




Strongyloides stercoralis is a zoonotic parasite of dogs and cats with adult parasites that reside in the small intestine. Clinical signs of disease (strongyloidosis) are most commonly observed in young animals and typically characterized by diarrhea and malabsorption. Diagnosis should be based on Baermann examination of fresh feces. Ivermectin or fenbendazole is recommended for treatment.
S stercoralis is a small, slender nematode that when fully mature is ~2 mm long, located at the base of the villi in the distal half of the small intestine of dogs and cats. The worms are almost transparent and all but impossible to see grossly at necropsy. Usually, infections are associated with warm, wet, crowded, unsanitary housing. The species found most often in dogs is identical to that found in humans.

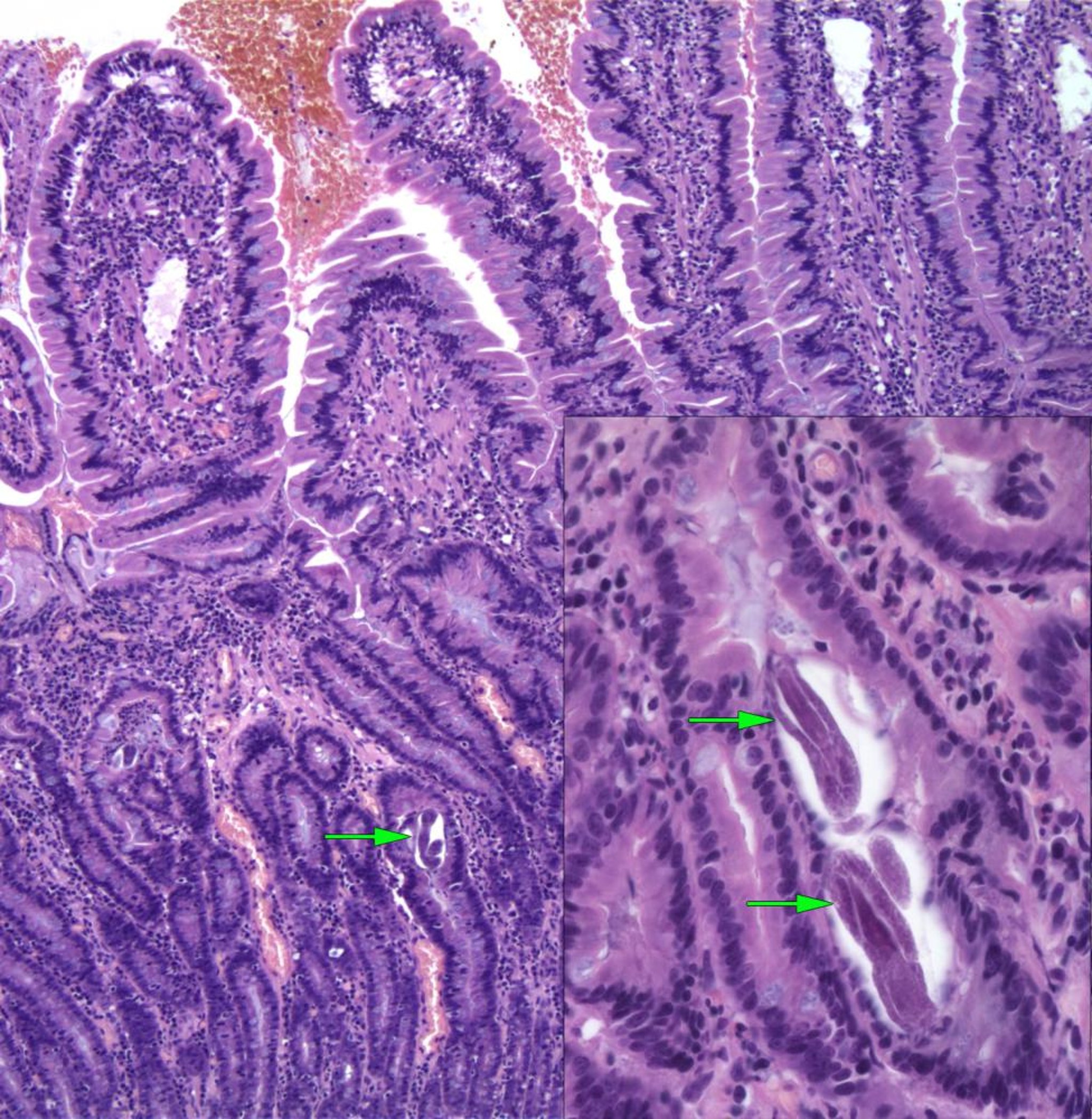
Courtesy of Dr. Jeff Caswell.
The parasitic worms are all females. The eggs embryonate rapidly, and most larvae hatch before being passed in the feces. Under appropriate conditions of warmth and moisture, development in the environment is rapid; the third larval stage may be reached in little more than a day. Some of these larvae develop into infective filariform larvae; others develop into free-living worms that mate and produce progeny similar to that of the parasitic female. The filariform larvae penetrate the skin but also may infect a host via ingestion.
Transmammary transmission is possible. Progeny may be shed in the feces 7–10 days after infection. Autoinfection due to larvae that developed to the infective stage within the GI tract can result in infections in which dogs shed larvae for lengthy periods.
Clinical Findings of Strongyloides sp in Small Animals
Most often, Strongyloides occurs in neonatal puppies and kittens. The presence of clinical signs indicates that a heavy infection has been building up for some weeks. A blood-streaked, mucoid diarrhea, usually present in young animals during hot, humid weather, is characteristic. Emaciation is often prominent, and decreased growth rate may be one of the first clinical signs. Appetite usually is good, and the dog or cat is normally active in the earlier stages of the disease.
In the absence of concurrent secondary infections, there is little or no fever. Usually in advanced stages, there is shallow, rapid breathing and fever, and the prognosis is grave. Autoinfection and systemic infections may be induced by the use of corticosteroids or other factors that affect immunocompetence. There may be larvae in tissues, and these animals are more likely to die. At necropsy, there can be evidence of verminous pneumonia with large areas of consolidation in the lungs as well as marked enteritis with hemorrhage, mucosal exfoliation, and much secretion of mucus.
Diagnosis of Strongyloides sp in Small Animals
Baermann examination of feces
Histopathology of small intestine at postmortem
First-stage Strongyloides larvae (~380 mcm long) may be identified by direct microscopic evaluation of a small quantity of feces. Usually, the Baermann technique is used to separate larvae from fecal material and increase the diagnostic sensitivity. Fecal PCR assay is also offered by some diagnostic laboratories. However, both Baermann and PCR assay examination have low sensitivity (20%–30%) due to inconsistent shedding of larvae; examination of multiple fecal samples increases the diagnostic sensitivity. It is important to use fresh fecal material obtained from an infected dog so the larvae can be easily differentiated from hookworm larvae or free-living soil nematodes.
Occasionally, eggs (50–60 × 30–35 mcm) may be identified by flotation of fresh feces. Adult female worms can be identified by scraping the mucosa of the small intestine. They are only ~2 mm long; however, the presence of eggs in the uterus easily differentiates them from larvae of other nematodes. Histopathology findings in the small intestine wall are characteristic (see figure).
Treatment and Control of Strongyloides sp in Small Animals
Ivermectin or fenbendazole
Supportive care
Environmental management
Poor sanitation and mixing of susceptible and infected dogs can lead to a rapid buildup of the infection in all dogs in a kennel or pen. Dogs with diarrhea should be promptly isolated from dogs that appear healthy. Direct sunlight, increased soil or surface temperatures, and desiccation are deleterious to all free larval stages. Thorough washing of wooden and impervious surfaces with steam or concentrated salt or lime solutions, followed by rinsing with hot water, effectively destroys the parasite. Because the disease in humans can be serious, caution should be exercised when handling infected dogs. The disease in humans (as in dogs) is much more likely to be severe if the patient is immunosuppressed.
Infections in dogs can be treated with ivermectin (0.2 mg/kg, PO, daily, for two consecutive days) or fenbendazole (50 mg/kg/day, PO, for 5 days, repeated 4 weeks later). In cats, fenbendazole (50 mg/kg/day, PO, for 3 days) can be administered. These are not approved regimens in either cats or dogs. In all animals, feces should be examined regularly for at least 6 months after treatment to confirm efficacy.
Key Points
Strongyloides stercoralis (threadworm) is a parasite of dogs and cats acquired via ingestion of infective larvae in milk or the environment, or via penetration of the skin.
Larvae in fresh feces are infective for humans and can cause disease in immunocompromised individuals.
Disease most commonly occurs in puppies and kittens, with diarrhea, malabsorption, and, to a lesser extent, bronchopneumonia, most commonly observed.
Diagnosis is typically based on clinical signs and examination of feces using the Baermann method.
Ivermectin or fenbendazole, combined with supportive care, should be administered for treatment.
For More Information
Intestinal Threadworm. Tropical Council for Companion Animal Parasites Ltd. Accessed Oct 3, 2022. https://www.troccap.com/canine-guidelines/gastrointestinal-parasites/intestinal-threadworm/







