




Esophageal obstruction, commonly known as choke, occurs secondary to obstruction of the esophagus with food or foreign objects. Symptoms include nasal discharge of feed, coughing, bloat, and dysphagia. The diagnosis is confirmed with passage of an oro- or nasogastric tube or with endoscopy of the esophagus. Most cases can be resolved by means of sedated lavage of the esophagus, with water delivered by oro- or nasogastric tube to remove the impacted feed material. Rare cases require general anesthesia or surgery to resolve the obstruction. The prognosis for uncomplicated cases is good; however, complications such as esophageal stricture or aspiration pneumonia can worsen the prognosis.
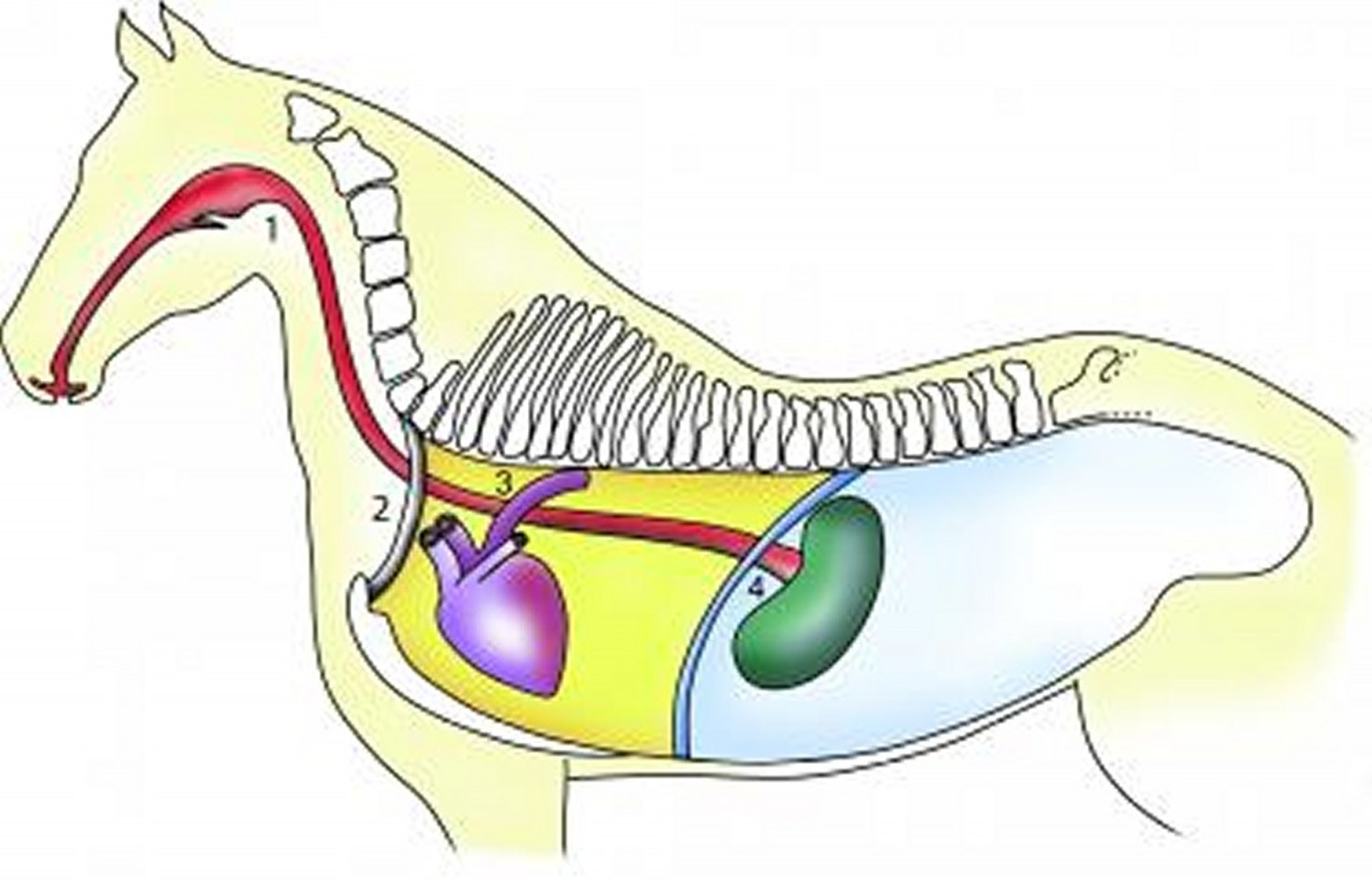
Esophageal obstruction (choke) occurs when the esophagus is blocked by food or foreign objects. It is the most common esophageal disease in large animals. Horses most commonly obstruct on grain, beet pulp, or hay. Esophageal obstruction can also occur after recovery from standing chemical restraint or general anesthesia. Cattle tend to obstruct on a single, solid object (eg, apples, beets, potatoes, turnips, cornstalks, or ears of corn).
Clinical Findings of Esophageal Obstruction in Large Animals


Courtesy of Dr. Jan Hawkins, Purdue University.
In horses, clinical signs associated with esophageal obstruction include nasal discharge of feed material or saliva, dysphagia, coughing, or ptyalism. The horse may appear anxious or appear to retch by stretching and arching the neck. Affected horses may continue to eat or drink, worsening the clinical signs.
In cattle, clinical signs include free-gas bloat, ptyalism, or nasal discharge of food and water. Ruminants may be bloated and in distress or recumbent, or there may be protrusion of the tongue, extension of the head, bruxism, and ptyalism. Acute and complete esophageal obstruction is an emergency because it prohibits eructation of ruminal gases, and free-gas bloat develops. Severe free-gas bloat may result in asphyxia because the expanding rumen puts pressure on the diaphragm and reduces venous return of blood to the heart.
Diagnosis of Esophageal Obstruction in Large Animals
Clinical signs
Outcome of passage of an oro- or nasogastric tube
Endoscopy
Esophageal obstruction can usually be diagnosed based on clinical signs. Physical examination findings compatible with esophageal obstruction include nasal discharge of feed material and water, bruxism, ptyalism, and palpable enlargement of the esophagus. In some instances, foreign objects lodged in the cervical esophagus may be located via palpation. Subcutaneous emphysema, cervical cellulitis, and fever may be associated with esophageal rupture. The inability to pass a stomach (ruminants) or nasogastric tube (horses) can also confirm the diagnosis.


Courtesy of Dr. Sameeh M. Abutarbush.

Courtesy of Dr. Sameeh M. Abutarbush.
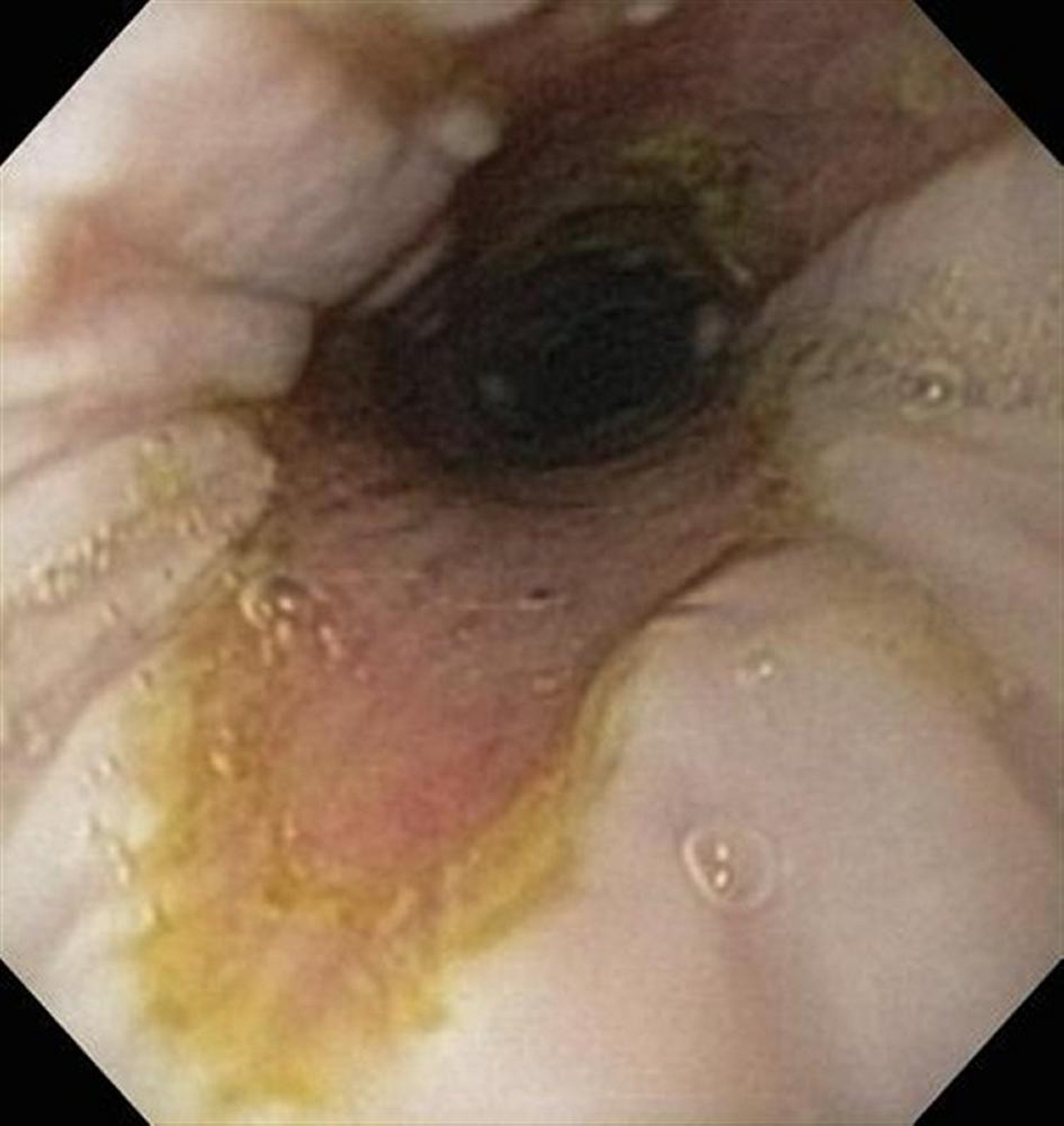
An endoscopic examination helps localize the site of esophageal obstruction, type of obstructing material, and extent of esophageal ulceration. Because of the risk of aspiration pneumonia, the respiratory tract should be evaluated carefully, including auscultation of the heart and lungs and thoracic radiography. In complicated or chronic cases, a CBC and serum biochemistry profile should be performed. Suggestive CBC abnormalities include leukocytosis, left shift, toxic neutrophils, and hyperfibrinogenemia, whereas biochemical abnormalities include hyponatremia, hypochloremia, and hypokalemia secondary to excessive loss of saliva.
Treatment of Esophageal Obstruction in Large Animals
Sedatives and muscle relaxers to relax the esophagus
Passage of oro- or nasogastric tube to relieve esophageal obstruction
Antimicrobial and anti-inflammatory medications
In horses, many cases of esophageal obstruction may resolve spontaneously if feed and water are withheld. Spontaneous resolution can be aided by IV administration of sedatives (eg, xylazine and detomidine). Oxytocin (0.11–0.22 U/kg, IV, once) is useful to relax esophageal smooth muscle. To ensure that the esophageal obstruction has resolved completely, all horses with suspected obstruction should have a nasogastric tube passed into the stomach or an endoscopic examination.
Waiting >4–6 hours before passing a nasogastric tube is not recommended because of the risk of esophageal mucosal ulceration and aspiration pneumonia. Horses that do not respond to conservative management (withdrawal of feed and water, IV administration of sedatives, or oxytocin) should be initially treated with esophageal lavage as follows: After IV administration of sedatives, a nasogastric tube is inserted to the level of the obstruction. Water is delivered to the obstruction site with a stomach pump, and the tube is slowly inserted and withdrawn to lavage the esophagus. The head must be lower than the torso to minimize aspiration of water into the lungs. Lavage via nasogastric tube is successful in at least 90% of cases.


Courtesy of Dr. Jan Hawkins, Purdue University.
For horses unresponsive to standing esophageal lavage, general anesthesia should be considered, with the horse positioned in lateral recumbency and orotracheally intubated. Again, the head must be positioned lower than the torso to prevent water passing into the lungs. A cuffed endotracheal tube (18–22 mm) is inserted into the esophagus as far as possible or to the level of the esophageal obstruction, and the cuff inflated. A nasogastric tube is inserted through the endotracheal tube, and the esophagus is lavaged. Again, resolution of obstruction should be confirmed with endoscopy or passage of the nasogastric tube into the stomach. An esophagotomy to resolve esophageal obstruction is rarely required.

Courtesy of Dr. Jan Hawkins, Purdue University.
All chronic cases of esophageal obstruction should be evaluated endoscopically after successful resolution. These horses frequently have esophageal ulceration that can be circumferential. Severe mucosal ulceration can result in esophageal stricture and repeat obstruction. Endoscopy is also useful to exclude esophageal diverticula, which can predispose to esophageal obstruction. Esophageal diverticula can also be diagnosed with contrast esophagograms.
Horses without mucosal ulceration should be fed water-soaked, complete pelleted feed for at least 7–14 days to minimize the likelihood of repeat esophageal obstruction. Horses with mucosal ulceration should be fed this diet for 60 days, after which follow-up endoscopy should be performed to evaluate whether mucosal ulceration has resolved and esophageal stricture has occurred. Horses with chronic mucosal ulceration with stricture may require surgical management.
Aspiration pneumonia should be managed with antimicrobials and anti-inflammatory drugs. Duration of antimicrobial treatment is typically 7-14 days but may be considerably longer in some cases and depends on the clinical scenario. Commonly used antimicrobials include potassium penicillin G (22,000 U/kg, IV, every 6–12 hours), procaine penicillin G (22,000 U/kg, IM, every 6–12 hours), trimethoprim sulfamethoxazole (30 mg/kg, PO, every 12 hours), and gentamicin sulfate (6.6 mg/kg, IV or IM, every 24 hours). Metronidazole (15 mg/kg, PO, every 6 hours) is useful for management of anaerobic infections. NSAIDS are used with caution and typically only in the acute phase (first several days) because of the risk for gastrointestinal and renal adverse effects, particularly in horses that may already be dehydrated. The most common anti-inflammatory drugs used are phenylbutazone (2.2–4.4 mg/kg, PO or IV, every 12 hours) and flunixin meglumine (1.1 mg/kg, IV, every 12 hours).
In cattle, esophageal obstruction accompanied by bloat (ruminal tympany) is an emergency, and if clinical signs of distress indicate, the bloat must be relieved by trocarization through the left sublumbar fossa. Once tympany has been relieved, solid objects (eg, potatoes) may often be massaged free or spontaneously dislodge as their outer surfaces are softened by saliva. Caution should be used if any attempt is made to push an offending object down the esophagus using a probang; esophageal rupture and fatal septic mediastinitis may result.
Esophageal obstruction in ruminants can be managed with standing esophageal lavage via orogastric tube or while under general anesthesia. Large foreign bodies can often be pushed into the rumen without further problems. Rare cases of esophageal obstruction with foreign bodies may be treated with esophagotomy.
Complications of Esophageal Obstruction
In horses and cattle, aspiration pneumonia and septic pleuropneumonia may be complications of esophageal obstruction, especially in chronic cases. Chronic esophageal obstruction (>24 hours) may be associated with pressure necrosis of the esophageal mucosa because of prolonged contact with the foreign body. Circumferential mucosal damage may contribute to esophageal stricture.


Courtesy of Dr. Jan Hawkins, Purdue University.
An often fatal complication of chronic esophageal obstruction is esophageal rupture. Cervical esophageal rupture can lead to localized cervical cellulitis or septic mediastinitis or pleuropneumonia. Intrathoracic esophageal rupture is typically fatal. Cervical esophageal rupture can be managed by local drainage, wound lavage, and insertion of a nasogastric tube into the rupture site. A traction diverticulum is allowed to form, and the nasogastric tube is removed. Esophageal rupture managed with extraoral alimentation rarely results in esophageal stricture. In cases of septic mediastinitis or pleuropneumonia, euthanasia should be considered because of the difficulty in successfully resolving the bacterial infection.
Esophageal Obstruction Secondary to Extraesophageal Disease
Cervical and prethoracic trauma may result in periesophageal or esophageal fibrosis involving the muscular layer. This can result in esophageal stricture and intermittent or recurrent esophageal obstruction. In some cases, there is no external evidence of cervical or prethoracic trauma. In cases of suspected extraesophageal trauma, endoscopic examination of the esophagus and a contrast esophagogram can be useful diagnostic tools. Once the site of esophageal stricture is identified, some cases of muscular stricture can be resolved with esophageal myotomy or removal of fibrous connective tissue surrounding the esophagus.







