

Periodontal disease is infection and inflammation of the periodontium. Key clinical signs are halitosis, plaque and calculus, inflamed and bleeding gums, gingival recession, periodontal pocketing, bone loss, furcation exposure, mobile teeth, and eventual loss of teeth. Diagnosis is by means of periodontal probing and dental radiography to assess the amount of attachment loss associated with the teeth. Treatment includes professional dental cleaning and cleaning of the root surface or periodontal pocket with gingival curettage (with or without creating a periodontal flap).
Periodontal disease is infection and inflammation of the tissues that surround and support the teeth (ie, periodontium):
alveolar bone
cementum
periodontal ligament
gingiva
Clinical or radiographic evidence of inflammation, breakdown, or loss of any of the periodontium constitutes some level of periodontal disease.
If left untreated, gingivitis (inflammation of the gingiva) can progress to periodontitis (inflammation of the deeper periodontal tissues).
Periodontal disease is not without systemic effects (impact on organ health, interaction with endocrine diseases, etc).For example, periodontal disease has been associated with an increased risk of chronic azotemic kidney disease (2, 3, 4).
A variety of terms are used to describe the procedures involved in oral examination and the treatment and prevention of periodontal disease. Colloquial terminology includes “prophy,” “prophylaxis,” and “dental”; however, these terms are fraught. More descriptive terms such as comprehensive oral health assessment and treatment (COHAT); comprehensive oral prevention, assessment, and treatment (COPAT); and oral assessment, treatment, and prevention (oral ATP) have been proposed.
Etiology and Pathogenesis of Periodontal Disease in Small Animals
Periodontal disease is caused by plaque bacteria accumulating on the tooth surface and eliciting a host response to the bacterial insult. The accumulation of plaque, the biodiversity of microbiota, and the host immune system are factors in the pathogenesis of periodontal disease.
The oral cavity supports a rich bacterial microbiota of both aerobic and anaerobic species, many of which thrive in plaque on tooth surfaces in periodontal disease. Bacterial plaque on the crown surface of a tooth constantly presents antigen to the marginal gingiva, stimulating an inflammatory response, resulting in gingivitis.
The bacteria in plaque are predominantly nonmotile, gram-positive aerobes, including Staphylococcus spp and Streptococcus spp; however, many others are also present.
Although this microbiota does stimulate an immune response, the bacteria in an otherwise healthy mouth exist in relative commensal harmony with the host. They may even be beneficial by helping to limit the numbers of periodontopathogenic bacteria.
If the plaque becomes very thick (eg, with poor oral hygiene) and oxygen within the plaque is depleted, the bacterial population can become more pathogenic, with a higher percentage of nonmotile, gram-negative anaerobic rods. Along with many others, the following bacteria are found in the presence of teeth with periodontal disease:
Bacteroides fragilis
Peptostreptococcus
Porphyromonas gulae
Porphyromonas salivosa
Porphyromonas denticanis
Prevotella intermedia
Treponema spp
Bacteroides splanchnicus
Interestingly, some of the common human periodontopathogens such as Haemophilus (formerly Actinobacillus) actinomycetemcomitans are notably absent in animals.
Subgingival plaque (plaque on the tooth surface below the gingival margin) is also commonly inhabited by these more periodontopathogenic species of bacteria. Periodontitis is caused by the host's response to subgingival plaque.
Inflammatory mediators produced by the host directly result in bone and tissue damage around the root. The bacteria themselves and their metabolic products also contribute to bone damage.
Development of periodontitis is also affected by other intrinsic (eg, genetics, tooth crowding, thin alveolar bone, age) and extrinsic (eg, diet, stress, concurrent disease, oral hygiene) factors.
Plaque
Plaque is the soft layer or film on the tooth surface that forms from a combination of food particles, salivary glycoproteins and minerals, and bacteria present within the mouth. It begins as a biofilm on the tooth surface that matures to a more complex layer from the interactions with the bacterial organisms found within the mouth.
Plaque is composed of many microorganisms that differ from their planktonic forms. In a biofilm, microorganisms are more resistant to antimicrobials, disinfectants, and antibacterial agents.
Plaque continuously forms on the tooth surface and in between the teeth. It can be removed from the surface by daily brushing and a professional dental cleaning, although by the next day, an additional layer has begun to form on the tooth surface. Plaque is the precursor to calculus (tartar).
Calculus
Calculus, or tartar, is the mineralized form of plaque. As the plaque remains undisturbed on the tooth surface, the salivary minerals help the plaque mature to form calculus.
This hard substance creates a protective barrier for the bacteria. This shield can cause a mechanical irritation to the soft tissues of the gingiva and the buccal mucosa and also elicit an inflammatory response from the host, resulting in breakdown or loss of the periodontium (structures holding the teeth in the mouth).
Gingivitis
Gingivitis is inflammation (ie, redness, swelling, and bleeding) of the gingiva (ie, the gums), a tough, keratinized cuff of soft tissue associated with the teeth that is tightly adhered to underlying bone via periosteum and continuous with the alveolar mucosa.
In the progression of periodontal disease, gingivitis occurs first. Gingival inflammation then extends apically leading to loss of periodontal attachment.
Epidemiology of Periodontal Disease in Small Animals
Up to 70% of cats and 80% of dogs have some level of periodontal disease by age 2 (1). There is a correlation between increased body weight and age with an increased incidence of periodontitis in cats.
Other risk factors include toy breeds, immunosuppression (diabetes mellitus, hyperadrenocorticism), poor nutritional status, and abnormally positioned plaque retentive surfaces (eg, malocclusion).
Clinical Findings and Lesions of Periodontal Disease in Small Animals
Key clinical signs of periodontal disease are bad breath (halitosis); plaque and calculus (tartar) accumulation; red, swollen, and bleeding gums (ie, gingivitis); gingival recession; periodontal pocketing; bone loss; furcation exposure; mobile teeth; and eventual loss of teeth.
Common indices used in veterinary dentistry qualitatively grade the degree of whole-mouth calculus (see the table ) and gingivitis (see the table ) on ordinal scales of 0–3.
Calculus Grading
Grade | Characteristics |
|---|---|
0 (None) | No supragingival calculus |
1 (Mild) | Minimal supragingival calculus |
2 (Moderate) | Moderate supragingival calculus with subgingival deposition |
3 (Severe) | Heavy supragingival calculus with substantial subgingival deposition |
Gingivitis Grading
Grade | Characteristics |
|---|---|
0 (None) | Normal gingiva |
1 (Mild) | Mild swelling and slight increased red color |
2 (Moderate) | Moderate swelling and redness, with bleeding upon periodontal probing |
3 (Severe) | Severe swelling and redness, with spontaneous bleeding |
A common index used in veterinary dentistry qualitatively grades the degree of localized or generalized periodontal disease on an ordinal scale of 0–4 (see table ):
Stage 0: In teeth with healthy periodontal tissues, no gingivitis or periodontitis is evident, thus there is no evidence of periodontal disease.
Stage 1: There is gingivitis only, without attachment loss; the height and architecture of the alveolar margin are normal. This stage is confined to the soft tissues only. At this stage, there is normal periodontal pocketing.
Stage 2: There is early periodontitis with < 25% of attachment loss or, at most, there is a stage 1 furcation involvement in multirooted teeth. The furcation area of a tooth is where the roots of a multirooted tooth converge and meet. There may be early radiographic signs of periodontitis and attachment loss. The loss of periodontal attachment is < 25% as measured by increased periodontal probing depth or by suspected loss of attachment, determined radiographically by an increased distance from the normal alveolar margin to the cementoenamel junction relative to the length of the root.
Stage 3: There is moderate periodontitis, with 25%–50% of attachment loss as measured by increased periodontal probing depth or by radiographic determination of the distance of the alveolar margin from the cementoenamel junction relative to the length of the root, or there is a stage 2 furcation involvement in multirooted teeth (see ).
Stage 4: There is advanced periodontitis, with > 50% of attachment loss as measured by increased periodontal probing depth or by radiographic determination of the distance of the alveolar margin from the cementoenamel junction relative to the length of the root, or there is a stage 3 furcation involvement in multirooted teeth (see ; see also ).
Stages of Periodontal Disease
Stage | Gingivitis | Attachment Loss |
|---|---|---|
0 | No | No |
1 | Yes | No |
2 | Yes | < 25% |
3 | Yes | 25%–50% |
4 | Yes | > 50% |


Gingivitis, or inflammation of the gingiva, of cheek teeth in the left maxilla of a dog. Note moderate to severe plaque and calculus accumulation and red and swollen gingiva at the third and fourth premolar teeth and first molar tooth. This dog would have a calculus index of 2–3 and gingivitis index of 2.
Courtesy of Dr. Ben Colmery III.

Clinical appearance of periodontitis of canine, premolar, and molar teeth in the left mandible of a cat. Note the presence of gingivitis and gingival recession, most notably of the third and fourth premolar teeth.
Courtesy of Dr. Ben Colmery III.


Calculus grade 3 of the maxillary and mandibular incisor and canine teeth. Note deposition of calculus on the tooth surfaces and the apparent fissure lines associated with the maxillary incisors and the location of the mandibular symphysis. The fissure lines are present because the teeth have clinical mobility. Also note the clinical absence of the mandibular central incisors. All maxillary and mandibular teeth were clinically present beneath the calculus in this patient.
Courtesy of Dr. Brenda Mulherin.
Diagnosis of Periodontal Disease in Small Animals
Conscious oral examination
Anesthetized oral examination
Intraoral dental radiography
A conscious oral examination in small animals is the precursor to an anesthetized oral examination.
Intraoral dental radiography is a valuable diagnostic tool. In certain cases, advanced imaging (eg, CT) may be helpful (eg, for treatment planning).
Conscious Oral Examination
The information gathered on a conscious oral examination should be interpreted with caution because only the external surface of the teeth may be observed. The information gathered is also dependent on the compliance of the patient.
When performing a conscious oral examination, the viewer can gather information on the following:
any occlusion abnormalities
obvious signs of trauma to the teeth (tooth fractures or discoloration, etc)
evidence of calculus (tartar) on the teeth or inflammation
presence of all teeth
extra or missing teeth
evidence of foreign material or abnormal growth of tissue within the mouth
The key to the conscious oral examination is symmetry. There should be symmetry to the calculus deposition or inflammation (if present) and symmetry to the animal's bite or occlusion.
Occlusion
An animal's occlusion should be identical on the right and left sides. It is easiest to assess the occlusion on a conscious examination or on a sedated examination before an endotracheal tube is placed.
There are 5 main characteristics of a normal occlusion:
Midline match: Characteristics of a midline match are those in which the maxillary and mandibular incisors meet at midline on both arcades. A parallel line should be able to be created without shifting the line to either the right or the left side.
Incisor overlap: The incisor overlap is described as the occlusal cusps of the maxillary incisor teeth being positioned just in front of the occlusal cusps of the mandibular incisor teeth so that the mandibular incisors occlude in the cingulum of the maxillary incisor teeth.
Canine interlock: The mandibular canine tooth should be positioned between the maxillary third incisor tooth and the maxillary canine tooth. The mandibular canine tooth should also be slightly angled toward the buccal surface of the cheek.
Premolar interdigitation: The cusp tips of the maxillary premolar teeth should be positioned in the space created by the mandibular premolar teeth.
Carnassial overlap: The carnassial teeth in the dog and the cat are defined as the maxillary fourth premolar and the mandibular first molar teeth. These teeth should overlap in a normal occlusion with the maxillary fourth premolar tooth overlapping the mandibular first molar tooth on the buccal aspect of the tooth.
Any deviation of these 5 points of a normal occlusion will constitute a malocclusion.
Historically, an animal's occlusion may have been described as brachygnathic or prognathic. This can be confusing because it depends on which arcade is the one being described as abnormal. Rather, malocclusions can be divided into 4 classifications:
Class 1: Neutroclusion is described as a normal relationship between the maxillary and mandibular arcades, but there is malposition of one or more teeth.
Class 2: Mandibular distoclusion (parrot mouth) is described as an abnormal relationship between the maxilla and the mandible with the mandible being positioned caudal to the maxilla. This would give the appearance of the mandible being too short, or the maxilla being too long. In this occlusion, the mandibular incisors do not occlude with the cingulum of the maxillary incisors.
Class 3: Mandibular mesioclusion (monkey mouth) is described as an abnormal relationship between the maxilla and the mandible with the mandible being positioned rostral to the maxilla. This would give the appearance of the mandible being too long or the maxilla being too short. In this occlusion, the mandibular incisors occlude in front of the maxillary incisors.
Class 4: Maxillomandibular asymmetry is divided into three categories dependent on the occlusion presented:
In rostrocaudal malalignment, there is a "front to back" discrepancy. One side of the jaw is longer than the other side of the jaw; stated differently, one side has mesioclusion or distoclusion.
In side-to-side malalignment, there is a loss of a midline match, and the maxilla or mandible is deviated to the right or left side away from midline. The maxillary and mandibular incisor teeth do not align with midline.
In dorsoventral malalignment, the maxilla and mandible do not meet to form a closed bite and the patient has an open bite. This is usually caused by the maxilla or mandible being either too wide or too narrow. This creates an abnormal space between the teeth that does not allow the mouth to fully close.
An alternative term to describe any of these three types of class 4 malocclusion is wry bite.
Anesthetized Oral Examination
Anesthetized oral examination allows the veterinarian to evaluate the structures that support the teeth. It also allows evaluation of the other soft tissue structures of the mouth, including the tongue, tonsils, hard and soft palates, and buccal mucosa.
Anesthetized examination gives the veterinarian the best opportunity to evaluate these structures and observe whether there are any abnormalities present within the mouth, such as areas of inflammation, enlargement consistent with neoplasia, or foreign material within the mouth. Early detection of oral masses is paramount for detecting neoplasia. In addition, an extraoral examination including palpation of the face should be performed.
Periodontal assessment includes tooth-by-tooth assessment involving periodontal probing to measure sulcus depth and to assess furcation exposure in multirooted teeth and tooth mobility. Findings and any treatment are recorded in a dental chart (a graphical representation of the mouth, displaying each tooth in occlusal, buccal, and/or palatial/lingual aspects).
Periodontal Probing
All dogs and cats should maintain a physiologic periodontal pocketing depth. This pocket is filled with crevicular fluid.
In a healthy mouth, the amount of fluid produced is very small and is meant to help flush food particles and bacteria away from the free gingival margin. In a diseased pocket, the crevicular fluid is considered an exudate composed of inflammatory mediators and the byproducts of broken-down tissues and cells.
When advanced disease is present, an increased periodontal probing depth will be observed as will an increased loss of attachment of the periodontium (see ).


To assess the probing depth on a patient, a periodontal probe is inserted with gentle pressure between the free gingival margin of the gingiva and the tooth surface to the level where the gingiva is attached to the tooth. The depth of penetration directly corresponds with the periodontal probing depth for that area of a tooth. Because a single area may not be representative, six different areas need to be assessed for circumferential evaluation of a tooth. The normal periodontal probing depth is
Courtesy of Dr. Brenda Mulherin.
The normal accepted probing depth for the dog is 1–3 mm and for the cat is 0.5–1 mm. Although the periodontal probing depth can vary between patients and specific teeth, 1–3 mm is the accepted standard range regardless of the size of the patient.
Periodontal probing is accomplished by placing the periodontal probe between the tooth and the free gingival margin and sinking the probe into the sulcus with gentle pressure. The periodontal probing depth is calculated as the measurement where the probe stops within the base of the sulcus (ie, the level where the gingiva is attached to the tooth).
Furcation Exposure
For multirooted teeth, the periodontal probe is inserted from the side where the roots branch to assess for furcation exposure.
Stage 1 furcation involvement exists when a periodontal probe extends less than halfway under the crown in any direction of a multirooted tooth with associated attachment loss.
Stage 2 furcation involvement exists when a periodontal probe extends approximately halfway under the crown of a multirooted tooth with associated attachment loss but does not extend all the way through the roots of a tooth.
Stage 3 furcation exposure exists when a periodontal probe extends under the crown of a multirooted tooth, through and through from one side of the furcation and out the other.
Mobility
All teeth should have some level of mobility. If they were held rigidly in the alveolar bone, they would be more prone to trauma and fracture. The periodontal ligament allows physiologic movement of the teeth.
Stage 0 mobility up to 0.2 mm is considered physiologic.
Stage 1 mobility is present when tooth mobility is increased in any direction other than axial over a distance of > 0.2 mm and up to 0.5 mm.
Stage 2 mobility is present when tooth mobility is increased in any direction other than axial over a distance of > 0.5 mm and up to 1 mm.
Stage 3 mobility is present when tooth mobility is increased in any direction other than axial over a distance > 1 mm or any axial movement. An axial movement would be one in which the tooth can be depressed into the alveolus in an axial direction.
Intraoral Dental Radiography
The 2019 AAHA Dental Care Guidelines for Dogs and Cats strongly recommends full-mouth intraoral dental radiography in all dental patients. Intraoral radiographs are necessary to fully assess the extent of disease and thus avoid inappropriate treatment or overlooking inapparent disease (see ).


Intraoral radiographic appearance of periodontitis of cheek teeth in the left mandible of a cat. Note the loss of alveolar bone, most notable at the distal root of the third premolar tooth and mesial root and furcation of the fourth premolar tooth.
Courtesy of Dr. Ben Colmery III.
Treatment of Periodontal Disease in Small Animals
Professional dental cleaning
Periodontal treatment
Dental extraction
Treatment of periodontal disease depends on the severity of attachment loss. Frequent treatments that are used to stabilize or treat the progression of disease include the following:
professional anesthetized dental cleaning (scaling and polishing)
closed periodontal treatment (root planing and gingival curettage)
local administration of antiseptic and anti-inflammatory drugs
open periodontal treatment (improved access to diseased tissues after flap creation)
complex flaps and bone grafting procedures to extraction of nonsalvageable teeth
home oral hygiene (measures taken by the client at home)
Professional Dental Cleaning
When treating gingivitis, removal of the bacterial plaque on the tooth surfaces is of utmost importance. This can reverse gingivitis, returning the gingiva to a healthy, uninflamed state. This is achieved through professional dental cleaning (scaling and polishing) with power and manual instruments under general anesthesia to remove plaque and calculus.
Dental cleaning on an awake animal improves the cosmetic appearance of the tooth crowns but does not improve periodontal health. The owner might falsely believe the condition has been treated; however, periodontal disease continues to thrive below the free gingival margin, causing attachment loss.
If the gingivitis does not resolve, further examination should be performed to identify additional complicating conditions, such as persistent subgingival plaque and calculus or the presence of predisposing factors.
Some less common causes of gingivitis, such as systemic disease (eg, uremic stomatitis), autoimmune disease, juvenile hyperplastic gingivitis, or gingivostomatitis, may require more than plaque removal alone to decrease the inflammation.
Periodontal Treatment
Periodontitis requires more aggressive periodontal treatment.
Closed root planing and curettage is debridement without creating a mucoperiosteal flap. Open root planing is the act of cleaning and debriding the root surface or periodontal pocket after creating a mucogingival flap.
Various periodontal surgeries with or without bone graft or membrane placement can also be used to help decrease attachment loss noted on anesthetized oral examination.
Root scaling (removing plaque and calculus on exposed root surfaces) and root planing (smoothing the root surfaces by removing textural irregularities and diseased cementum) are performed, followed by gingival curettage that removes the infected and inflamed inside layer of a periodontal pocket.
Shallow periodontal pockets are treated in a closed fashion (without a flap); however, pockets > 5–6 mm deep require open surgery (creation of a periodontal flap) to expose the root surface and alveolar bone for adequate treatment (root scaling and planing and alveoloplasty). The connective tissue side of the flap needs to be debrided before closure of the flap to avoid contact of infected and inflamed granulation tissue with the planed root surfaces.
Local placement of a perioceutic agent containing antimicrobials (eg, doxycycline) into cleaned periodontal pockets may be helpful. Extraction is often the best treatment for teeth with increased mobility and attachment loss that have a guarded to poor prognosis.
Periodontitis is not as easily reversible as gingivitis. Lost alveolar bone may be augmented by use of bone grafts or bone graft substitutes. Barrier membranes may be placed between the bone defect and gingival tissues to achieve guided tissue regeneration.
Maxillary canine teeth with pockets on the palatal aspect of the tooth that have already progressed to form an oronasal fistula require extraction and oronasal fistula repair. Deep infrabony defects in multirooted teeth with bone loss that undermines a furcation can infect the pulp through a furcation canal, resulting in secondary endodontic disease.
Similarly, if periodontitis has progressed apically and reached the apex of the root of a tooth, secondary endodontic disease will develop. Saving such teeth requires both periodontal treatment and endodontic treatment, and the prognosis is determined by the extent of periodontal disease.
Dental Extraction
Teeth that have become mobile because of loss of attachment should be extracted. Occasionally teeth can be saved through major periodontal surgery procedures. It is important to note that disease will recur without drastic changes in home oral hygiene.
Extraction of diseased teeth allows the soft tissue and affected bone to heal. While this procedure is a definitive treatment for a diseased tooth, a pet dog or cat can function without teeth and have an excellent and potentially improved quality of life.
Prevention of Periodontal Disease in Small Animals
Prevention of gingivitis is the same as its treatment: plaque removal and control. Biofilms are easily and effectively removed mechanically with a toothbrush. Even large accumulations of supragingival plaque are easily removed by toothbrushing. Teeth should be brushed daily to remove plaque and prevent calculus (tartar) accumulation (see ). While plaque can be removed by brushing, calculus can only be removed with professional scaling and polishing.

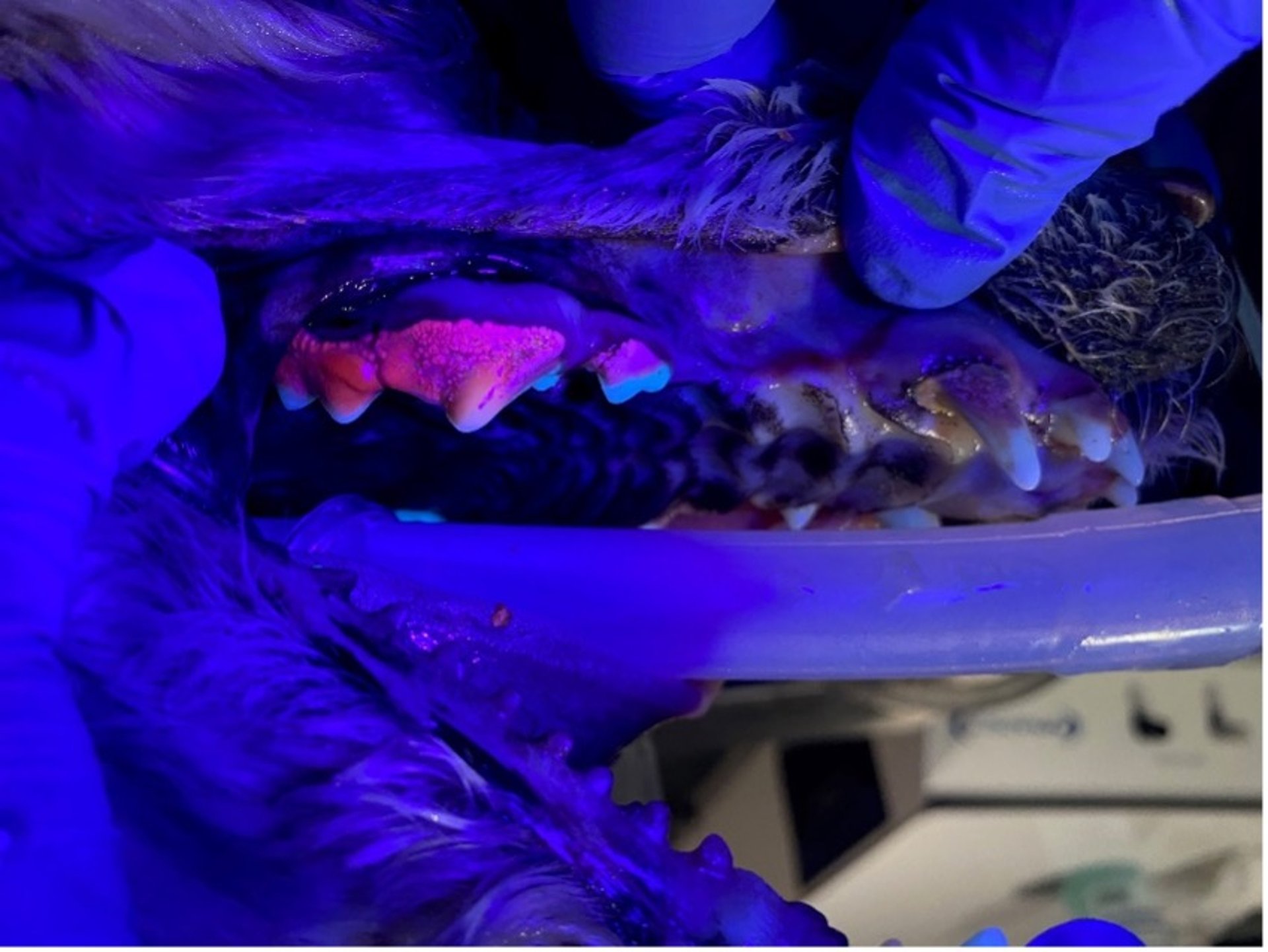
Use of a plaque light on the maxillary premolar teeth of a dog. Plaque fluoresces a bright pink color when the blue light is applied. This can be a training tool for owners to recognize the amount of plaque on the tooth surface. In addition, for owners who are diligent with home care, it can identify areas in which they could improve their brushing technique. Note that the image demonstrates the use of a plaque light to identify plaque, but it is overlying a heavy layer of calculus, which can only be removed by a professional.
Courtesy of Dr. Brenda Mulherin.
Only the outside (labial and buccal) surfaces of the teeth need to be brushed in most dogs and cats. The lingual or palatal surfaces of the teeth are more difficult to access. Fortunately, the tongue rubs against these surfaces, allowing less plaque and calculus formation on these surfaces in most patients.
For dogs and cats that may not tolerate regular toothbrushing, plaque accumulation can be decreased by wiping the tooth surfaces with a gauze pad at least every second day. Plaque that remains on the tooth surface for > 2 days mineralizes to form calculus that cannot be removed by brushing.
Although calculus gives the appearance of unhealthy teeth, its contribution to periodontal disease is minor. Calculus needs to be removed with a professional dental cleaning and cannot be removed with daily brushing.
Texture of the diet, chews, treats, and toys can affect the self-cleansing mechanisms of the teeth. Firm, fibrous items that allow tooth penetration can remove plaque (and occasionally calculus) from the tooth surfaces during chewing. Items that are hard (eg, bones, hooves) can crack teeth and should be avoided.
The common perception that dry kibble (as opposed to canned food) decreases plaque and calculus through mechanical cleaning does not necessarily always hold true. The Veterinary Oral Health Council website provides further information about dental home care products that meet certain requirements for plaque and calculus control.
In addition to texture, some diets are formulated to include ingredients that help decrease oral bacteria (eg, chlorhexidine) or slow plaque mineralization (eg, polyphosphates).
Products that slow the development of the pellicle (biofilm) on the tooth surface or prevent the adhesion of pioneering plaque bacteria on the surface of the tooth may provide some benefit.
Prevention of periodontitis is more complicated. Regular daily home care and oral hygiene measures to prevent and remove supragingival plaque provide some protection. This routine helps by minimizing the number of periodontopathogens in the mouth.
More importantly, predisposing anatomical and systemic factors, including the following, should be identified and addressed:
Severe crowding of teeth or supernumerary teeth causing crowding can be relieved through selective surgical extractions.
Metabolic conditions such as diabetes mellitus or renal failure can be diagnosed, treated, and controlled.
Inappropriate behaviors or parafunctional habits such as cage biting or rock chewing and inappropriate selection of toys (eg, tennis balls) that damage the tissues can be identified and modified.
Key Points
Plaque is a soft biofilm that, combined with the host immune response, produces inflammation of the periodontium, resulting in periodontal disease.
Periodontal disease is diagnosed and treated under general anesthesia by trained veterinary professionals using periodontal probing and dental radiography to assess attachment loss.
Providing daily or at least every other day toothbrushing appears to be the most effective way to improve and maintain periodontal health. In addition, dental diets; chews, treats, and toys; oral gels, rinses, and sprays; and water and food additives can be used to help stabilize and decrease the incidence of periodontal disease.
References
Wiggs RB, Lobprise HB. Periodontology, In: Veterinary Dentistry, Principles and Practice. Lippincott Raven; 1997:186-231.
Cave NJ, Bridges JP, Thomas DG. Systemic effects of periodontal disease in cats. Vet Q. 2012;32(3-4):131-144. doi:10.1080/01652176.2012.745957
Dersot J-M. How to recognize the eight signs of periodontitis?Int Orthod. 2013;11(2):166-176. doi:10.1016/j.ortho.2013.02.003
Trevejo RT, Lefebvre SL, Yang M, Rhoads C, Goldstein G, Lund EM. Survival analysis to evaluate associations between periodontal disease and the risk of development of chronic azotemic kidney disease in cats evaluated at primary care veterinary hospitals. J Am Vet Med Assoc. 2018;252(6):710-720. doi:10.2460/javma.252.6.710
For More Information
Mulherin BL, ed. Veterinary Oral Diagnostic Imaging. Wiley-Blackwell; 2023.
Also see pet health content regarding dental disorders of dogs and dental disorders of cats.





