




Giardiasis is an intestinal infection with the protozoan flagellate parasite Giardia spp. Most infections of veterinary health importance are by G duodenalis, a species complex of different genotypes that tend to show host specificity; production animals, companion animals, and wildlife can all be infected. In general, the clinical signs of giardiasis are abdominal discomfort and diarrhea, often with steatorrhea. Diagnosis is usually by demonstration of cysts or antigens in fecal samples. Treatment regimens are variable and depend on specific indications. Hygiene measures are an essential component of control.
Giardiasis is an intestinal infection with the protozoan parasite Giardia spp. Giardia infection occurs worldwide in most domestic and wild mammals and many birds. It is also very common in humans. In some animals, particularly ruminants but also wild mammals, Giardia infection commonly occurs without overt or apparent clinical signs.
Three major groups of Giardia have been described based on morphology of the vegetative stage (trophozoite): G muris from rodents, G agilis from amphibians, and a third group from various warm-blooded animals. This third group includes at least four species, including G ardeae and G psittaci from birds, G microti from muskrats and voles, and G duodenalis (also known as G intestinalis and G lamblia). This latter species comprises a complex of eight different assemblages, which have also been described as separate species, and among them they have a wide mammalian host range.
In general, when veterinarians and physicians refer to Giardia or giardiasis, they are referring to G duodenalis and this is the focus of this topic. Among the eight assemblages of G duodenalis, some (A and B) have a relatively wide host range and may infect humans and a range of animals, whereas other assemblages are more host specific: assemblages C and D infect dogs, assemblage E infects livestock (pigs, cattle, sheep, goats), assemblage F infects cats, assemblage G infects rodents, and assemblage H infects pinnipeds. Some of the assemblages themselves have been subdivided into genotypes with different genetic characteristics and host predilections. For example, assemblage A1 predominantly infects domestic animals but is common in wildlife and also infects humans; assemblage A2 predominantly infects humans but also infects domestic animals and occurs rarely in wildlife; Assemblage A3 predominantly infects wildlife and occurs occasionally in domestic animals but seldom infects humans. This division into Assemblages and genotypes is confusing, but it is important for understanding the epidemiology and the possibility of between-species transmission, particularly zoonotic transmission, such as from domestic animals to their owners.
Surveys conducted in different parts of the world have reported point prevalence estimates of Giardia infection of around 10%–30% for dogs and somewhat lower for cats, with higher rates of infection in younger animals. However, there are wide variations between studies. Dogs shedding Giardia cysts frequently have no clinical signs, and the relevance of continually treating dogs that seem to be permanently infected, but apparently healthy, remains a subject of debate. Various other small pet animals (such as rabbits and guinea pigs) have also been shown to be susceptible to Giardia infection. Among rodents, chinchillas are particularly notable for a high occurrence of infection, with clinical signs, and the predominance of assemblage B infections which, at some commonly used typing genes, are identical to the assemblage B infections reported in humans. Thus, it appears that although zoonotic transmission of Giardia to humans is generally rare, it may be more likely to occur from infections in chinchillas.
In small ruminants (sheep and goats), data tend to indicate an occurrence of around 20%–25%, ranging from < 10% to >40%, with similar data for cattle. On farms where Giardia infection has been diagnosed in ruminant stock, a cumulative occurrence of close to 100% may be expected. In general, very young animals (neonates) are less likely to be infected, although animals < 6 months of age tend to be more susceptible to infection with signs of disease. Frequently, however, even infections with very high cyst excretion are not associated with clinical signs. Nevertheless, diarrhea, weight loss, ill thrift, and even death have also been associated with Giardia infection in some animals.
In pigs, the occurrence of Giardia tends to be lower, at around 15%, but is age related, with low infection rates (around 5%) recorded from piglets and sows and higher rates reported from starter pigs and fatteners (15%–30%). Many infections in pigs seem to be asymptomatic. In horses, occurrence rates of < 10% (from around 0.5% to 20%) seem usual, with infection more likely in foals, but with symptomatic giardiasis only rarely reported.

Cycle and Transmission of Giardiasis in Animals
The life cycle of Giardia is relatively simple. The flagellate, vegetative stage (trophozoites) of Giardia inhabit the lumen of the small intestine, where they may attach to the brush border of epithelial cells via the ventral disk, absorb nutrients, and multiply by binary fission. There are no intracellular stages. The trophozoites usually live in the proximal portion of the small intestine and migrate down the intestine during the course of infection, encysting in the small or large intestine. The prepatent period is generally 3–10 days.
The cysts are passed in the feces and are immediately infectious. Cyst shedding may be continual over several days and weeks but is often intermittent, especially in the chronic phase of infection. The cyst is the infective stage and can survive for several weeks, or even months, in an appropriate (cool and damp) environment. Although trophozoites may be passed in the feces, especially during bouts of severe diarrhea, they do not survive for long in the environment and, if ingested, they are not able to infect a new host.
Transmission occurs via the fecal-oral route, either by direct contact with an infected host that is contaminated with infective cysts or through a contaminated environment. Characteristics that facilitate infection include the high and prolonged excretion of environmentally robust cysts by infected animals and the low infectious dose. Giardia cysts are infectious immediately after excretion and are very resistant, resulting in a gradual increase in environmental infection pressure. High humidity facilitates survival of cysts in the environment. Overcrowding favors transmission.
Pathogenesis of Giardiasis in Animals
Giardia infections cause an increase in epithelial permeability, increased numbers of intraepithelial lymphocytes, and activation of T lymphocytes. Trophozoite toxins and T-cell activation initiate a diffuse shortening of brush border microvilli and decreased activity of the small-intestinal brush border enzymes, especially lipase, some proteases, and disaccharidases. The diffuse microvillus shortening leads to a decrease in overall absorptive area in the small intestine and thus an impaired intake of water, electrolytes, and nutrients. In addition, the proteins secreted by Giardia trophozoites contribute to degrading the intestinal mucous barriers and disrupting the intestinal intracellular junctions. The combined effect of decreased resorption, brush-border enzyme deficiencies, and a lack of integrity between cells of the intestine results in dysregulation of the absorption and barrier functions of the intestinal epithelium, resulting in malabsorptive diarrhea.
The reduced activity of lipase and the increased production of mucin by goblet cells may explain the steatorrhea and mucous diarrhea that has frequently been described in symptomatic giardiasis. Giardia infection has, in some circumstances, been associated with a lower likelihood of viral and bacterial infection, possibly via immunologic pathways.
Clinical Findings and Lesions of Giardiasis in Animals
Presentation of Giardia infections seems to vary both between and within animal groups. Giardia infection in cats, or, more typically, dogs may be present without clinical signs and diagnosed only during routine fecal checks. However, it may also be associated with chronic diarrhea or steatorrhea, which can be continual or intermittent, particularly in puppies and kittens. Weight loss may also occur. In clinical giardiasis in cats and dogs, feces usually are soft, poorly formed, pale, malodorous, contain mucus, and appear fatty. Watery diarrhea is unusual, and blood is usually not present in feces. Vomiting is unusual but may occur.
Giardiasis must be differentiated from other causes of nutrient malassimilation (eg, exocrine pancreatic insufficiency and intestinal malabsorption). Clinical laboratory findings are usually normal. Among small animal pets, chinchillas appear to be particularly prone to Giardia infection, especially kits; although clinical signs of infection appear to be relatively common, infection in apparently healthy animals has also been reported frequently in surveys.
In calves, and to a lesser extent in other production animals, giardiasis can result in diarrhea that does not respond to antimicrobial or coccidiostatic treatment. The excretion of pasty to fluid feces with a mucoid appearance may indicate giardiasis, especially when the diarrhea occurs in young animals (1–6 months old). Experimental infection of goat kids, lambs, and calves resulted in a decreased feed efficiency and subsequently a decreased weight gain.1 However, as with other animals, apparently asymptomatic excretion also occurs; very large numbers of cysts can be observed in the feces of cows and sheep with no apparent clinical signs.
Gross intestinal lesions are seldom evident, although microscopic lesions, consisting of villous atrophy and cuboidal enterocytes, may be present.
References
Koudela B, Vitovec J. Experimental giardiasis in goat kids. Vet Parasitol. 1998; Jan 15;74(1):9-18. doi: 10.1016/s0304-4017(97)00146-5.
Diagnosis of Giardiasis in Animals
Detection of Giardia cysts or trophozoites in fecal samples
Detection of Giardia antigen in fecal samples
The two main methods to diagnose Giardia infection are identification of Giardia cysts, and considerably less frequently, trophozoites in fecal samples and detection of Giardia antigen in fecal samples.
Giardia cysts are oval (9–15 × 7–10 mcm) and can be detected in feces concentrated by the centrifugation-flotation technique using zinc sulfate (specific gravity 1.18). Sodium chloride, sucrose, or sodium nitrate flotation media may be too hypertonic and distort the cysts. Staining cysts with iodine aids in identification.

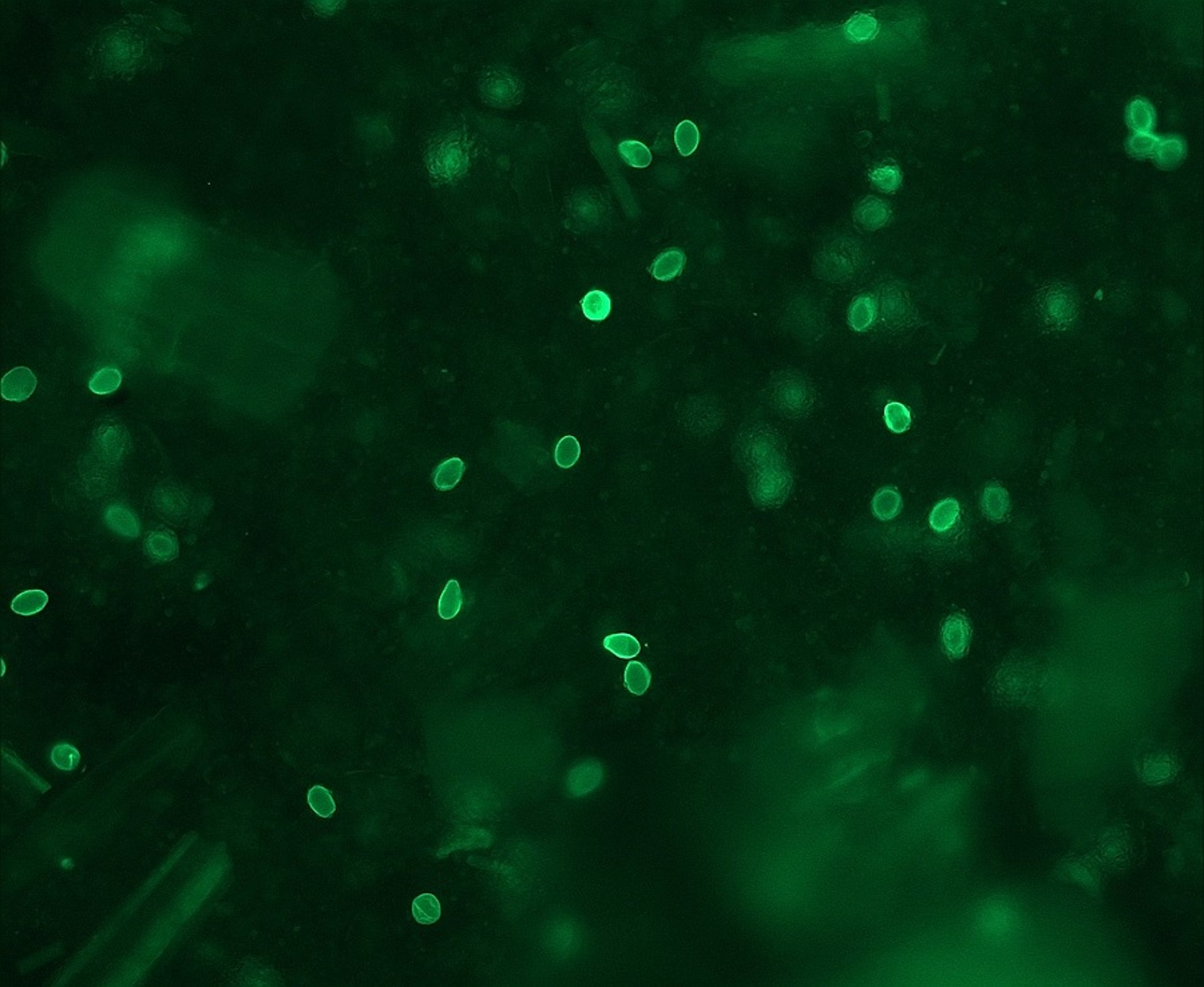
Courtesy of Dr. Lucy Robertson.

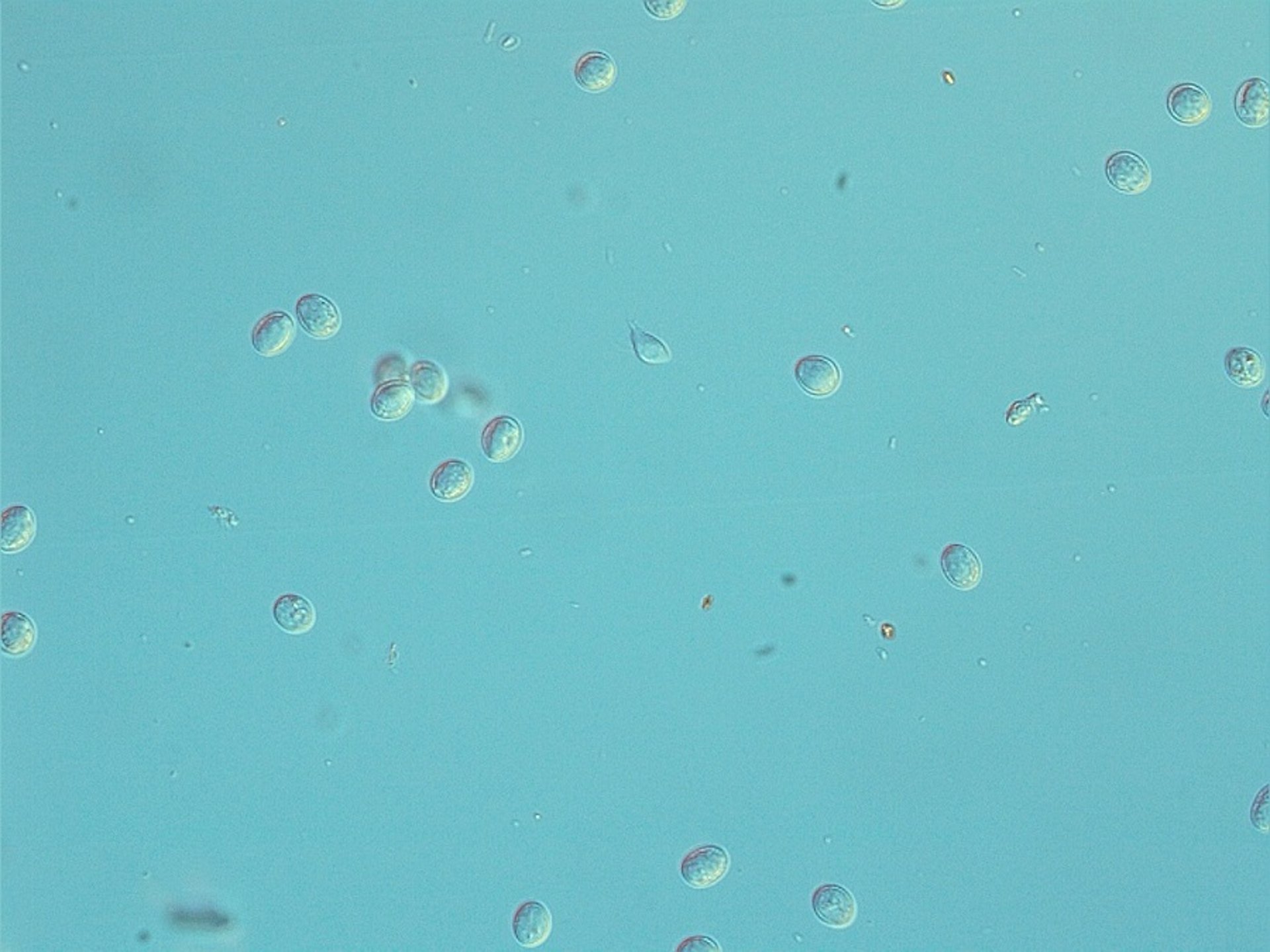
Courtesy of Dr. Lucy Robertson.
Because Giardia cysts are excreted intermittently, infections may be missed; therefore, several fecal examinations should be performed if giardiasis is suspected (eg, three samples collected over 3–5 consecutive days). Because Giardia cysts rupture if dried or exposed to heat or extreme cold, the empty cysts may be difficult to see and may not have the same flotation characteristics as intact cysts.
For laboratories with a fluorescent microscope, an immunofluorescent antibody staining of the cyst walls (IFAT) may be a rapid and easy way to detect them. Several commercial IFAT kits are available, with the antibodies usually coupled to fluorescein isothiocyanate.
Although cysts are the transmission stage of Giardia, and most often observed in feces, very occasionally the motile, piriform trophozoites (12–18 × 7–10 mcm) may be observed in saline smears of loose or watery feces. They should not be confused with yeast or with trichomonads, which have a single rather than double nucleus, an undulating membrane, and no concave ventral surface. The "falling leaf" swimming motion of Giardia trophozoites is also characteristic.
Giardia antigen that occurs in feces can be a useful method to diagnose Giardia infection, should infection be suspected but no cysts observed on microscopic examination. Microtiter plate-format ELISA tests to diagnose Giardia infection in animals are apparently not commercially available, but some veterinarians have reported success with those designed for use in humans working satisfactorily with dog samples, or in-house plate-format ELISA tests can be used.
More commonly, and available from different commercial suppliers, are ELISA-based in-clinic tests, mostly for dog samples, that use lateral flow technology; these are simple to use and may provide a result within minutes. Different tests vary in their sensitivity and specificity; information about these differences is proprietary. Given the relative expense and defined shelf-life of these tests, it may be useful to investigate before investing in a particular test and to compare with other tests (such as IFAT or in-house plate-format ELISA) as a component of ongoing quality control. Molecular methods (PCR array) are also available for diagnosis but are rarely used in a routine diagnostic setting.
In some situations (eg, in outbreaks or if a human case and an infected animal are in the same household), determining which assemblage of Giardia is causing the infection may be relevant. Different protocols to identify the various assemblages have been published; however, relatively large numbers of nucleated cysts may be necessary for successful DNA extraction and amplification at target genes. Unequivocal results may be elusive, particularly in dogs.
Treatment of Giardiasis in Animals
Address clinical signs versus achieve cessation of cyst shedding
Fenbendazole, metronidazole, or albendazole
There is some debate concerning whether animals without clinical signs that continue to shed Giardia cysts, even after treatment, should continue to be treated. Such cases need to be evaluated on an individual basis, preferably using a clinical decision-tree type format. Indeed, some guidelines advise against treating animals with subclinical infection; however, risk of transmission to other susceptible hosts) should be considered, and strict hygiene measures are relevant. Drug treatment regimens should probably aim to stop clinical signs rather than eliminate cyst shedding. Treatment approval varies between country; no drugs are approved for treatment of giardiasis in dogs and cats in the US, and no drug is licensed for treatment of Giardia infection in ruminants or other livestock.
Fenbendazole (50 mg/kg per day, for 3–10 days) is approved for treatment of dogs in most countries in Europe (although only for 3 days of treatment in some countries) and can be recommended for cats. It is reported to stop shedding of Giardia cysts in dogs, with no adverse effects reported, and is safe for pregnant and lactating animals. Fenbendazole is therefore considered a first-line drug for treatment, but metronidazole can be considered, either alone or together with fenbendazole, should clinical signs continue. However, although successful treatment of dogs with metronidazole has been reported (25 mg/kg, every 12 hours, or 50 mg/kg per day, for 5 days), and it is licensed in most European countries for treating both dogs and cats, it has been associated with serious adverse effects of the CNS in dogs after chronic treatment or high doses.
Albendazole is not recommended for use in dogs and cats because of possible bone marrow suppression. A combination of praziquantel (5 mg/kg), pyrantel (15 mg/kg), and febantel (15 mg/kg), once a day, for 3 days, has also been shown to be effective for treating dogs and is licensed in most European countries and also outside the EU. Other agents have also been tried experimentally, especially when more usual treatment regimens have been unsuccessful. These include, but are not limited to, azithromycin (10 mg/kg per day, for 5 days), nitazoxanide (75 mg/kg per day, for 14 days), tinidazole (50 mg/kg per day, for 5 days), secnidazole (30 mg/kg, two single doses 2 weeks apart), and chloroquine (2.5 mg/kg, every 12 hours, for 5 days). In general, published reports of such investigations indicate that the novel treatment has been successful.
Although there are no licensed treatments for Giardia in livestock, both fenbendazole and albendazole (5–20 mg/kg per day, for 3 days) have been shown to reduce cyst shedding in both sheep and cattle and provide some clinical benefit (decreased diarrhea and increase weight gain). Paromomycin (50–75 mg/kg, per day, for 5 days) has also been found to be efficacious in cattle. Other treatments have been tried on livestock and have been reported to be effective (eg, secnidazole, 10 mg/kg).
That different treatments are often tried indicates frequent frustration with cyst shedding, and sometimes clinical signs, continuing after treatment. It is unclear whether this indicates treatment failure or re-infection, although both may play a role.
Supportive or supplementary therapies such as probiotic treatment have been suggested, but there is little reliable evidence that such therapies are effective.
Control of Giardiasis in Animals
Giardia cysts are immediately infective when passed in the feces and survive well in the environment, particularly in damp and cool conditions in which cysts may stay infective for months. Cysts are a source of infection and reinfection for animals, particularly those in crowded conditions (eg, kennels, catteries, or intensive rearing systems for production animals). Thus, control should include removing feces as soon as possible (at least daily) and disposing of potentially infectious waste. Infected dogs and cats should be bathed to remove cysts from the hair coat, and use of a shampoo containing chlorhexidine digluconate has been recommended. Prompt and frequent removal of feces limits environmental contamination, as does subsequent disinfection. Cysts are inactivated by most quaternary ammonium compounds, steam, and boiling water.
Although no disinfectants are registered to kill Giardia cysts, regular frequent washing and drying of blankets, bedding, and food and water containers, along with other normal good hygiene practices, can limit transmission to other hosts and reinfection after recovery. Isolating of diarrheic pets or diagnosed carriers will also limit transmission.
To increase the efficacy of disinfectants, solutions should be left for 5–20 minutes before being rinsed off contaminated surfaces. Disinfection of grass yards or runs is impossible, and these areas should be considered contaminated for at least a month after infected dogs were last present. Cysts are susceptible to desiccation, and areas should be allowed to dry thoroughly after cleaning.
Key Points
Giardia duodenalis infects a wide range of hosts, including humans and most pets and livestock, although not all isolates are infectious to all animals.
Many infections are subclinical, and clinical infections are generally associated with chronic diarrhea with steatorrhea.
Various diagnostic options are available and are generally focused on identification of either transmission stages (cysts) in feces or fecal antigen testing.
Various treatment options are available, some of which are off-label. Drug treatment should aim at suppressing clinical signs rather than halting shedding of cysts, and good hygiene practices should be considered an essential component of control.
For More Information
ESCCAP: GL6 Control of Intestinal Protozoa in Dogs and Cats. Currently available in 9 languages (Dutch, English, French, German, Italian, Polish, Spanish, Swiss French, Swiss German). English version updated in 2018.
CAPC: Giardia (Dog, updated 2019); (Cat, updated 2018).
Scorza, V. (2013). Giardiasis: an overview. Clinicians Brief.
Tysnes KR, Skancke E, Robertson LJ. Subclinical Giardia in dogs: a veterinary conundrum relevant to human infection. Trends in Parasitol. 2014;30(11):520-527. doi:10.1016/j.pt.2014.08.007
Also see pet health content regarding giardiasis in dogs, cats, and horses.




