

Equine asthma is a chronic, nonseptic respiratory disease of adult horses. Although a heterogenous disease, all horses with asthma share common features of airway inflammation, airway hyperresponsiveness, and airway remodeling. Diagnosis of equine asthma is most often based on clinical signs and cytological evaluation of bronchoalveolar lavage fluid. Reducing allergen exposure is essential in managing horses with asthma. Medical management includes treatment with systemic or inhaled corticosteroids and bronchodilators.
Equine asthma, a chronic, allergen-mediated inflammatory disease of the lower airways, is highly prevalent in adult horses of varying ages. This condition has been associated with many names including heaves, broken wind, and chronic obstructive pulmonary disease (COPD). Most recently, "equine asthma" has been adopted as the terminology to encompass the three related conditions of inflammatory airway disease (IAD), recurrent airway obstruction (RAO), and summer pasture recurrent airway obstruction (SPRAO). Mild-moderate asthma represents horses with IAD and severe asthma represents horses previously labelled as having RAO (heaves).




Pathophysiology of Asthma in Horses
Three components contribute to the pathophysiology of equine asthma: airway inflammation, airway hyperresponsiveness, and airway remodeling. Neutrophilic airway inflammation characterizes severe equine asthma while mild-moderate asthma can present as any combination of neutrophilic, eosinophilic, or mastocytic inflammation. Mucus hypersecretion accompanies airway inflammation, causing lower airway obstruction. Inflammatory mediators, bronchospasm, and dysfunction in airway smooth muscle relaxation contribute to airway hyperresponsiveness. Airway remodeling is most consistently observed with severe asthma. Chronic inflammation causes recurrent injury to and remodeling of the airway walls which ultimately results in narrowing of the airway lumen. These changes are irreversible in longstanding or severe cases of equine asthma. The magnitude of airway wall remodeling correlates most consistently with the magnitude of airway hyperreactivity.
In the asthmatic horse, these pathophysiologic effects manifest as expiratory airflow limitations and resultant increased work of breathing, air trapping in the lung periphery, and hypoxemia secondary to altered gas exchange. In horses with severe asthma, the disease is episodic and progressive; however, it can be controlled. In horses with mild-moderate asthma, treatment may prevent the progression to severe asthma.
Etiology of Asthma in Horses
The etiology of equine asthma is multifactorial and best understood for horses suffering from severe asthma. Equine asthma is an allergen-mediated condition involving hypersensitivity of some horses to aerosolized substances in the environment—particularly the components of respirable dust in hay or bedding (molds, endotoxin, micro-organisms, pollen) or noxious gases or pollutants. Most horses exhibit clinical signs when stabled and fed hay, whereas elimination of these inciting factors results in remission or attenuation of clinical signs. The average age at onset of severe asthma is 9 years. Approximately 17% of mature horses in northern, temperate geographical areas have some allergen-induced lower airway inflammation.(1, 2, 3) Although there does not appear to be a gender or breed predilection for this condition, heritable predispositions are described.
A subtype of severe asthma (SPRAO) is recognized in adult horses at pasture in hot, humid climates. This subtype of asthma is most often recognized in the southeastern US but has also been described in horses in the Pacific Northwest and UK. In these horses, manifestation of clinical disease is seasonal (primarily summer); the exact inciting environmental factors are unknown, but grass pollen or fungal spores are suspected.
Mild-moderate asthma affects up to 80% of athletic horses (pleasure and racehorses)(1, 2, 3) at some point in their life and is a common cause of impaired performance and interruption of training. Asthma in these horses represents a heterogeneous inflammatory condition of the lower respiratory tract whose etiology most likely shares certain aspects with severe asthma. In some horses mild asthma may progress to severe asthma later in life, while in others the condition is transient. An allergen-mediated component is suspected in many horses with mild asthma. Additional factors with a proposed link to the development of mild-moderate asthma include infection with respiratory viral (EHV-2, equine rhinitis virus A variant) or bacterial (Streptococcus spp) pathogens, or recurrent pulmonary stress associated with strenuous training.
Clinical Findings of Asthma in Horses


Courtesy of Dr. Bonnie R. Rush.


Courtesy of Dr. Thomas Lane.


Severe Asthma (RAO)
Horses with severe asthma demonstrate variable and episodic periods of expiratory dyspnea at rest with frequent coughing episodes. Exercise intolerance and nasal discharge are common findings. In controlled cases, these signs may be subtle, with horses experiencing periods of disease remission. In horses with longstanding or poorly controlled disease, the characteristic “heave line” may develop, demonstrating hypertrophy of the abdominal muscles of expiration, and body condition is often poor. Thoracic auscultation with or without a rebreathing examination allows for identification of characteristic expiratory wheezes. A rebreathing examination should not be performed in a dyspneic animal. Additional findings include a prolonged expiratory phase of respiration, tracheal rattle, and over-expanded lung fields secondary to air trapping in peripheral airways. Crackles may also be present and are associated with excessive mucus production.
Mild-moderate Asthma (IAD)
In contrast, mild-moderate asthma typically presents with nonspecific complaints of poor performance or exercise intolerance at maximal work. Increased respiratory effort at rest is not typical and distinguishes this condition from severe asthma. Similarly, characteristic expiratory wheezes are less pronounced and are rarely identified without a rebreathing examination. Horses with moderate asthma may present with occasional cough or mild tachypnea at rest and mucoid nasal discharge is occasionally noted. In mild cases, respiratory compromise is often unrecognized at light work, making diagnosis challenging. Horses with any form of equine asthma are not typically febrile unless secondary bacterial pneumonia has developed.
Diagnosis of Asthma in Horses
Bronchoalveolar lavage
Endoscopy
Response to therapeutic trial
The goal in the diagnostic approach to equine asthma is to identify and characterize lower airway inflammation while also excluding other causes of lower airway disease. A thorough history and identification of characteristic clinical signs is critical and may allow for a presumptive diagnosis of equine asthma in more severe cases. Ancillary tests are important in horses presenting with mild-moderate asthma or with subtle clinical signs and are essential for achieving a definitive diagnosis.
Bronchoalveolar lavage (BAL) is the test of choice for identifying and characterizing lower airway inflammation. BAL is not innocuous in horses that are dyspneic at rest; it may not, therefore, be clinically appropriate in horses with severe, uncontrolled asthma. In these horses, clinical improvement after administration of a fast-acting bronchodilator may be used to support diagnosis of severe equine asthma.
Cytologic findings on BAL fluid analysis are consistent with neutrophilic inflammation (severe asthma) or neutrophilic, eosinophilic, and/or mastocytic inflammation (mild-moderate asthma). Curschmann spirals (inspissated mucus/cellular casts) may be seen in horses with excessive mucus obstructing the small airways. Hemosiderin (bi-product of red blood cell breakdown) and hemosiderophages (alveolar macrophages containing hemosiderin) are occasionally identified in the BAL fluid of horses with asthma, particularly when Wright Giemsa or Perls' Prussian Blue cytological staining is used. The identification of hemosiderophages is routinely used to diagnose Exercise Induced Pulmonary Hemorrhage (EIPH) in horses. EIPH is a condition associated with bleeding into the lungs in strenuously exercising horses such as race horses or upper level endurance horses. The relationship between asthma and EIPH remains incompletely defined in horses. Although asthma has been associated with an increased risk of EIPH in some studies, this relationship has not been consistently observed (4), and hemosiderophages may also be identified in the BAL of sedentary horses with severe asthma and no history of EIPH.(5) In horses with an eosinophilic BAL, important differentials besides asthma include parasitic pulmonary disease and hypersensitivity pneumonitis. It should be noted that concurrent identification of peripheral eosinophilia, miliary pulmonary opacities, or eosinophilic pulmonary granulomas are not consistent with a diagnosis of eosinophilic equine asthma.

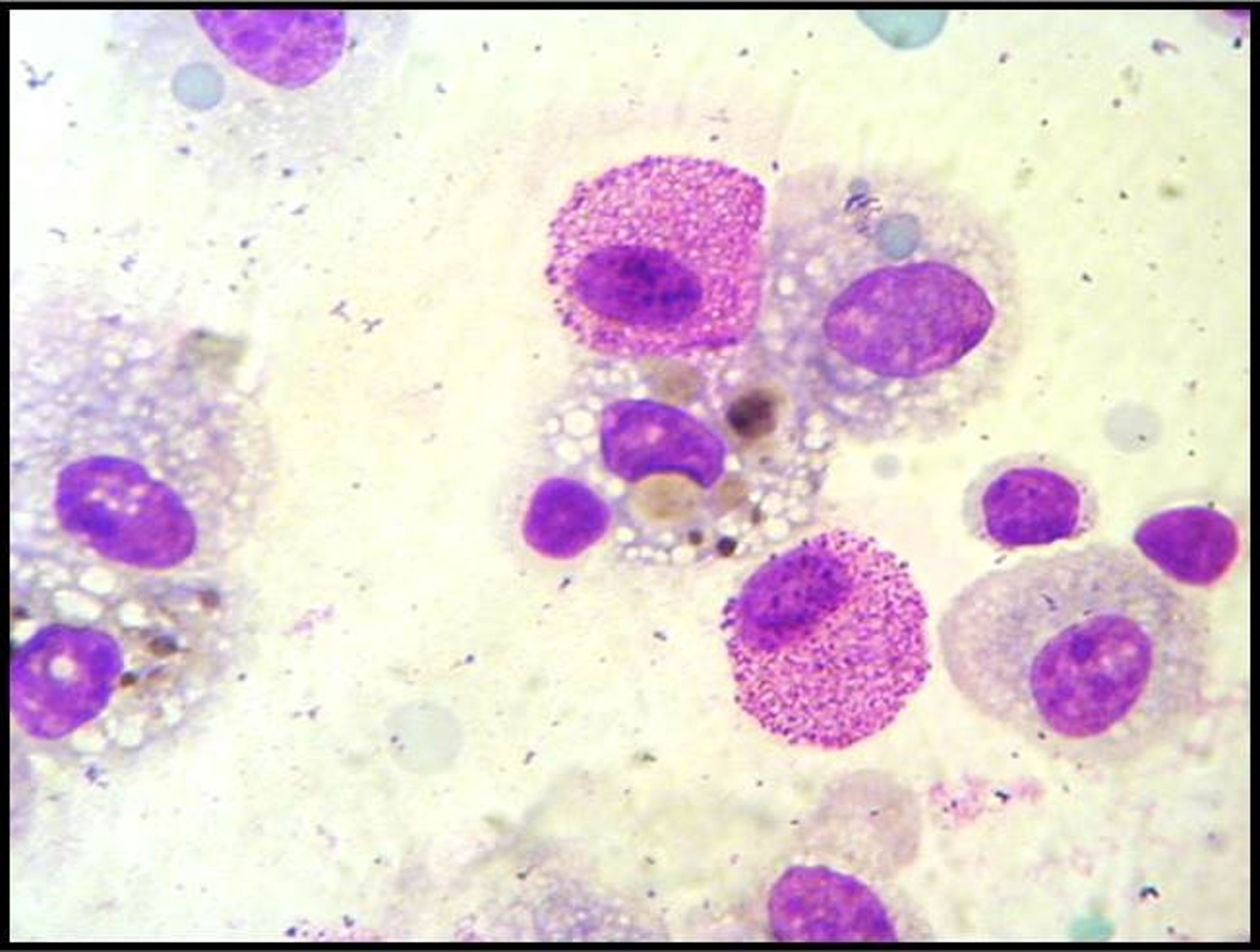
Courtesy of Dr. Melissa Mazan.

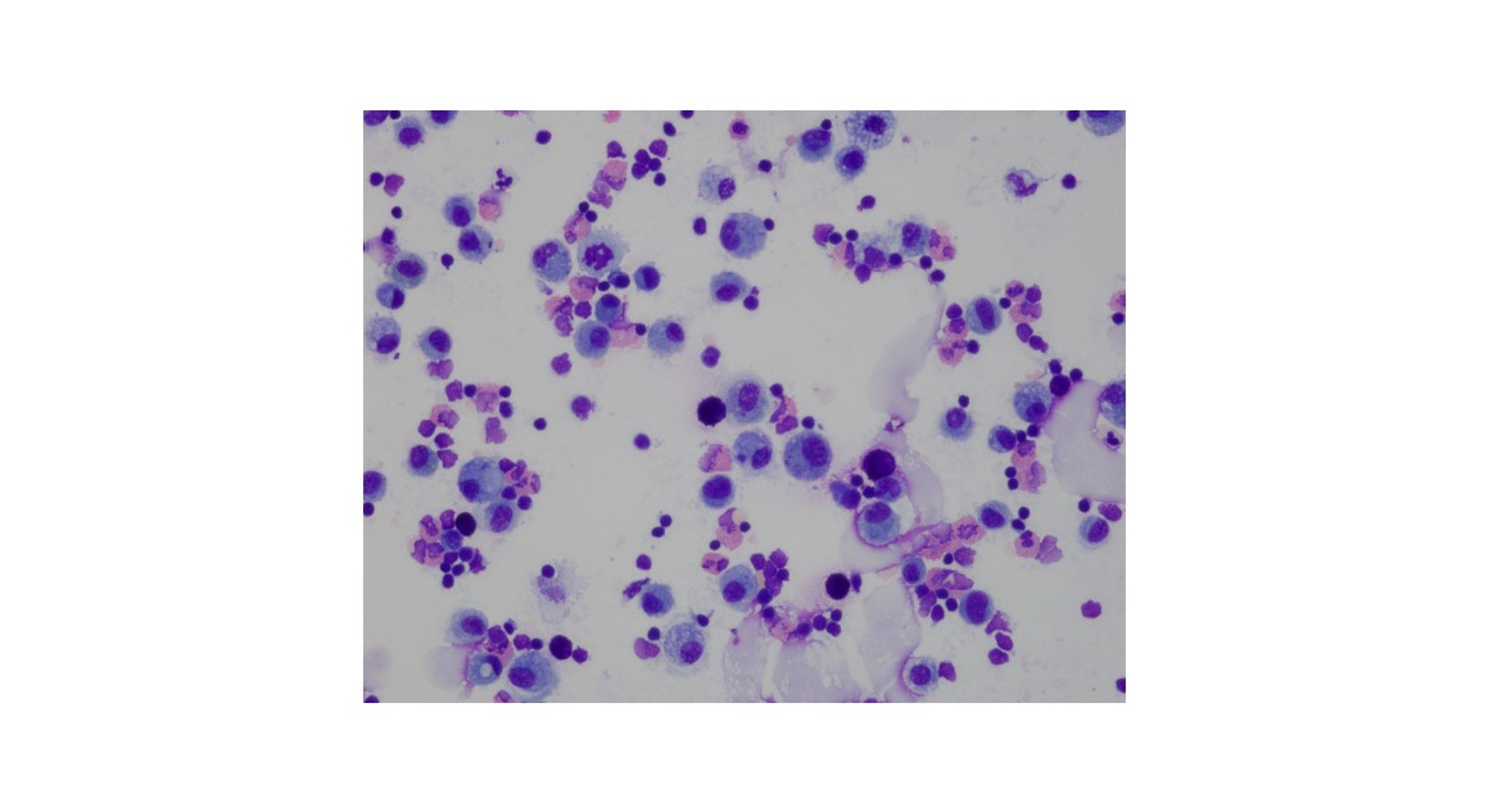
Courtesy of Dr. Emily Graff and Dr. Kara Lascola.

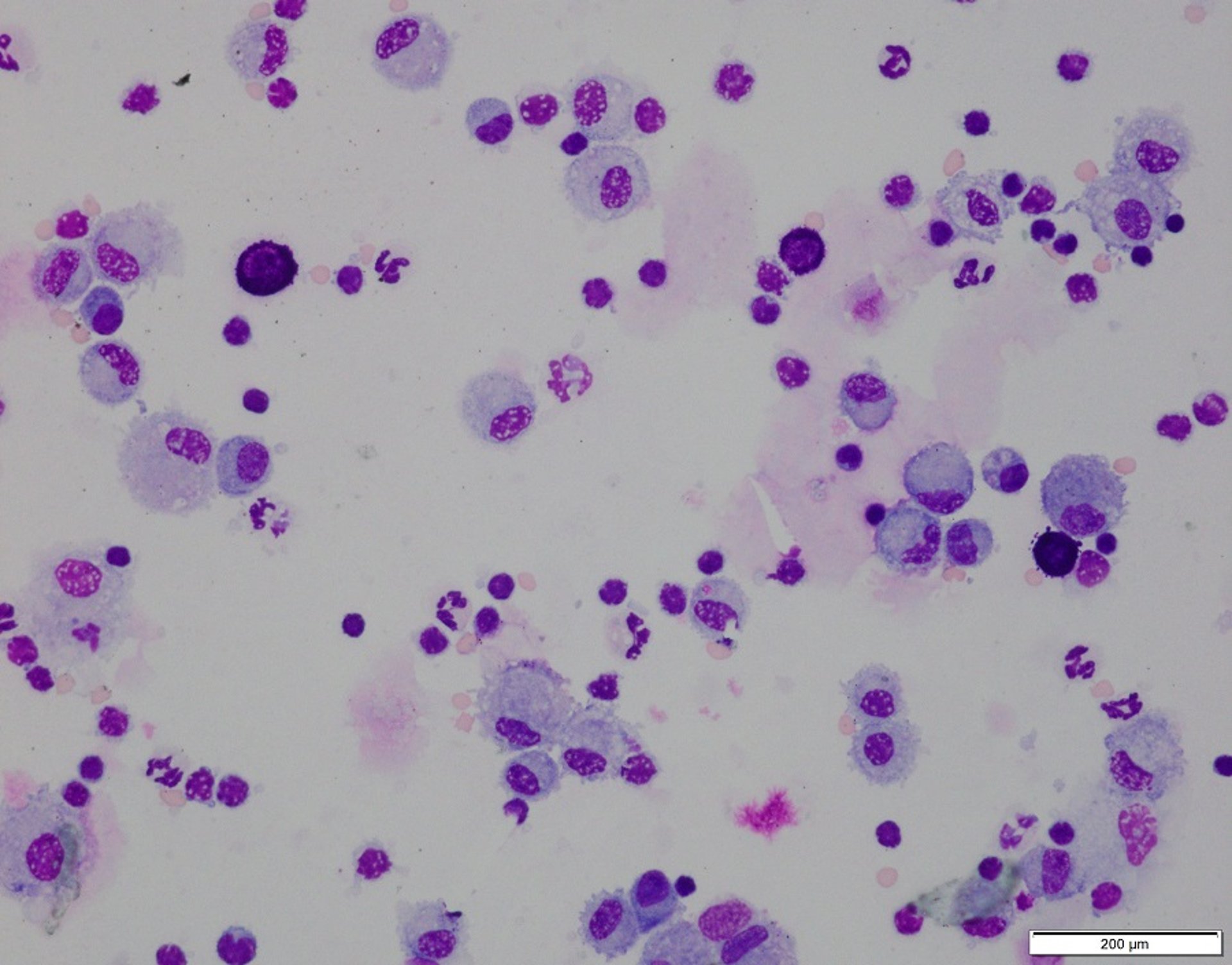
Courtesy of Dr. Emily Graff.
Endoscopic examination of the trachea and lower airways may reveal mucus accumulation, edema, and mucosal inflammation. Tracheal (grade 0–5) and bronchial (grade 0–3) mucus scoring systems are described for the diagnosis of equine asthma but are somewhat subjective. Additional tools described for the diagnosis and characterization of equine asthma include pulmonary function testing with bronchoprovocation to quantify lung dysfunction and airway hyperreactivity, and endobronchial ultrasound or biopsy to characterize airway inflammation and remodeling. These tools are currently limited to referral centers and often restricted to research settings.
Hematology and serum chemistry results are unremarkable. Although several have been evaluated (serum amyloid A, haptoglobin, surfactant proteins, etc), there are currently no reliable systemic biomarkers for the diagnosis of equine asthma. Thoracic radiographs typically reveal a diffuse bronchial and interstitial pattern and are of little benefit in confirming the diagnosis of equine asthma, but may help identify important differential diagnoses, including interstitial pneumonia, pulmonary fibrosis, or bacterial pneumonia.
Cytologic abnormalities in horses with severe and mild-moderate asthma
Cell Type | Normal | Severe Asthma | Mild-moderate Asthma |
|---|---|---|---|
Neutrophils | < 5% | 25%– 90% | > 10% – < 25%a |
Mast cells | < 2% | typically < 2% | > 5% |
Eosinophils | < 1% | typically < 1% | > 5% |
a Couetil LL, Cardwell JM, Gerber V, et al. Inflammatory airway disease of horses - revised consensus statement. JVIM. 2016;30:503-515. | |||
Treatment of Asthma in Horses
Environmental management
For severely-affected horses, asthma is a lifelong disease. The goals for treatment are to control episodes of disease exacerbation and to slow disease progression. For younger horses with mild-moderate asthma, treatment may not be as intensive, and for some of these horses, the disease may resolve spontaneously or with treatment. Goals for treatment and control of equine asthma, especially in severe cases, must include both long-term environmental management and medical strategies aimed at reducing the progression of airway inflammation and hyperreactivity as well as strategies aimed at improving the horse’s quality of life and/or athletic potential.
Environmental management is the single most important component of control of the disease, with the goal of minimizing the horse’s exposure to aerosolized allergens. In some horses, this alone can lead to resolution of clinical signs and improvement in lower airway inflammation. Medication will alleviate clinical signs of disease, but clinical signs will return after medication is discontinued if the horse remains in an allergen-rich environment.
Management changes should target common sources of allergen exposure. The most common culprits are organic dusts present in even good quality hay. If possible, horses should be maintained at pasture, with fresh grass as the source of roughage. (Round bale hay is particularly allergenic and is a common cause of treatment failure for horses on pasture).
Horses that remain stalled should be provided low-dust bedding and feed in a well-ventilated environment. Low-dust bedding options include shavings and cardboard. Immersing hay in water or steaming it before feeding can substantially reduce respirable dust, but doing so is often ineffective for highly sensitive horses. In these cases, hay cubes or pellets or haylage and complete pelleted feeds can be fed. Turnout during stall cleaning is helpful. Housing in the same building as an indoor arena or where hay is stored overhead should be avoided. Horses with summer pasture–associated obstructive pulmonary disease should be maintained in a dust-free, stable environment with turn-out limited to mowed pasture during the cooler times of day or evening.
Medical management relies on the judicious use of corticosteroid preparations (to reduce pulmonary inflammation) and bronchodilating medications (to provide relief of airway obstruction). Systemic and aerosolized formulations are available for many medications. Aerosolized treatment allows for direct delivery of the medication to the lower airways; several equine-adapted devices are available for use of inhalants.
Beta-2 adrenergic agonists (clenbuterol, albuterol) and muscarinic receptor antagonists (atropine, hyoscine butylbromide, ipratropium) are described for use as bronchodilators in horses and provide immediate relief of airway obstruction until clinical signs of disease are controlled by corticosteroids. It is inappropriate to treat equine asthma with bronchodilators as the sole treatment. Concurrent administration of beta-2 agonists with corticosteroids may potentiate anti-inflammatory effects of corticosteroids. Clenbuterol is the only beta-2 adrenergic agonist with FDA approval for use in horses. Drug tolerance has been associated with prolonged use of this medication.
Common Medications Used for Treatment of Equine Asthma
Drug Category | Drug and Dosage |
|---|---|
Bronchodilators | |
Beta-2 agonists | Clenbuterol: 0.8–3.2 mcg/kg, PO, q 12 h. FDA approved for equine chronic obstructive pulmonary disease. Tachyphylaxis is possible. Albuterol: 1–2 mcg/kg, inhaled via an equine-specific mask, q 1–3 h. Short duration of action. |
Muscarinic antagonists | Atropine: 0.02 mg/kg, IV. Short acting, potent bronchodilator. Tachycardia and gastrointestinal adverse effects are possible. Use only as an emergency rescue treatment. Butylscopolammonium bromide (hyoscine butylbromide): 0.3 mg/kg, IV. Very short (< 30 min) duration. Fewer adverse effects than atropine. FDA-approved for equine use as an intestinal antispasmodic. Ipratropium bromide: 0.18 – 0.3 mg per horse, inhaled via an equine-specific mask, q 4-8 h. Low systemic absorption allows for fewer adverse effects. |
Corticosteroids | |
Systemic | Dexamethasone: 0.04 mg/kg, IV or IM, every 24 h; 0.05 mg/kg, PO, q 24 h). For long-term treatment. Prednisolone: 1.1–2.2 mg/kg, PO, q 24 h. Taper to lowest effective dose. For long-term treatment. |
Inhaled | Fluticasone: (1–6 mcg/kg, inhaled via an equine-specific mask, q 12 h). Systemic absorption is possible. Beclomethasone: 1–8 mcg/kg, inhaled via an equine-specific mask, q 12 h. Systemic absorption is possible. Ciclesonide: 2744 mcg (8 actuations) per horse, inhaled via an equine-specific mask, q 12 h for 5 days, followed by 4116 mcg per horse (12 actuations), inhaled via an equine-specific mask, q 12 h for 5 more days. FDA-approved for severe equine asthma. |
Corticosteroids represent the most commonly administered medications for the control of airway inflammation. These may be delivered systemically (dexamethasone, prednisolone) or as inhaled formulations (fluticasone, beclomethasone, ciclesonide). Although described, nebulized dexamethasone does not appear to be effective in treating horses with severe asthma. Corticosteroids alone do not decrease airway neutrophilia but will improve hyperresponsiveness, airway remodeling, and clinical signs of asthma. Additional medications described for modulation of airway inflammation associated with mild-moderate asthma include low-dose interferon-alpha and sodium cromoglycate (a mast cell stabilizer). Dietary supplementation with polyunsaturated omega-3 fatty acids may be a helpful adjunct treatment in conjunction with environmental management. NSAIDs, antihistamines, mucolytic agents, and leukotriene-receptor antagonists have not demonstrated therapeutic benefit.
Key Points
Equine asthma is a common allergen–mediated chronic respiratory disease of adult horses, affecting two case populations: mild-moderate asthma in young, athletic horses and severe, progressive asthma in older horses.
Key features of equine asthma include airway inflammation, airway hyperresponsiveness, and airway remodeling, and all of these influence diagnostic and treatment strategies.
Findings on BAL cytology provide a definitive diagnosis of equine asthma and can be used to distinguish between mild-moderate and severe asthma.
Although medical treatment with bronchodilators and corticosteroids is important for horses with equine asthma, appropriate environmental management represents the cornerstone of treatment.
References
Couëtil, L.L., Ward MP. Analysis of risk factors for recurrent airway obstruction in North American horses: 1,444 cases (1990-1999). J Am Vet Med Assoc 2003;223:1645–50.
Wasko, A.J., Barkema, H.W., Nicol, J., Fernandez, N., Logie, N. and Léguillette, R., 2011. Evaluation of a risk‐screening questionnaire to detect equine lung inflammation: results of a large field study. Equine veterinary journal, 43(2), pp.145-152
Couetil LL, Cardwell JM, Leguillette, et al. Equine Asthma: current understanding and future directions. Front Vet Sci 2020 Jul 30;7:450. doi: 10.3389/fvets.2020.00450
Couetil LL, Cardwell JM, Gerber V, et al. Inflammatory airway disease of horses - revised concensus statement. JVIM. 2016;30:503-515.
Mahalingam-Dhingra A, Bedenice D, Mazan MR, Bronchoalveolar lavage hemosiderosis in lightly active or sedentary horses. JVIM. 2023. DOI: 10.1111/jvim.16692
For More Information
American Association of Equine Practitioners (AAEP): Managing summer pasture-associated obstructive pulmonary disease
Couëtil LL, Cardwell JM, Gerber V, et al. Inflammatory airway disease of horses – a revised consensus statement. J Vet Intern Med 2016; 30:503–515.
Equine asthma: current understanding and future directions. Front Vet Sci. 2020; 7:450 (pp 1–21.)
United States Equine Federation: 2022 Guidelines and Rules for Drugs and Medications
Also see pet health content regarding recurrent airway obstruction (heaves) and inflammatory airway disease in horses.





