




Ascites syndrome in poultry refers to right heart failure, usually due to pulmonary hypertension. The syndrome is most often associated with high altitude, rapid growth rate, or cold stress as chicks. Death occurs as an outbreak in the case of environmental predisposing factors, or sporadically in individual cases of rapid growth. Necropsy findings include ascites, hydropericardium, lung and liver congestion.
Ascites is an accumulation of noninflammatory transudate in one or more of the peritoneal cavities or potential spaces. The fluid accumulates most frequently in the two ventral hepatic, peritoneal, or pericardial spaces and may contain yellow fibrin clots. Although ascites can result from increased vascular hydrostatic pressure, vascular damage, increased tissue oncotic pressure, or decreased vascular oncotic (usually colloidal) pressure, in poultry it is most commonly associated with increased venous hydrostatic pressure. The causative venous hypertension is usually due to right ventricular failure (RVF), but it is also associated with primary hepatic fibrosis. It is well documented that most cases are due to a genetic predisposition to pulmonary hypertension, which progresses to congestive heart failure and terminal ascites in many cases.
Pulmonary hypertension occurs frequently in chickens secondary to high altitude–associated hypoxia, with resultant polycythemia and increased blood viscosity. It also occurs frequently secondary to the RBC rigidity of sodium toxicosis and less frequently from lung pathology. In poultry, liver damage may also be due to aflatoxin or to toxins from plants such as Crotalaria. In broiler chickens, obstructive cholangiohepatitis (due to Clostridium perfringensinfection) is the most common cause of the liver damage, which results in ascites. In both meat-type ducks and breeders, amyloidosis of the liver may also cause ascites.
When ascites occurs at high altitudes in meat-type chickens, which have a high metabolic oxygen requirement, it is usually due to primary or spontaneous pulmonary hypertension because of insufficient capacity of the pulmonary capillaries. Cold stress, even briefly, during the first 3 weeks of life is known to markedly increase the predisposition to ascites syndrome.
Pathogenesis and Epidemiology of Ascites Syndrome in Poultry
Ascites syndrome results from increased pressure in the pulmonary arteries when the heart tries to pump more blood through the lungs to meet the body’s oxygen requirement. The resultant volume and pressure overload on the right ventricle lead to dilatation and hypertrophy of the right ventricular wall, valvular insufficiency, RVF, and ascites.
Bird lungs are rigid and fixed in the thoracic cavity. The capillaries can expand very little to accommodate increased blood flow. Lung size in proportion to body weight, and particularly to muscle mass, decreases as meat-type chickens grow. Increased blood flow results in primary pulmonary hypertension and cor pulmonale.
Predisposing factors that increase oxygen demand (eg, cold), decrease oxygen-carrying capacity of the blood (eg, acidosis, carbon monoxide), increase blood volume (eg, sodium), or interfere with blood flow through the lung (eg, lung pathology that narrows or occludes capillaries, increased RBC rigidity, or polycythemia with increased blood viscosity) may result in flock outbreaks of ascites syndrome with or without ascites. Sporadic individual cases of RVF and ascites without these predisposing factors can occur in fast-growing broilers.
The incidence of ascites syndrome is > 2% in some broiler flocks.
Clinical Findings of Ascites Syndrome in Poultry
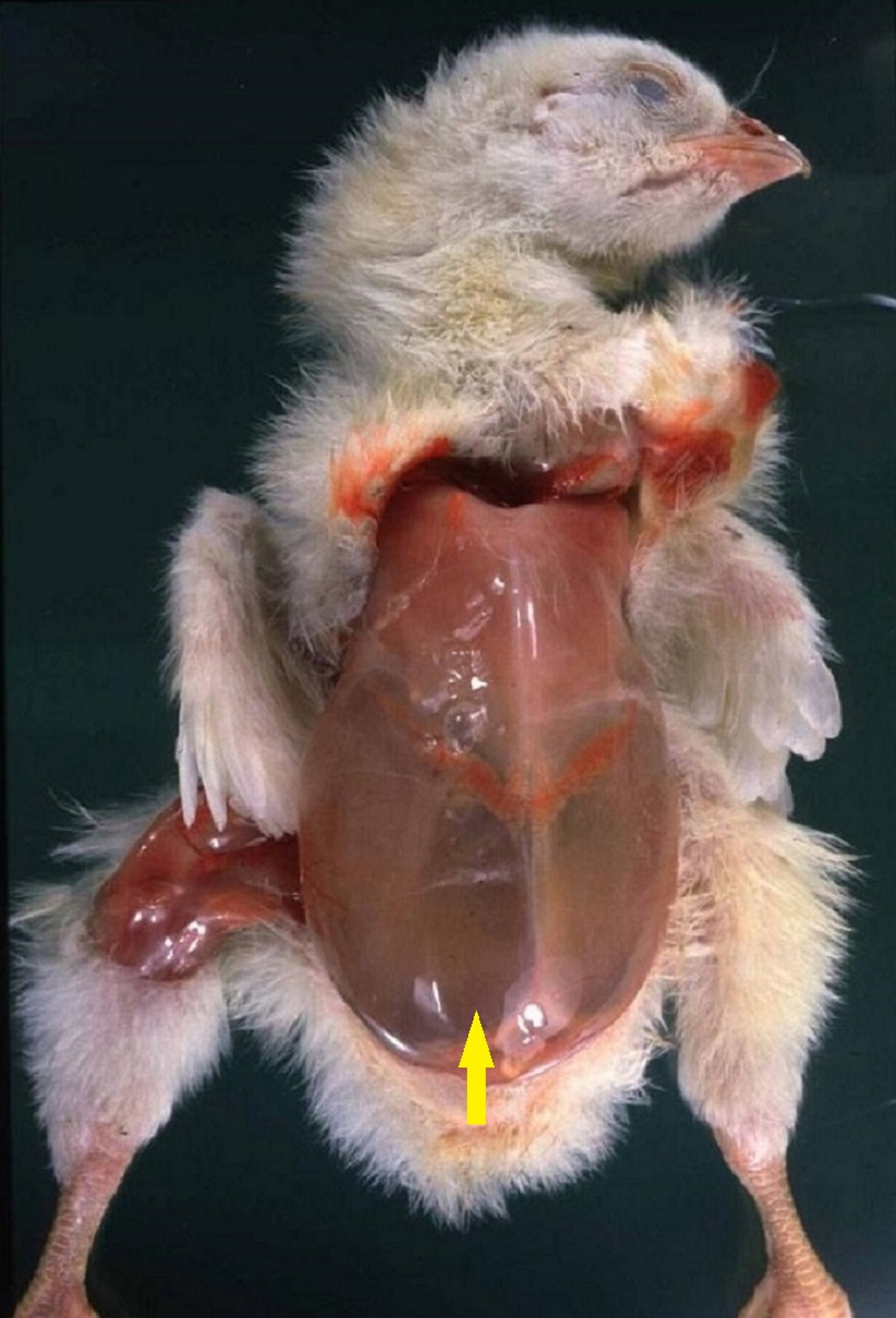
Occasionally, young broilers develop ascites syndrome, particularly if increased sodium or lung pathology (eg, aspergillosis) is involved; however, mortality is greatest after the age of 5 weeks. There are no clinical signs until RVF occurs and ascites develops. Clinically affected broilers are cyanotic; the abdominal skin may be red, and the peripheral vessels congested.
Because growth stops as RVF develops, affected broilers may be smaller than their penmates. However, rapid growth rate is a known predisposing factor, and sometimes the largest broilers are affected, with occurrence in males more frequent than in females. The ascites increases the respiratory rate and decreases exercise tolerance. Affected broilers frequently die on their backs.
Not all broilers that die from ascites syndrome actually have ascites. Death may occur suddenly, before clinical signs are observed or ascites develops.
Lesions

Courtesy of Dr. Billy M. Hargis.

Courtesy of Dr. Billy M. Hargis.
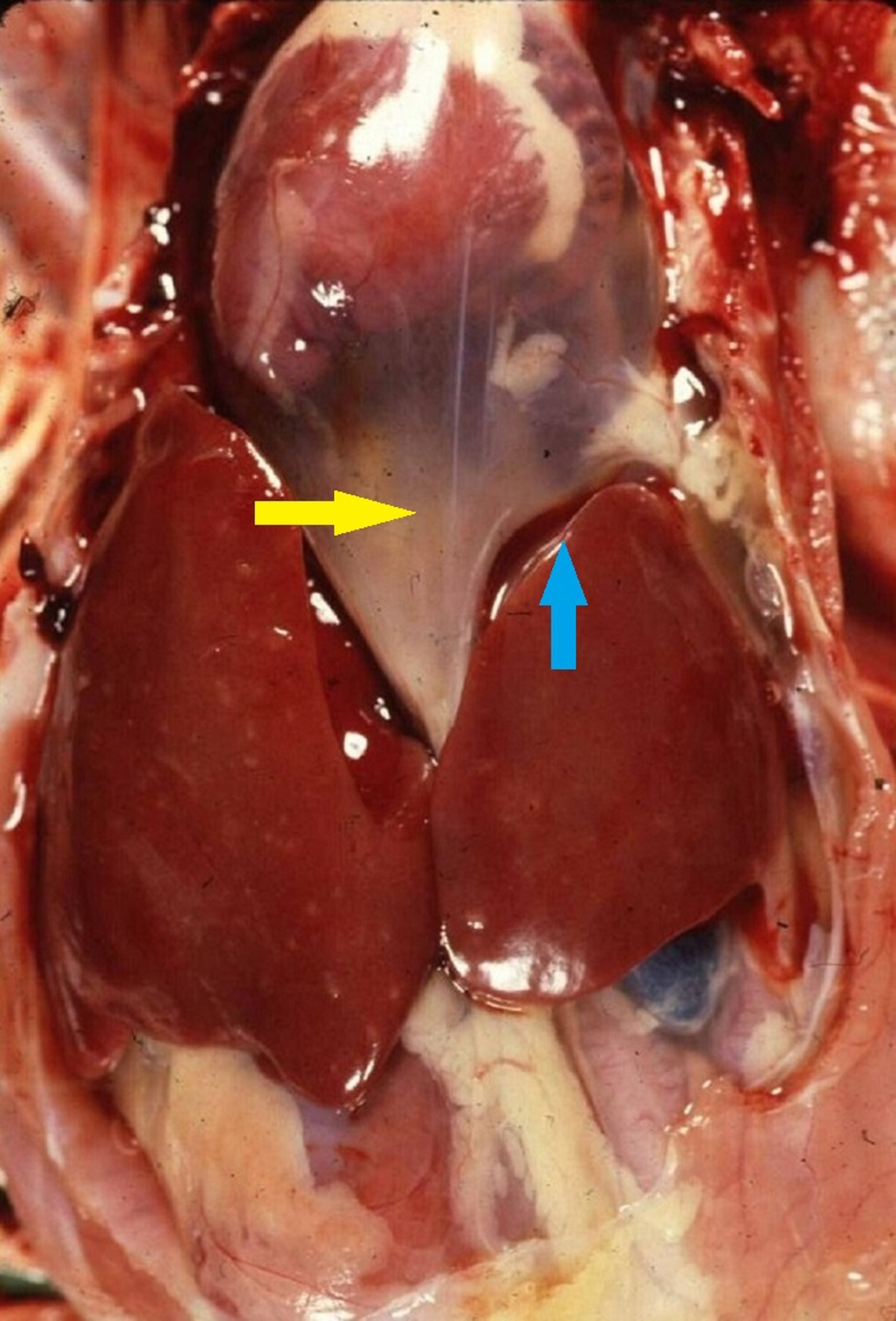
Post-mortem findings of ascites syndrome include variable amounts of clear, yellow fluid and clots of fibrin in the hepatoperitoneal spaces and pericardium, and a swollen liver. Hydropericardium is mild to marked; occasionally there is pericarditis with adhesions, usually from secondary infections. The liver may be firm with irregular margins due to edema, have clotted protein adherent to the surface, may be nodular, shrunken or even white with subcapsular edema and a thickened capsule. Right ventricular dilatation and mild to marked hypertrophy of the right ventricular wall may be evident. The right atrium and vena cava are markedly dilated in most cases. Occasionally, thinning of the left ventricle is observed. The lungs are extremely congested and edematous.
Diagnosis of Ascites Syndrome in Poultry
Necropsy findings
Broilers that die from ascites syndrome or suddenly as the result of RVF or pulmonary hypertension can be identified at necropsy by the lesions described above. If the wall of the right ventricle is enlarged or thickened, the broiler has probably died from ascites syndrome, even if there is no fluid in the body or heart sac.
Gross pathology is usually diagnostic, and follow-up testing for complicating factors (such as mycotoxicosis, or viral or bacterial etiologies) is only occasionally indicated.
Control of Ascites Syndrome in Poultry
Decreasing the metabolic oxygen requirement
Controlling environmental factors to preventing excessive loss of body heat
Decreasing the birds’ metabolic oxygen requirement by slowing growth or decreasing feed density or availability can prevent ascites that is due to pulmonary hypertension.
Environmental temperature, humidity, and air movement should be controlled to prevent excessive loss of body heat, particularly in the early neonatal period. Even brief exposure to cold stress during the first weeks of life is known to predispose flocks to this condition.
Ascites due to other factors (eg, sodium, lung damage, or liver damage) can be prevented by avoidance of the etiologic agents involved. Altitudes > 3,000 feet (900 meters) are unsatisfactory for meat-type chickens, and growth must be slowed to prevent mortality. More care to prevent chilling is also necessary at higher altitudes.
Research has demonstrated that broilers can be genetically selected for both resistance and susceptibility to pulmonary hypertension and associated ascites. Some breeders include oxygen saturation (SpO2) values in genetic selection indices. The total percentage of mortality or condemnations at processing may be decreased by improvements in environmental conditions (better ventilation, regulated temperature, lower amount of dust).
Key Points
Ascites syndrome in poultry results from pulmonary hypertension and secondary right heart failure.
Rapidly growing broilers, those raised at altitude > 3,000 feet, or chicks exposed to cold as neonates are most susceptible.
Treatment is not pursued; diagnosis is made at necropsy and prevention of risk factors is the primary management strategy.







