut surface of the excised sample is blotted a number of times to remove surface blood and serum, and the dried surface is applied to a clean, dry slide with gentle pressure. A number of areas can be prepared on a single slide. The preparations should be quickly air dried and then stained.
Body Fluid Evaluation:
Once a body fluid (eg, urine, pleural or peritoneal fluid) is obtained, a cytospin preparation is by far the best method of cell concentration. However, few practices have access to a cytospin, so centrifugation of the preparation and sampling of the centrifuged sediment is the usual method of cell concentration. Once the slide has been prepared, it should be rapidly air dried before staining.
If the fluid is to be sent to a laboratory, adding a few drops of formalin (the concentration is not critical) helps preserve cells and prevent bacterial overgrowth during transit. Severe bacterial overgrowth obscures the cells, and their metabolic products tend to destroy cells in cytology preparations. This is particularly useful for bronchoalveolar lavage samples and urine, which often contain infectious agents and are prone to bacterial contamination at sampling. The laboratory must be advised of the presence of formalin, which excludes the use of Romanowsky stains. Adding EDTA to help preserve cytology samples is often recommended, but the effect is minimal.
Cells in CSF samples degenerate very quickly and are usually present in very low numbers. Cytospin preparations are almost essential for CSF examination; this can usually be achieved only in a reference laboratory. The addition of a few drops of 10% formalin preserves the cells in CSF very well during transit.
Interpretation of Cytology Samples
Cytology interpretation can be guided by an algorithm that also covers the common questions asked by clinicians. From a clinical viewpoint, it is often not necessary to complete all stages of this algorithm. For example, a simple differentiation of inflammation from neoplasia may be sufficient to allow a decision on the next stage of case management. Full cytology interpretation may require the services of a diagnostic laboratory, and a definitive diagnosis often requires histopathology. Some lesions cannot be definitively diagnosed by cytology. If in doubt or if the cytologic interpretation does not correlate with the clinical picture, histology is essential for full interpretation. Whenever the diagnosis is in doubt, biopsy is indicated.
Cytology algorithm
Algorithm to interpret cytology samples. |

Inflammation:
Recognition of basic inflammatory cells—neutrophils, eosinophils, lymphocytes, macrophages, and plasma cells—is essential for interpretation of cytology samples. Some tumors contain a large number of inflammatory cells, but these are very uncommon, even when there is tumor necrosis. The presence of only inflammatory cells in a sample usually indicates a primary inflammatory lesion. Ulceration produces inflammation on the surface of neoplastic lesions, but even in this case the inflammatory cells typically do not extend deeply into the underlying neoplasm. A small percentage of mast cell tumors, however, are composed almost entirely of inflammation, hemorrhage, and edema with only a small number of mast cells. These can be difficult to identify even by histology.
Neutrophils:
These are the first cells to arrive in an area of inflammation, and they continue to be attracted to the site as long as the inflammatory stimulus lasts. Large numbers of neutrophils indicate acute inflammation and often are accompanied by smaller numbers of macrophages. This pattern is most often caused by infection or foreign body reaction, including furunculotic reactions directed against hair and keratin embedded in the soft tissue. If fluids are not examined immediately, bacteria, if present, will begin to proliferate, but phagocytosis of bacteria does not occur after sampling. Therefore, if the bacteria are truly pathogenic, they should be within the cytoplasm of the phagocytic cells. The cells’ cytoplasm may contain RBCs, tissue debris, or foreign material.
Macrophages:
Macrophages arrive at a site of inflammation within 2–3 hr and are not necessarily an indicator of chronicity, although they often increase with time. They phagocytize bacteria and also larger structures, such as fungi, cellular debris, and foreign material. These cells are often associated with tissue destruction.
Macrophages come from circulating monocytes and have variable morphology. In the tissue, the cytoplasm greatly enlarges over time and usually becomes vacuolated. The nuclei become rounded. If a macrophage exhibits vacuolation or phagocytosis, it is often described as activated. They can be multinucleated, especially with foreign body reactions and in longstanding lesions. Under certain circumstances, they may become epithelioid. These cells have oval or round nuclei and small, often indistinct, nucleoli. Their cytoplasm is expanded but uniformly stained and not vacuolated. They can look epithelial, and great care must be taken when interpreting such cells. However, they do not normally form clusters, which is a key factor in differentiation from epithelial cells.
Macrophages are almost always seen in bronchoalveolar lavage fluid (they come from the alveoli) and body cavity fluids (part of the modification process), joints (a normal component but increased in disease), and cyst contents (a nonspecific reaction).
Eosinophils:
Eosinophils have segmented nuclei and eosinophilic cytoplasmic granules. They vary slightly between species and are generally slightly larger than neutrophils. In cytology preparations, it can occasionally be difficult to distinguish poorly stained eosinophils from neutrophils, because the granules can become indistinct and the cytoplasm of degenerating neutrophils become more acidic, giving a more eosinophilic staining reaction. They are often seen in association with mast cells. Eosinophils are associated with allergies and also are prominent in parasitic diseases, superficial cutaneous viral infection in cats, and fungal infections. They are the predominant cell type in specific eosinophilic conditions such as eosinophilic granuloma in cats (rarely in dogs), canine eosinophilic folliculitis and furunculosis, and eosinophilic collagenolytic granuloma in horses. Some cases of canine cutaneous mast cell tumors have a very high proportion of eosinophils and very few mast cells (<5% of cases).
Of the most commonly encountered veterinary species, rabbits and guinea pigs have inflammatory cells equivalent to neutrophils in other species, but have eosinophilic cytoplasmic granules. These are called heterophils. They can be difficult to distinguish from eosinophils. The cellular equivalent to neutrophils in birds and reptiles are also heterophils with eosinophilic granules.
Lymphocytes:
Lymphocytes are usually small with very little cytoplasm and smudged chromatin with no nucleoli. The almost-round nuclei are similar in size to those of red cells. RBCs are often present in cytology preparations, where they can be used as a comparative and absolute scale. RBCs vary slightly with species; in dogs, RBCs are ~7 microns in diameter. Medium and large lymphocytes, which have a slightly more open chromatin pattern and more cytoplasm, can also be seen in inflammatory processes. Along with plasma cells, lymphocytes are part of the chronic inflammatory response and tend to arrive in tissue a few days after the acute inflammation has begun. However, they are not specific for a particular stimulus and are mostly small lymphocytes. If mostly medium to large cells are present, lymphoma is a possibility. However, even large lymphoblastic cells can be seen in low numbers in inflammatory processes. Normal and reactive lymphocytes in body fluids often appear larger than the same cells from soft tissue.
Multinucleated Cells:
These cells are large and have larger numbers of nuclei with one to three small nucleoli and vacuolated cytoplasm. They develop from macrophages (see above) and tend to appear late in the course of inflammation. The cytoplasm should be examined for the presence of fungal organisms and for foreign material. These cells are usually seen in small numbers mixed with other inflammatory cells as part of a granulomatous reaction. Multinucleated cells are much less specific in birds and reptiles, in which they are common in many focal inflammatory lesions, irrespective of cause, and can appear quite early in the inflammatory process.
Fibroblasts:
Fibroblasts are not inflammatory cells, but they are frequently seen in association with inflammation. They will proliferate as part of the repair reaction associated with any tissue damage and appear in an inflammatory lesion after ~2 days. Classically, fibroblasts and fibrocytes are elongated cells with pointed tails of cytoplasm. They have round or oval nuclei, indistinct nucleoli, and moderate amounts of uniform, pale blue-staining cytoplasm. The cytoplasmic boundaries are indistinct, giving a “wispy” appearance. When fibroblasts are aspirated from tissue, the cells often become round and lose their spindle shape, but a small number, especially cells in groups, retain their elongated shape. Reactive fibroblasts cannot be definitively distinguished cytologically from low-grade spindle cell tumors. If found in association with inflammatory cells, spindle cells are most often reactive. If found in large clumps with no apparent stimulus, they are more often neoplastic (but neoplasia cannot be excluded). Because fibroblasts and fibrocytes are the principal connective tissue cell, they are tightly adherent to each other, and cell harvest tends to be low.
Neoplasia:
Inflammatory lesions are characterized by cells from different populations. The presence of cells that are predominantly of the same population indicates normal tissue, hyperplasia, or neoplasia. Ideally, the first stage in evaluation of a cytologic sample for neoplasia is to determine the tissue type from which the cells have come. If this is not possible, it is necessary to simply determine the likely behavior of the cells. This can often be done without specifically identifying the cell type. The following checklist includes features that can be examined to determine tissue type and likely behavior of the lesion: 1) cell numbers, 2) cell distribution within the smear, 3) cell shape, 4) nucleus:cytoplasm ratio, 5) pleomorphism (both nuclear and cytoplasmic), 6) number, shape, and size of nucleoli, and 7) cytoplasmic content such as melanin, metachromatic granules, fat, etc. Classification of the cell type and likely behavior may require a tissue biopsy. With few exceptions, histology will be necessary for a definitive diagnosis and is always necessary to assess mitotic index and to grade a tumor.
There are three basic tissue types: epithelial, mesenchymal (supporting or connective tissue), and round cells.
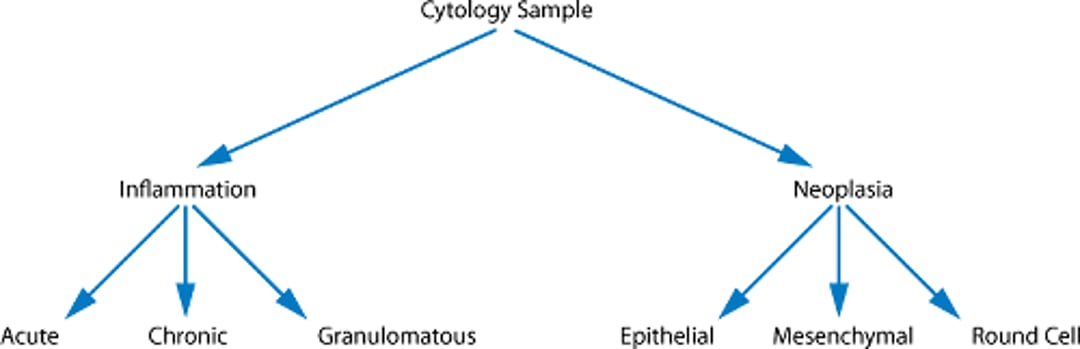
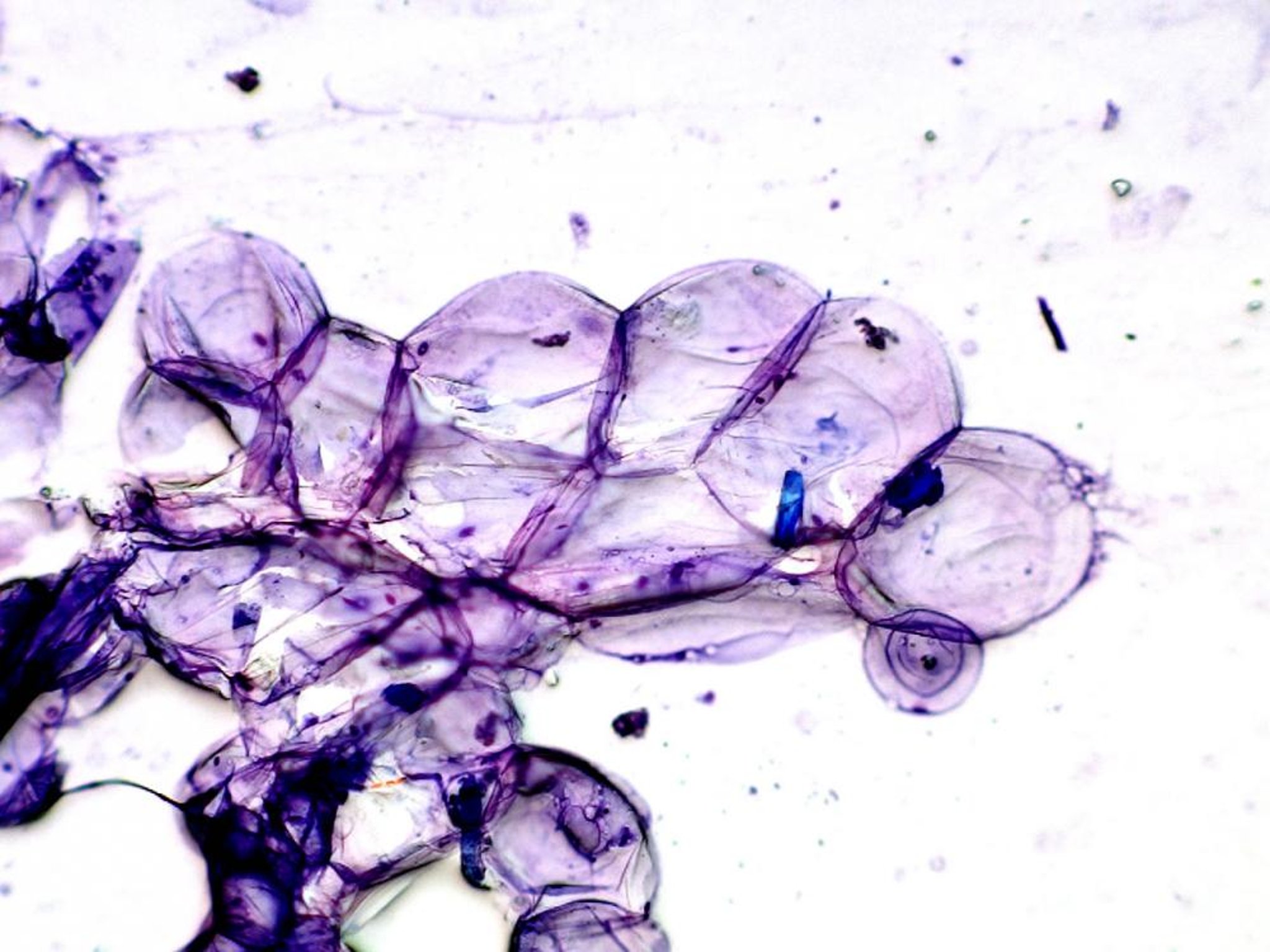
Epithelial Cells:

These polygonal epithelial cells are sticking together in clusters. Cell boundaries are distinct. The purple "wisps" are contents of ruptured, smeared, and stretched nuclear material, which is a common artifact.
Courtesy of Abbey Veterinary Services.
Epithelial cells are round, cuboidal, or polygonal and tend to adhere tightly to each other and exfoliate in clusters or sheets. They have a sharp cytoplasmic outline and exfoliate in moderate numbers. Cells with more than one nucleus are uncommon.
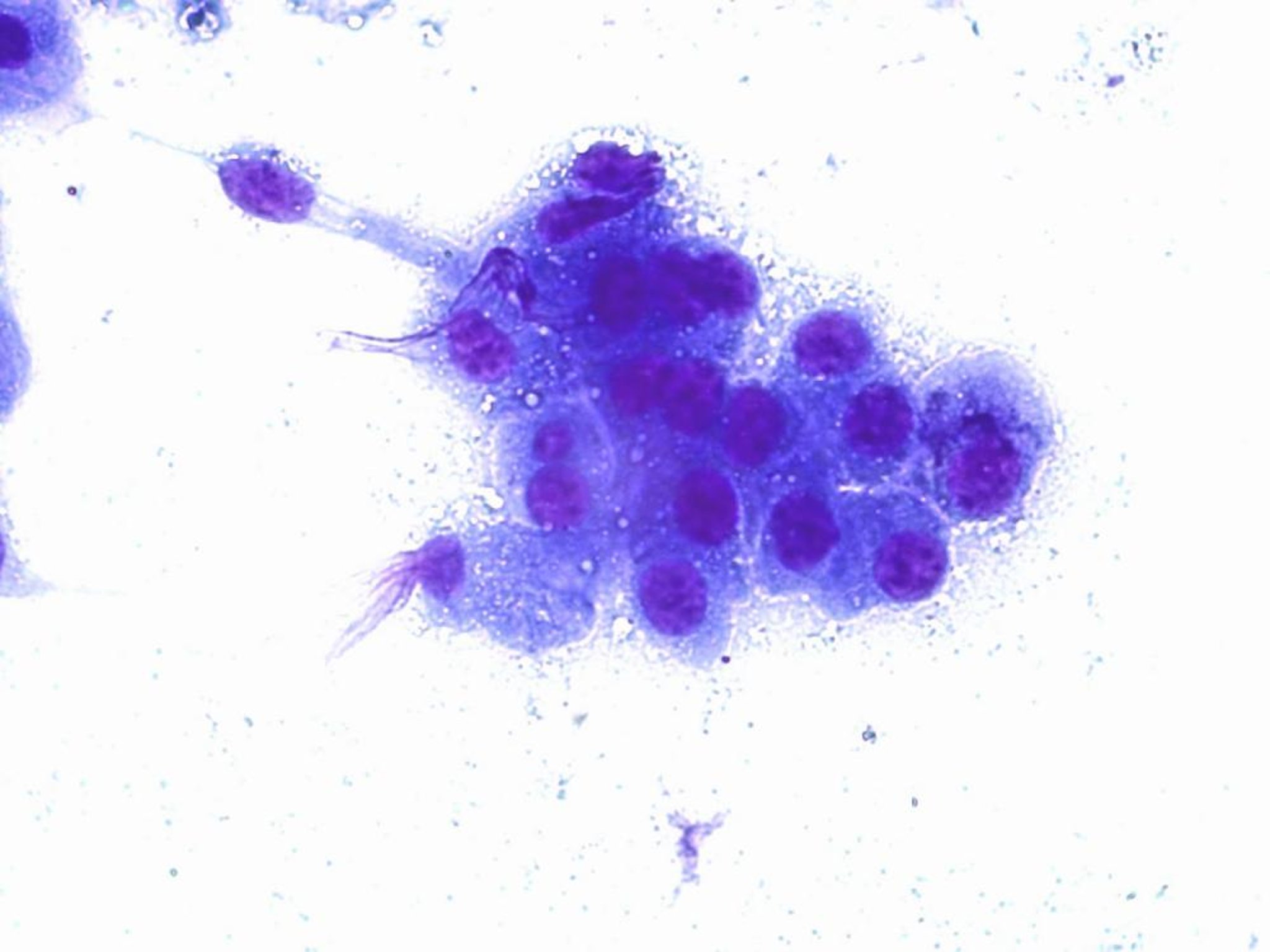
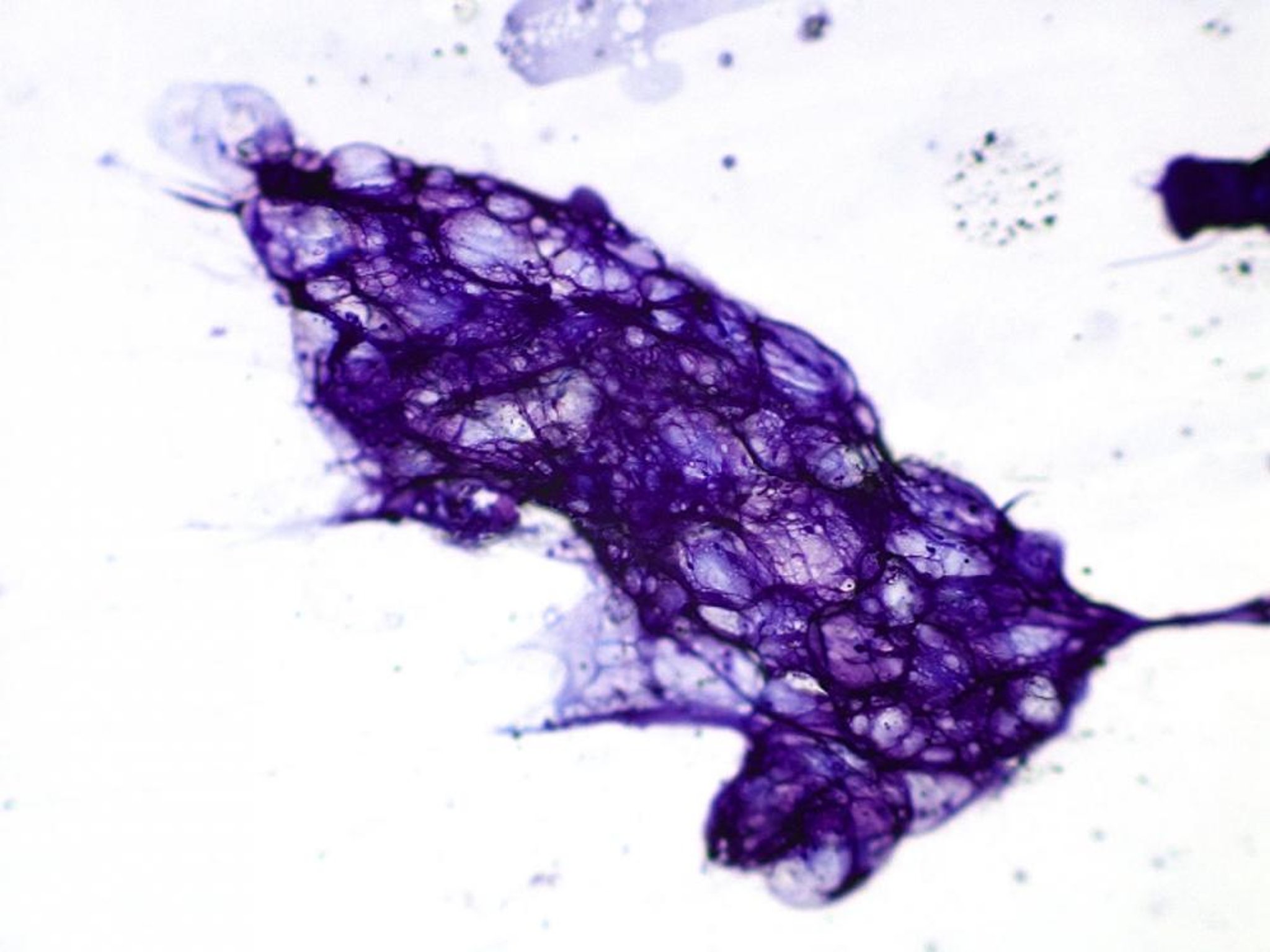
Mesenchymal Cells:
Mesenchymal, or spindle, cells lie singly in low numbers. They do not have sharp cytoplasmic boundaries, and the cytoplasm is slightly elongated and spindle shaped.
Courtesy of Abbey Veterinary Services.
Mesenchymal cells are tightly adherent and usually exfoliate in low numbers as single cells or small aggregates. They are classically spindle shaped but usually round up and become plump when removed from the body, particularly when they are lying singly within the smear. The spindle shape is often more apparent in small aggregates. They tend to appear “wispy” because of indistinct cytoplasmic boundaries. Binucleate cells are not uncommon.
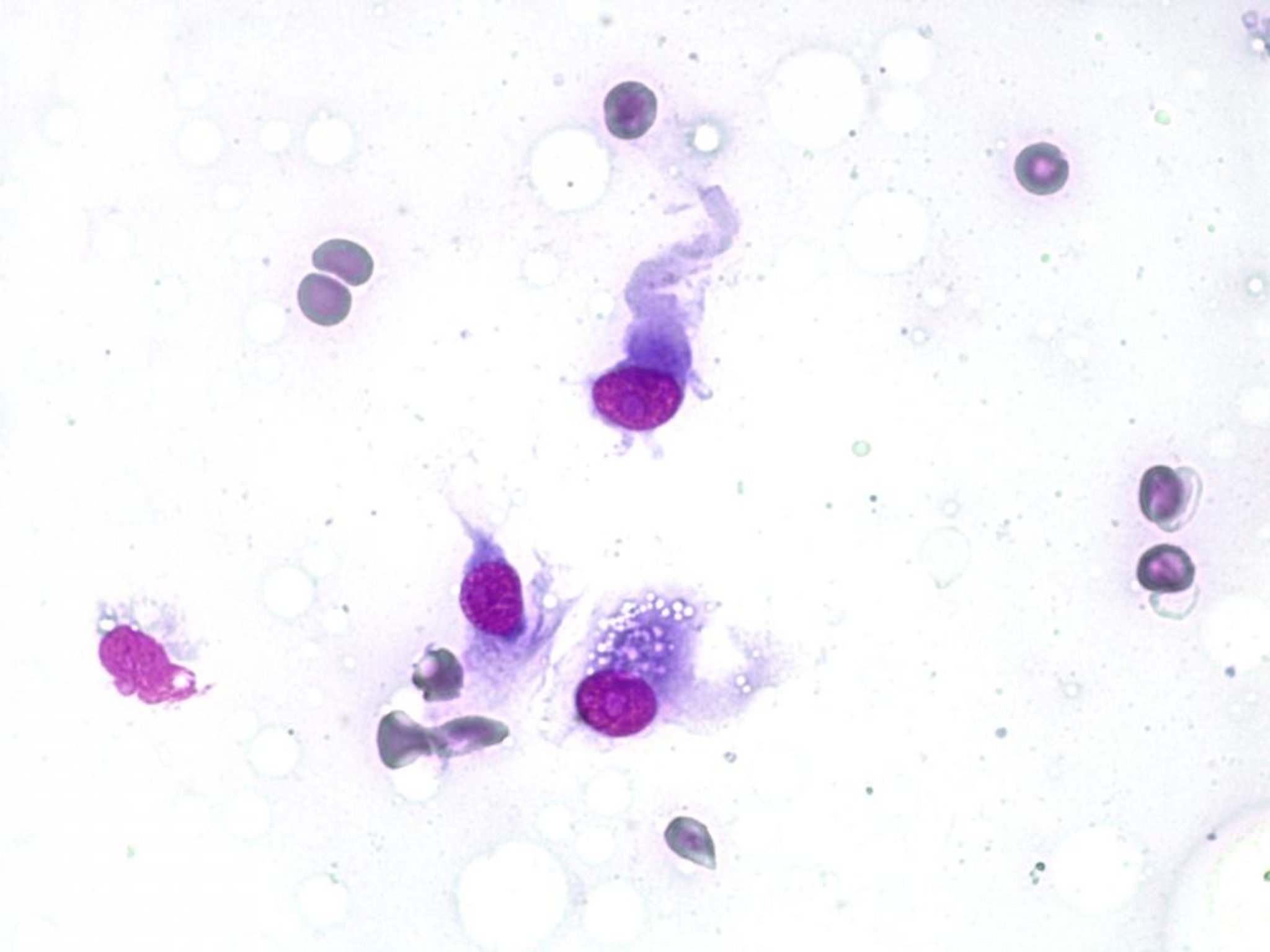
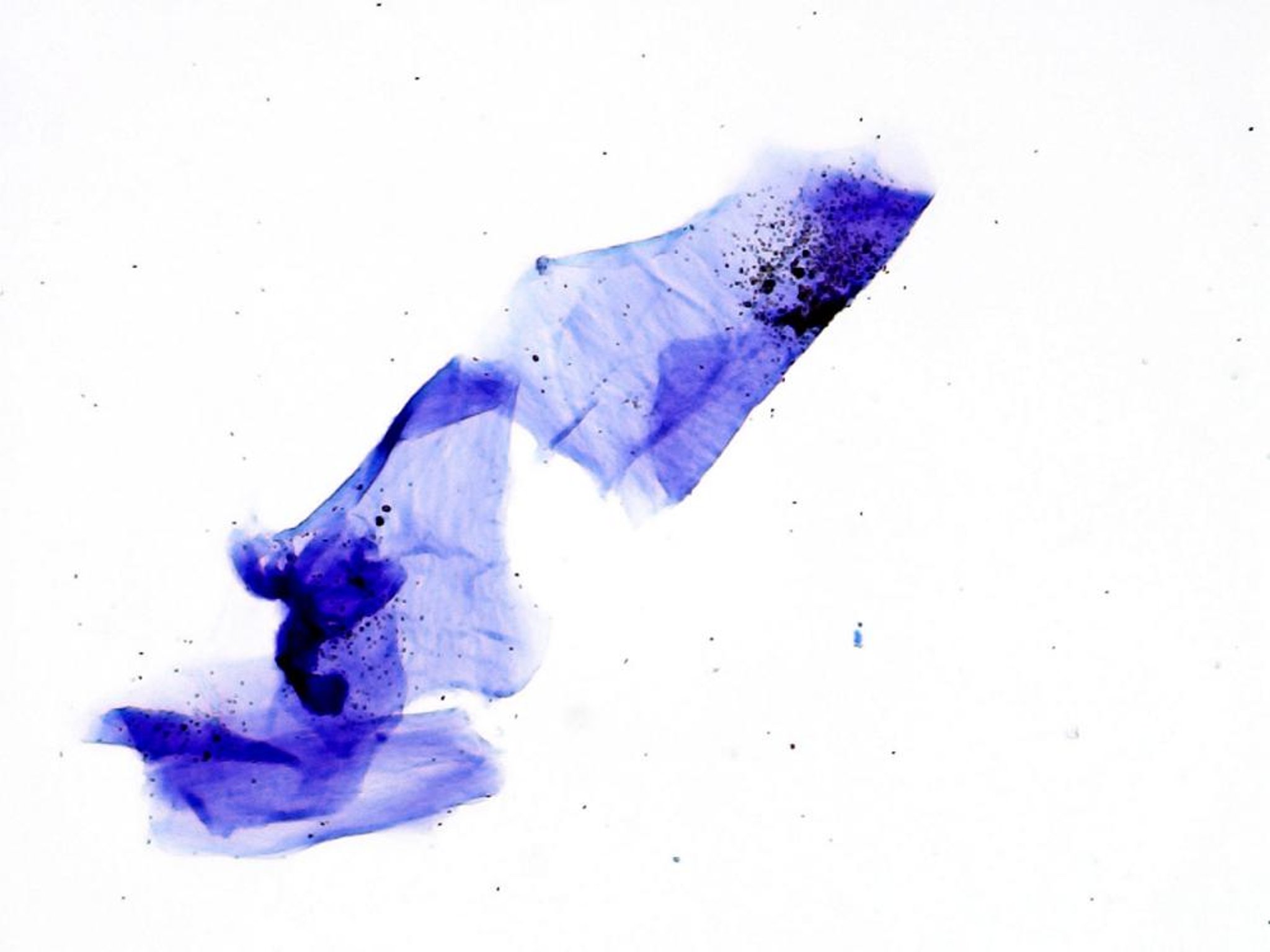
Round Cells:
Within the usual blood contamination, there are cells that are well separated and nonadherent; this is typical of round cell tumors.
Courtesy of Abbey Veterinary Services.
Round cells have little or no adherence in the body. They typically exfoliate in large numbers and lie individually in the smear without clumping. Cells of this category include mast cells, lymphocytes, histiocytes, plasma cells, and cells of transmissible venereal tumors.
Tumor Evaluation:
To distinguish benign from malignant tumors, the amount of variation in certain characteristics within the cell population must be assessed. In general, the more malignant the cell, the less differentiated it becomes and the more variation there is in the cell morphology. Benign tumors have cells that are often uniform in size with a uniform nucleus:cytoplasm ratio; they strongly resemble or are identical to the cell of origin. The more malignant the cells become, the more variation is seen in these criteria. Nuclear criteria are the major indicators of malignancy.
Criteria for malignancy include the following: variation in cell size and shape, increased cell exfoliation, increased nuclear size, increased nucleus:cytoplasm ratio, variation in nuclear size and an increase in multinucleated cells, increased mitosis with abnormal mitotic figures, a coarse and often clumped chromatin pattern, altered shape of the nucleus due to close approximation of a nucleus from an adjacent cell (nuclear moulding), and large and often multiple nucleoli of irregular and abnormal shape. There are a number of exceptions to these indicators; in such situations, histology is essential for full interpretation.
The following are some exceptions to the rules of interpretation:
Thyroid carcinomas usually have fairly uniform, well-differentiated cells. A diagnosis of carcinoma can be made simply on the size of the mass in dogs (tumors >3 cm are automatically considered malignant) but not in cats. Major features of malignancy, such as capsular, soft-tissue invasion and vessel invasion, can only be identified histologically. Other tissues in which it may be impossible to differentiate benign from malignant cells include apocrine gland carcinomas, basal cell tumors, melanomas, and proliferative lesions of the liver.
Unlike most malignant tumors, lymphoma is commonly characterized by a uniform population of cells that are larger than normal lymphoid cells. Therefore, variation in morphology is not necessary for a diagnosis of malignancy with this tissue type. If there is marked variation and small lymphocytes are present, then that is more typical of hyperplasia.
Some normal structures, such as hepatoid glands, have more than one cell type (reserve and terminal cells) and can therefore show variation in morphology, and benign tumors of hepatoid glands can have a similar mixture. Nuclear morphology, however, maintains benign features.
Many mammary tumors can show marked variation in cell morphology but histologically would be classified as benign. Indicators of mammary tumor behavior are architectural features, such as local tissue invasion and invasion of vessels. These cannot be assessed using cytology. These exceptions often make cytologic interpretation unreliable, particularly for these types of tissues.
Most spindle cell tumors do not metastasize but are locally aggressive and often difficult to remove. The criteria for malignancy are often less important with respect to the behavior of these tumors than for the epithelial tumors.
Common Cytology Results:
Some specific features of cytology preparations can provide a more accurate interpretation of the sample. Listed below are some common results and their interpretation.
Mature Fat Cells:
These typical balloon-like fat cells are characteristic of benign lipoma and mature body fat. Both involve the same cells and cannot be distinguished on cytology.
Courtesy of Abbey Veterinary Services.
This is a common presentation of fat cells for both lipoma and mature body fat. The cells are folded and overlapping and less distinctly balloon-like.
Courtesy of Abbey Veterinary Services.
Mature fat cells are seen in benign lipomas and mature body fat. It is not possible to differentiate these cytologically. Fat cells are mesenchymal cells, and because they tend not to exfoliate well, they are usually present in low numbers. If a sample has come from the center of a nodular mass, fat cells are diagnostic for lipoma. These clear-staining, balloon-like cells are often in clusters, folded, and overlapping.
Spindle Cells:
It is usually not possible to differentiate reactive spindle cells from those of spindle cell neoplasia. Indicators of neoplasia include absence of a reactive stimulus, such as inflammation or hemorrhage, and a higher cell population with more numerous and larger clumps of cells. Greater variation in cell morphology indicates more aggressive behavior. When removed from their tissue, they often round up and can be mistaken for round cells, but there are usually some distinctly spindle cells in most preparations.
Keratin:
These terminally differentiated keratin flakes are seen as irregular polygonal sheets like tissue paper with no nuclei. The dark dots are melanin pigment granules.
Courtesy of Abbey Veterinary Services.

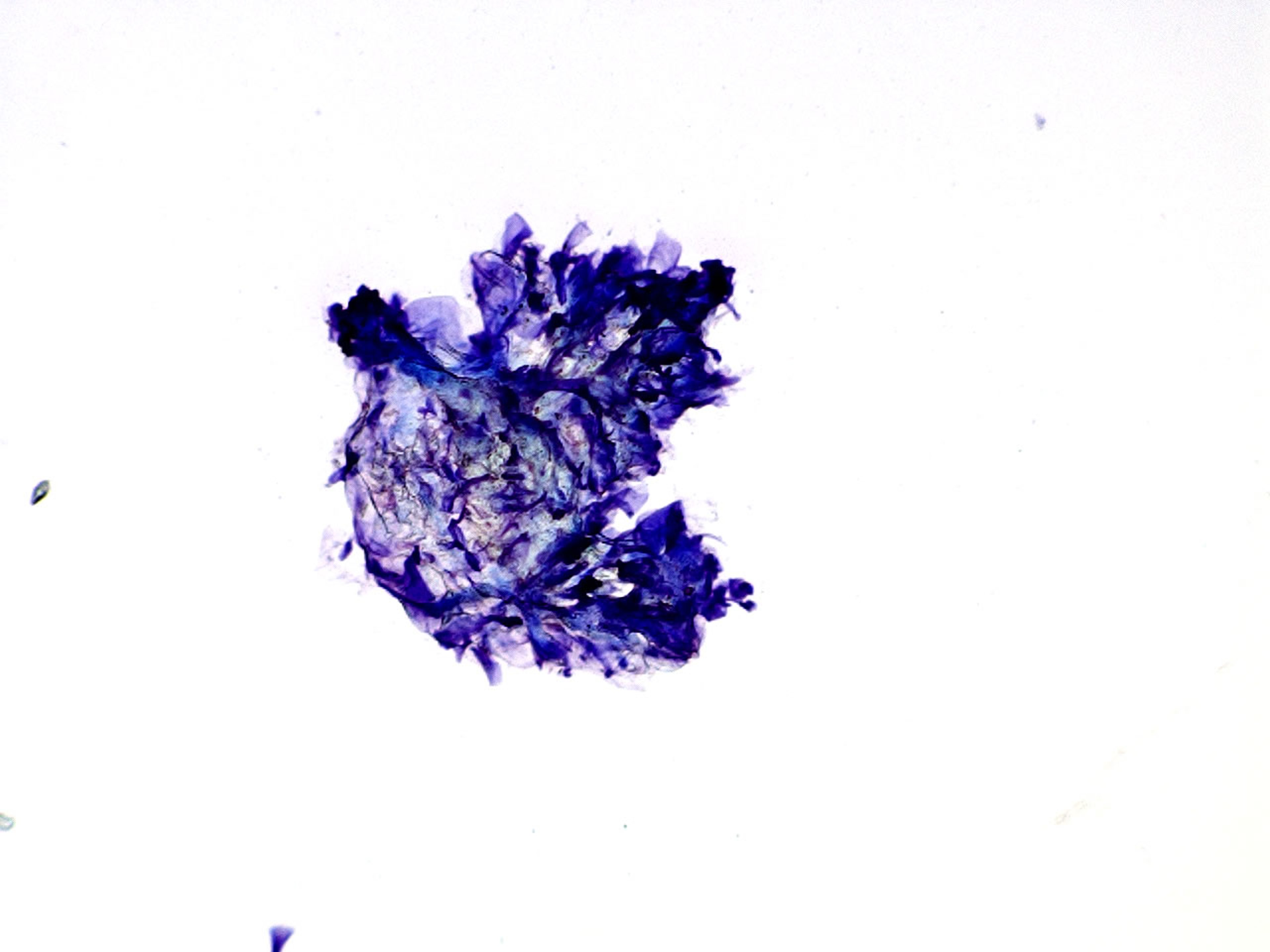
This mass of keratin flakes has much overlap and little individual identity, which is a common finding on cytology. If there are many large clumps, this is likely to be a real change such as the content of a keratin-filled cystic lesion rather than contamination. Again, there are no nuclei.
Courtesy of Abbey Veterinary Services.
Keratin includes nucleated and terminally differentiated non-nucleated squamous epithelial cells. Keratin can be a contaminant from the surface of the skin of the animal or the skin of all handlers of the sample and is a common artifact. It can also be sampled from cutaneous keratin-filled cysts, which are always benign and very common, particularly in dog skin. Large, densely packed clumps of keratin in restricted areas in the center of the slide suggest that keratin is not an artifact but has been sampled from the lesion.
Blood:
Blood is a common artifact of fine-needle aspiration but can also come from blood-filled spaces in tissue. These can be non-neoplastic, such as hematomas, aneurysms, or severe bruising, or neoplastic lesions such as hemangiomas and hemangiosarcomas. The presence of spindle cells does not adequately differentiate neoplastic from non-neoplastic causes of hemorrhage ( see Tumor Evaluation:). Spindle cells produce the neoplastic blood vessels in hemangiosarcomas, but especially in young dogs, they can occasionally produce a very cellular capsule to a soft-tissue hematoma. The capsule contains very active fibroblasts, but they are not neoplastic. Blood that has come directly from the vascular system normally contains significant numbers of platelets. Using a 25-gauge needle can help decrease blood contamination. Blood is almost always seen in aspiration from parenchymatous organs, such as the liver, spleen, kidneys, and bone marrow.
No Cells:
Lack of cells is a common problem of fine-needle aspiration. If the technique is practiced properly, absence of cells can indicate mesenchymal cell proliferation (including lipomas), because these structural cells within the body are tightly adherent cells that do not exfoliate well.
Cells with Cytoplasmic Granules:
The most important type among cells with cytoplasmic granules is the mast cell, given that mast cell tumors are common in dogs. These are medium-sized cells with round nuclei. With Romanowsky stains, the granules are dark blue or purple, small (about the size of bacteria), and usually found in large numbers in the cytoplasm. Less-differentiated mast cells have fewer granules. Cytology cannot be used to grade mast cell tumors; grading always requires histology, because it does not depend on only cell morphology. The cells are fragile, and often there are large numbers of granules in the background that have been released from damaged cells. In dogs, eosinophils are often present and very occasionally can be the dominant cell type; however, they are less common in other species. Mast cell tumors in horses have similar cytology to those in dogs, but in cats the cells in mast cell tumors are often smaller, more uniform, and have less distinct granulation.
Thyroid cells can also have dark granules, usually blue or black. These tyrosine granules are very small, low in number, and can be difficult to see. Larger black granules are associated with melanomas. Cytology cannot differentiate benign from malignant melanomas; however, melanomas on haired skin in dogs are usually benign and those on nonhaired areas, such as the lips, feet, and mouth, are usually malignant. Basal cell tumors also often contain cells with melanin, especially in cats. These tumors are usually benign and cytologically can sometimes be difficult to distinguish from melanomas. Melanin can also be seen in macrophages (melanophages), sometimes in large amounts, but it is usually in much larger clumps within the cytoplasm rather than fine granules that are seen in melanocytes. Very fine magenta granules can sometimes be seen in osteoblastic cells from osteosarcoma. Golden, granular material accumulates in the cytoplasm of macrophages when there has been hemorrhage into soft tissue (hemosiderophages). Liver cells can sometimes contain bile, which stains very dark, and occasionally long, thin strands of dark material can be seen where canaliculi have become filled with bile.
Cells with Cytoplasmic Vacuoles:
A large, single vacuole is seen in fat cells. In normal or benign cells, the nuclei are small and often indistinct, and the cells are often folded like a collapsed ball. Smaller cells with larger, more prominent nuclei and some cytoplasm in addition to clear, often small vacuoles are more suggestive of malignancy.
Cells with multiple, small vacuoles with a foamy appearance include macrophages, sebaceous glandular cells, and salivary cells. It can be very difficult to differentiate these; the site and other clinical features can be a deciding factor in interpretation.
Differentiation of Round Cell Tumors:
Round cell tumors include mast cells, plasma cells, lymphocytes, histiocytic cells, and transmissible venereal tumor cells. Mast cells have distinctive granules within the cytoplasm and are usually easily identified; if they are the dominant cell type, this is diagnostic for a mast cell tumor. In rare cases, mast cells can have few or no granules in the cytoplasm. Lymphoid cells classically have a very high nucleus:cytoplasm ratio; few other cells have this feature. Neoplastic, lymphoid cells are medium size to large, with a nucleus at least 1.5 times the size of an erythrocyte. Nucleoli are often multiple, sometimes quite prominent. However, the rare cases of small-cell lymphoma have cells indistinguishable from normal lymphocytes.
Cells of a histiocytoma (Langerhans cells) are not especially histiocytic cytologically. They are round cells with a small to moderate amount of pale-staining cytoplasm. They are fairly uniform and have nuclei that are eccentric within the cell. Nucleoli are indistinct. True histiocytic cells are slightly more problematic to interpret. These are part of the cell line that includes the antigen-presenting cells, such as macrophages and Langerhans cells, but can range from inflammatory and reactive cells to highly malignant round cell tumors. They tend to be larger than the other round cells with more cytoplasm, sometimes are vacuolated, and can have oval or indented nuclei. Infiltrates of histiocytic cells are often problematic, even with a full-tissue biopsy examination, and always require histologic examination to assess behavior.
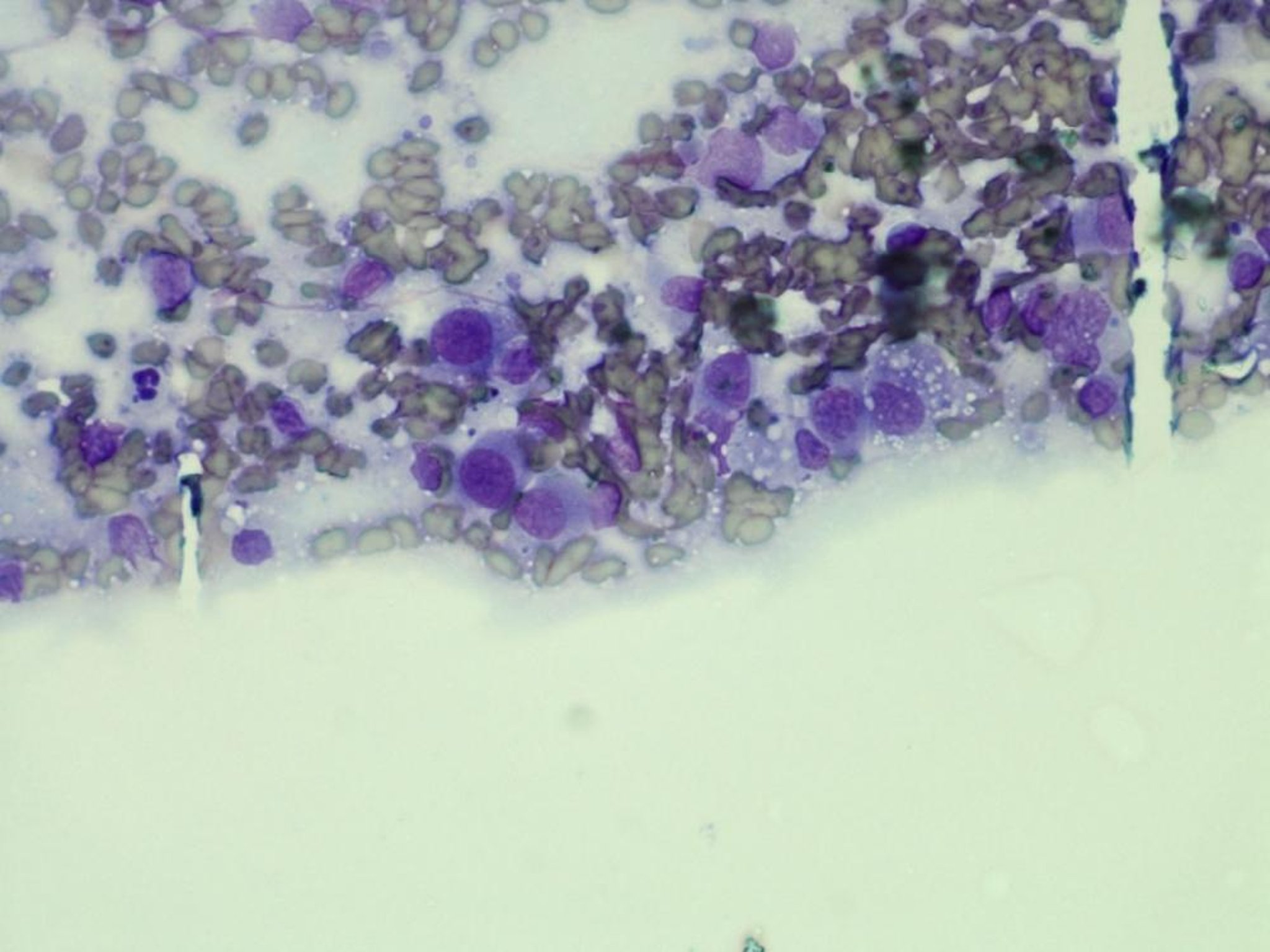
The cells are round with eccentric nuclei and indistinct nucleoli. Occasional cells have small vacuoles in the cytoplasm. As with other round cells, they do not adhere to each other. Note there is blood contamination, and the cells have concentrated at the edge of the smeared blood.
Courtesy of Abbey Veterinary Services.
Neoplastic plasma cells include cells of myeloma. These are usually well differentiated and have most of the characteristics of normal plasma cells. When neoplastic, they are found in large numbers with few other cell types present. Benign nodular proliferations of plasma cells, plasmacytomas, show more marked pleomorphism and often differ markedly from normal plasma cells. Many have a slightly histiocytic appearance, and these can be difficult to distinguish cytologically. These cells have a round nucleus and a coarse chromatin pattern, which sometimes becomes clumped around the nuclear membrane. The nucleus is often eccentric with an intensely basophilic cytoplasm and paranuclear pale Golgi zone.
Cells of transmissible venereal tumors tend to have a moderate amount of cytoplasm (more than found in lymphoblasts), often with small vacuoles. Nuclear chromatin is coarse, with one or two fairly prominent nucleoli. Mitotic figures are often numerous. Unlike most cytology preparations of neoplastic lesions, they tend to have moderate variation in the nucleus:cytoplasm ratio.
Cytology of Specific Sites:
Lymph Nodes:
Normal, hyperplastic, and early neoplastic lymph nodes have a mixed population of cells. Cells are predominantly small lymphocytes with variable numbers of medium and large lymphoid cells and some plasma cells. A uniform population of cells indicates neoplasia. Lymph node aspirates often have a population of cells that are much paler staining and larger, with some cells completely losing their cytoplasm. These cells are in varying stages of degeneration and should be ignored. Size in comparison with RBCs is useful. Normal mature lymphocytes or small neoplastic lymphocytes (rare) have nuclei the same size as RBCs. However, neoplastic lymphoid cells have nuclei at least 1.5 times the diameter of RBCs. Lymphomatous lymph nodes may still contain a significant number of normal lymphoid cells. The proportion of smaller mature lymphocytes must then be compared with the larger immature cells to differentiate hyperplasia from neoplasia. The proportion considered significant varies, but in general, most cytologists consider a diagnosis of lymphoma when immature cells are >50% of the cell population. Some cytologists require a higher percentage of immature cells, particularly if there is only one lymph node enlarged. If there is doubt, a biopsy should be performed. Histopathologic confirmation of diagnosis is essential if therapy for lymphoma is considered and is always needed for full grading.
Submandibular lymph nodes are often difficult to assess. They drain the buccal and nasal areas and are subject to strong antigenic stimuli. They frequently undergo hyperplasia, often histologically atypical, especially in cats. Cats also develop unusual neoplastic conditions affecting this node, such as the T cell–rich B-cell lymphoma and Hodgkin-like lymphoma, both of which have a majority of normal lymph node cells. For these reasons, great care must be taken in the interpretation of lesions involving the submandibular lymph nodes, because false-negative and false-positive results for neoplasia are not uncommon.
Aspirates from suspected enlarged submandibular lymph nodes often yield only large foamy cells, which are salivary cells. This result can be due either to sampling error or to hypertrophy of the salivary gland in cases of sialoadenosis. The cause of sialoadenosis is not understood, but a significant minority of submandibular aspirates contain only these cells.
Body Cavity Fluids:
Meaningful analysis of fluids from body cavities requires total protein (measured with a handheld refractometer), total cell count, and a differential of cell types present ( see Table: Characteristics of Transudates and Exudate). Pure transudates are rare, because they rapidly become modified by leakage of fluid from lymphatics or blood vessels and attraction of mixed inflammatory cells. Transudates attract activated macrophages with varying numbers of nondegenerate neutrophils. The lymphocytes that may also be present are classified as small, but most look slightly larger than circulating lymphocytes and are part of the reactive process of the fluid in the body cavity. In addition, when fluid accumulates in the body cavity, the lining mesothelial cells proliferate and are shed into the fluid. These cells are large, often multinucleated, vary in appearance, and often are seen in groups with large nucleoli. They sometimes form grape-like clusters with a narrow, pale space between the cells. These features are usually considered to be associated with malignancy, but in this case, the cells are simply reactive and not neoplastic. Care must be taken to differentiate these mesothelial cells from neoplastic cells within the body fluid. A small number of these cells typically have a corona around the cytoplasmic envelope (giving a fuzzy outline); this is a distinguishing feature of mesothelial cells.
Characteristics of Transudates and Exudate
Total Protein (g/dL) | Cell Count (cells/mL) | |
|---|---|---|
Transudate | < 2.5 | < 1,500 |
Modified transudate | 2.5–7.5 | 1,000–7,000 |
Exudate | >3.0 | >7,000 |
Mesothelial cells can be present in very large numbers, especially in pericardial fluid. Malignant mesotheliomas are rare in domestic species, but it is not possible to differentiate neoplastic from reactive mesothelial cells on cytologic examination. The degree of polyploidy is not a distinguishing feature.
Mixed inflammatory cells increase in number as a transudate becomes modified and are present in large numbers in an exudate. Mesothelial cells would be expected in this type of sample, and it can therefore be useful to look for a second population when checking for neoplasia. Smoothly demarcated aggregates of atypical cells with no narrow spaces between the cells may indicate a second population of carcinoma cells.
Tracheal or Bronchoalveolar Lavage (BAL):
Respiratory epithelial cells are seen in BAL from healthy and diseased animals. The epithelial cells may retain their original structure with a ciliated surface and basal nuclei, but they often appear round with indistinct cilia.
Macrophages are usually the dominant inflammatory cell type in BAL from healthy animals. These come from deep in the alveoli and are part of the normal defense mechanisms. They greatly increase with fluid accumulation in the lung (eg, cardiovascular insufficiency) and in inflammatory conditions, where they are accompanied by other inflammatory cells. Debris, foreign material, hemosiderin, RBCs, and microorganisms can sometimes be seen in the cytoplasm of these cells. Macrophages containing hemosiderin in people are called heart failure cells, but their cause is less specific in domestic species. There are increased numbers of macrophages in many subacute and chronic lung disorders.
In healthy dogs and cats, neutrophils contribute <5% of cells in BAL preparations. Neutrophils are nonspecific inflammatory cells in the respiratory system and do not necessarily indicate infection. They can be the most numerous cells in an inflammatory reaction, even in cases of allergy. However, when neutrophils are present, the cytoplasm should always be examined carefully for the presence of any infectious agent. Bacteria can also sometimes be seen in the extracellular parts of the smear, but extracellular bacteria are often contaminants from the pharynx.
Great care must be taken to differentiate eosinophils from neutrophils in BAL preparations because the granules are often faint and difficult to identify. Eosinophils can comprise up to 5% of cells in BAL from healthy dogs but may reach 10% in healthy cats. Eosinophils that comprise >10% of cells indicate an allergic respiratory disease, although lungworms and heartworms can also cause this reaction. With lungworm infestation, larvae are sometimes present as large coiled structures.
Nucleated and nonnucleated squamous cells are commonly seen in BAL preparations and are often associated with bacteria on the cell surface. This indicates contamination from the pharynx. Bacteria are normal inhabitants of the pharynx, in particular Simonsiella, which are very large, ladder-like organisms. Their presence confirms contamination from the pharynx. If bacteria are present along with squamous epithelial cells, it may not be possible to conclude whether the bacteria are from the respiratory tree or the pharynx. Bacteria in the cytoplasm of neutrophils confirms a significant infection.
Synovial Fluid:
Full examination of synovial fluid should include protein content, mucin clot formation, viscosity, cell count and differential, and direct cytologic examination. It is usually not feasible to perform all of these tests in a practice setting, but cytologic examination and physical examination can usually give a good estimate of the results of most of these tests. Cytology, therefore, is the most useful single test in synovial fluid examination.
Sampling technique requires the following equipment: a 3-mL syringe, a 21- or 25-gauge needle, clean glass slides, and various collection tubes (plain, EDTA, and heparin). This technique always requires a degree of sedation, and a sterile technique is essential. Each joint has a recommended site for aspiration (beyond the scope of this discussion) and generally requires slight flexion or hyperextension. The needle attached to the syringe is slowly advanced into the joint space and, taking care not to scratch the articular surface, gentle suction is applied. Normal joint fluid is viscous and sticky and of small volume. The volume of fluid, however, depends on the size of the animal, the joint sampled, and the degree of effusion into the joint. When sample size is sufficient, it is essential to release the suction on the syringe before withdrawing the needle.
Sample handling is critical; because many tests can be performed on synovial fluid, and cytology is the most important, sometimes the sample volume is so small that no other test is possible. Therefore, a plain smear should always be made and quickly air dried as soon as the sample is obtained. Most tests can be performed on samples without anticoagulant (a plain red-topped tube), or the sample can be left in the sampling syringe. However, blood contamination, hemarthrosis, and inflammatory effusion introduce fibrin into the joint, and the sample may clot. Placing part of the sample into an EDTA tube can prevent this, but EDTA can interfere in the mucin clot test and, for this reason, a heparinized sample may also be necessary.
Results of cytology preparations can indicate the number of cells present, the type of cell and the differential, the presence of tumor cells, and the presence of bacteria. They can also give an indication of viscosity. In fluid of normal or increased viscosity, cells tend to align in rows in the direction of the smearing; this is described as windrowing.
In healthy animals, cell counts vary widely (eg, 0–4,400/mL in dogs), but they are usually very low. Counts >500/mL in dogs generally indicate a significant increase. Normal synovial fluid contains ~2 cells/high-powered field (400X magnification). In the vast majority of cases where there is an increased cell content, cell numbers are either low (up to 4 or 5 cells/high-powered field) in degenerative joint disease or very high in septic or autoimmune arthritis. Intermediate equivocal results are extremely uncommon.
Cell types include joint mononuclear cells, which are a mixture of circulating monocytes, tissue macrophages, and synovial lining cells. It is not possible, or even necessary, to differentiate these cells, because they all have a similar morphology and all react to similar stimuli. Cytoplasmic vacuolation of these cells, and especially the presence of phagocytosis of debris or RBCs, indicate activation, a feature not seen in normal joint mononuclear cells. In degenerative joint disease, synovial fluid usually contains only macrophages, occasionally with extremely low numbers of neutrophils.
Hemorrhage is common in synovial preparations but is frequently an artifact. True hemarthrosis provides a synovial fluid sample that is uniformly contaminated with blood at the time of sampling. If the blood contamination occurs at the very end of the sampling procedure with clear fluid initially, this is most likely artifact. In addition, in true hemarthrosis, RBCs may be seen in the cytoplasm of macrophages. Artifactual blood contamination will also introduce WBCs, such as neutrophils, making interpretation of inflammatory cells in the sample difficult, although blood contamination still gives only a low cell number.
Neutrophils are present in large numbers in both septic arthritis and autoimmune joint disease. These two conditions can usually be differentiated by the clinical history. In septic arthritis, bacteria are sometimes found within the cytoplasm of phagocytic cells. The absence of bacteria, either within cytology preparations or by culture, does not exclude bacteria as a cause of arthritis. False-negative results for bacteria are not uncommon.
Lymphocytes are often present in very small numbers in inflammatory processes but are not specific for a particular cause.
Osteoclasts are very occasionally seen when there has been erosion of the articular cartilage with exposure of the underlying bone.
Neoplastic cells in joint fluid are rare, although joints can be the site of both primary and secondary tumors.
Macrophages increase with any damage to a joint, especially in cases of degenerative joint disease. Cytoplasmic vacuolation of these cells, and especially the presence of phagocytosis of debris or RBCs, indicate macrophage activation, a feature not seen in normal joint mononuclear cells. In degenerative joint disease, synovial fluid often contains only macrophages.
Nasal Cavity:
The cytology of nasal flush preparations is similar to that seen with BAL preparations. A small number of respiratory epithelial cells are usually flushed out along with exudate. A predominance of eosinophils may indicate inhaled allergens, parasites, or fungi and may occasionally indicate bacteria or neoplasia. The presence of eosinophils in the nasal cavity therefore is less indicative of a specific process than in some other sites, eg, the trachea or bronchi.
Neutrophils are the most common exudative cell but, as with BAL, often indicate secondary infection. In the case of intranasal neoplasia, cells with neoplastic characteristics ( see Neoplasia:) may be present, but absence of these cells does not exclude neoplasia. Only a minority of neoplastic processes erode the overlying respiratory epithelium and allow exfoliation of neoplastic cells.
Similarly, absence of fungal hyphae within the preparation does not exclude fungal infection. Unless fungal plaques are sampled directly for both cytology and culture, false-negative results are common. Viral inclusions are rarely seen.
Vaginal Cytology:
This can be used to identify the various stages of the canine estrous cycle, but results must be interpreted in conjunction with the animal’s behavior. A sample of exfoliated cells is obtained from the vaginal vault cranial to the urethral orifice with a cotton-tipped swab or glass rod. Cells are gently rolled onto a glass slide, air dried, and stained. Features to be identified include neutrophils, bacteria, RBCs, and the types of epithelial cells. Epithelial cells (in increasing order of differentiation) are parabasal, small and large intermediate cells, and superficial cells. Parabasal cells are small, with central round nuclei, indistinct nucleoli, a relatively narrow band of cytoplasm, and a nucleus:cytoplasm ratio of ~1:1. Small intermediate cells have a similar nucleus but a much larger amount of cytoplasm. Large intermediate cells have a similar nucleus with very large amounts of cytoplasm and an angular, irregular outline. Superficial cells also have large amounts of cytoplasm, but their nuclei are pyknotic (small and contracted) or absent.
The stages of the estrous cycle change gradually. If a preparation does not conform exactly to a specific part of the cycle, judgment must be made regarding what stages are present. In proestrus, all types of epithelial cells are present along with neutrophils, RBCs, and mucus. As proestrus progresses, the epithelial cells increasingly approach terminal differentiation (superficial cells), and neutrophils slowly decrease. Bacteria are often present in large numbers. In estrus, >90% of epithelial cells are superficial cells, with no background mucus. There are large numbers of bacteria, but no neutrophils. In diestrus, parabasal and intermediate cells are >80% of the total epithelial cells. Variable numbers of neutrophils and bacteria are present but usually fewer than in proestrus. It can be difficult to differentiate some stages of proestrus from diestrus. In anestrus, parabasal and intermediate cells predominate. Neutrophils and bacteria are rare. RBCs do not help differentiate the stages of estrus.
Cerebrospinal Fluid:
Interpretation of CSF cytology is difficult, because it can be hard to obtain enough well-preserved cells for examination before the sample deteriorates. Cell counts in normal CSF are low (0–5 cells/μL in dogs and 0–8 cells/μL in cats). However, there is a large variation in cell counts between individuals; counts can also vary between cysternal and lumbar taps in the same individual. Because the albumin level of CSF is ~20% of that found in serum, the cells that are present rapidly degenerate. Cell counts should ideally be done and morphology examined within 1 hr of collection.
Because of the low cell numbers, the use of an automated cell counter is usually not appropriate. A hemocytometer can be used for cell counts, and a cytocentrifuge for cytology preparations. A simplified sedimentation technique (description of which is beyond the scope of this discussion) to concentrate cells onto a slide is suitable for practice use. The presence of more than one or two nucleated cells in a plain smear of CSF should be considered potentially significant.
In CSF, an increase in nucleated cells is called pleocytosis. There is tremendous variation and overlap in both the degree of pleocytosis and the types of cells present in both infectious and noninfectious conditions in the CNS. Interpretation should be integrated with the other clinical details of the case. If neutrophils and/or macrophages are present, the cytoplasm of the cells should be searched for bacteria and fungi. The absence of organisms or pleocytosis does not exclude infection, and noninfectious conditions in the CNS can also produce a neutrophilic pleocytosis.
Apart from lymphoma, it is rare to find neoplastic cells in CSF. If noninflammatory cells are present in the CSF, they should be interpreted using the basic principles detailed above.
Urine Cytology:
Urine can be examined as a wet preparation or as a dried cytology smear. Because of the absence of staining in a wet preparation, these are better limited to examination for crystals and RBCs. Although nucleated cells may be seen, in most cases they cannot be identified and are better examined using a dried cytology smear.
There are at least 10 common forms of urinary crystals. Identification is not discussed here but may be readily accomplished by use of good reference illustrations. (Also see Urolithiasis in Small Animals.)
Because cells in urine rapidly degenerate, particularly if bacteria are present, centrifuged preparations of urine samples should be examined rapidly after sampling. If this is not possible, boric acid is often added to urine to prevent degeneration and bacterial overgrowth, although its effect may be very limited. If a delay between sampling and examination is likely, a better preservation method is the addition of a few drops of formalin; however,the traditional Romanowsky stains cannot then be used. H&E stain is a better alternative for formalin-fixed samples.
Normal urine usually has very few nucleated cells. Single urothelial cells are occasionally present. Squamous epithelial cells are also seen in urine and come from the terminal urethra, vagina, vulva, and preputial epithelium. Squamous metaplasia of bladder epithelium after chronic inflammation is very rare.
Neoplastic cells in urine samples are almost always epithelial. They are rounded polygonal cells, often clumped, with marked variation in morphology, especially the nucleus:cytoplasm ratio. Uniform cells are more likely to be normal. Mildly pleomorphic cells can be associated with hyperplasia (eg, some cases of polypoid cystitis).
The inflammatory cells seen in cystitis are almost exclusively neutrophils. Eosinophils are seen in some rare, specific inflammatory conditions, but macrophages are very uncommon even in chronic conditions. By far the most common cause of inflammation is infection, so the cytoplasm of the neutrophils should be examined carefully for bacteria. It is very uncommon to see a significant neutrophil component accompanying neoplasia or calculi.
RBCs are commonly seen with neoplastic and inflammatory diseases of the bladder but are also often seen without an indication of other pathology. This can be a sampling artifact but is also a common finding in cases of interstitial cystitis. In cats, this term is often used synonymously with feline urologic syndrome, but interstitial cystitis also is seen in dogs and people, suggesting other unknown pathogenic factors that can cause this condition. Persistent hematuria without cytologic evidence of neoplasia or inflammation may indicate interstitial cystitis.
Also see Urinalysis.
Liver Cytology:
Although cytology is a popular method to investigate liver disease, there is disagreement on its usefulness. Blood contamination is found in most samples and may overshadow inflammatory infiltrates by introducing circulating WBCs. Diagnosis of many hepatic diseases relies on architectural features and the distribution of the changes within the liver rather than on the morphology of individual cells. Finally, in some hepatic disorders, hepatocytes proliferate without significant changes in their individual morphology (see below). These factors limit the amount of information that can be obtained from cytology of liver tissue.
Sampling methods are similar to those used for other organs. Sampling is usually performed under guidance of ultrasound, but blind sampling can be performed at the tenth intercostal space at the level of the connection of rib to rib cartilage. Bleeding during this procedure is not a significant risk.
In the healthy liver, hepatocytes are plump, polygonal rounded cells with a diameter of 25–30 microns. Nuclei are central and round with a single large, prominent nucleolus. A few cells are binucleated. There is a large amount of blue-staining cytoplasm that usually appears granular.
Changes in the metabolism of liver cells can be seen within the cytoplasm. The presence of numerous small, discrete vacuoles or one large vacuole indicates accumulation of fat. This has several potential causes and is prominent in feline hepatic lipidosis syndrome, starvation, pregnancy, and diabetes mellitus. Enlarged hepatocytes with a pale granular-staining cytoplasm but no discrete vacuoles are characteristic of excess glycogen storage. This is most often caused by increased levels of circulating steroids.
Bile stasis and pigment accumulation (eg, iron) can also be assessed by examination of the cytoplasm. Hepatocytes normally accumulate lipofuscin pigment, noted as small, fairly uniform, dark-staining granules, whereas bile and often hemosiderin tend to appear as slightly larger dark-staining bodies within the cytoplasm. Bile accumulation within the canaliculae (canalicular plugs) can also occasionally be seen. These appear as black ribbons on the surface of hepatocytes.
Cytologic interpretation of inflammation is difficult because of the inevitable blood contamination of samples. Inflammation should be considered significant only if it is present within clusters of hepatocytes. Although the individual inflammatory cells can be recognized, it is not possible to indicate which part of the liver is principally affected. Neutrophils can be seen in diffuse hepatitis and also in more focal cholangitis. Small, mature inflammatory lymphocytes are usually seen in periportal inflammatory conditions, such as lymphocytic pericholangitis in cats and chronic active hepatitis in dogs. Macrophages can also be seen in the chronic inflammatory conditions and also in certain infections. Phagocytic cells should be investigated for the presence of organisms within the cytoplasm, but this is uncommon in liver disease.
Primary proliferative nodular hepatocellular lesions include regenerative hyperplasia, nodular hyperplasia, adenoma (hepatoma), and hepatocellular carcinoma. Biliary proliferations can appear as cysts, adenomas, or carcinomas. Bile duct cells tend to be smaller than hepatocytes with less cytoplasm. They are cuboidal or low columnar cells that occasionally produce tubular structures within cytology samples. The cytoplasm is also more uniformly pale staining and not significantly granular. Nucleoli are smaller and less distinct. Significant cell harvest from cystic bile ducts is uncommon because most of these lesions are simply cystic space rather than cellular. If a significant number of biliary epithelial cells are obtained, neoplasia is most likely. However, malignant bile duct cells are more commonly uniform in size and shape and, therefore, do not always show the morphologic features usually associated with malignancy.
Hepatocellular proliferation is a difficult area of interpretation, because hepatocytes in benign proliferative lesions are very similar to those in well-differentiated carcinomas and indeed often cannot be differentiated even from normal hepatocytes. Only in cases with poorly differentiated pleomorphic cells can an adequate interpretation of malignancy be made. The benign and non-neoplastic proliferations always have the same morphology as normal hepatocytes. Therefore, false-negative results for proliferative lesions within the liver are common. Cytology is thus of limited value for nodular hepatocellular lesions.
Cytology can be a useful technique for diagnosis of round cell tumors in the liver. Even with severe inflammatory lesions, lymphocytes are present in low numbers and are generally small, mature lymphocytes. A large population of medium and large lymphoid cells indicates lymphoma. No other condition will give this result.
The other common round cell tumor that can affect the liver (particularly in cats but also occasionally in dogs) is mast cell tumor. The granules within mast cells are metachromatic, facilitating diagnosis. Aspirates of normal liver may contain a few mast cells, but in neoplasia they are usually present in large numbers. If other cells are obtained from cytology preparations, they should be interpreted using the principles described above.
Kidney Cytology:
Normal renal aspirates have almost a pure population of renal tubular cells. These are uniform, medium-sized cells of ~17–20 microns with central nuclei, small indistinct nucleoli, and a moderate amount of pale-staining cytoplasm. In cats, lipid droplets within the cytoplasm are a common, normal feature. The cells can be present either singly or in clusters and can occasionally be seen as tubular structures. They sometimes contain small, dark granules within the cytoplasm.
Renal lymphoma is the most common neoplastic disease of the kidney in cats and dogs. Because the cells are usually widely distributed within the tissue, false-negative results with cytologic examination are uncommon. Diagnosis can be made using the criteria described above. Primary renal tumors are uncommon.
Cystic lesions include renal cysts, most commonly seen in cats but also occasionally in dogs, and hydronephrosis. In both disorders, cell harvest is usually low, with a large amount of fluid. The cellular component of the sample is rarely helpful in identifying further the nature of the cystic structure.
Most inflammatory lesions in the kidney are chronic and produce fibrous connective tissue. Cell harvest from these lesions is usually exceedingly low, and cytology is not typically a useful technique. Pyogenic inflammation can sometimes be diagnosed. Cytology may help diagnose feline infectious peritonitis, although diagnosis using serologic techniques is more common. Because of the usually severe and widespread nature of the inflammation, cell harvest is usually high. The wide mixture of inflammatory cells present in feline infectious peritonitis, with a predominance of neutrophils, along with an appropriate history, are typical of the disorder.
Mammary Cytology:
Cytology is useful to differentiate inflammatory from neoplastic nodular lesions within mammary tissue. Mammary tumors are not commonly inflamed. It is less useful to differentiate the neoplastic conditions.
Neoplastic lesions must be interpreted using the criteria listed above ( see Neoplasia:). The criteria most useful to determine the behavior and prognosis of a mammary tumor are local tissue and vessel invasion, not cell morphology. These are best assessed histologically rather than cytologically. Therefore, cellular morphology is not necessarily a good guide to tumor behavior. In cats, malignant cells are often uniform and do not exhibit the normal malignant features; the size of the malignant tumor is the most useful prognostic indicator.





