




Strangles is a highly prevalent infectious disease characterized by upper respiratory tract lymph node abscessation secondary to infection with Streptococcus equi equi. The abbreviated terminology "Strep equi" is widely accepted to refer to this organism and is used here.
Strangles is a highly infectious disease of Equidae characterized by abscessation of the lymphoid tissue of the upper respiratory tract. It remains one of the most common infectious diseases of horses worldwide. The causative organism, Streptococcus equi equi, is highly host-adapted and produces clinical disease only in horses, donkeys, and mules. It is a gram-positive, capsulated beta-hemolytic Lancefield group C coccoid bacterium and, unlike Streptococcus equi zooepidemicus, is considered an obligate parasite and a primary pathogen in equids.
Strangles became a reportable disease in the US in 2017, although individual state guidelines on reporting vary. Diagnosis of strangles relies on culture of exudate from an abscessed lymph node or PCR array of guttural pouch or nasopharyngeal washes. Treatment of uncomplicated cases primarily relies on supportive care, with administration of antimicrobials recommended for complicated cases. Prevention and control measures are critical, especially during disease outbreaks.
Etiology and Pathogenesis of Strangles in Horses
S equi is highly infectious and produces high morbidity and low mortality in susceptible populations. Morbidity may reach 100% in naive horses. Disease is most severe in horses 1–5 years of age; however, it has been reported in foals as young as 3 months and in older adults. Transmission is via direct contact with infected horses or with any number of contaminated fomites. While horses with overt clinical signs of disease are obvious sources of infection, asymptomatic carriers (up to 40% of naturally infected horses) and horses recovering from infection but no longer demonstrating overt clinical signs play an important role in disease outbreaks and perpetuation of the organism within the population. Survival of the organism in the environment depends on temperature and humidity; wet, cold conditions and protection within mucoid secretions improve survival. S equi is susceptible to desiccation, extreme heat, and exposure to sunlight; most organisms do not survive > 3 days in the environment.
S equi bacteria gain entry to the upper respiratory tract via inhalation or ingestion and colonize regional lymph nodes within a few hours of infection. Bacterial replication and neutrophil influx contribute to the lymphadenopathy and lymph node abscessation that characterize clinical disease. Hematogenous and lymphatic spread of bacteria beyond the upper respiratory tract may also occur, resulting in abscess formation throughout the body (metastatic strangles). S equi bacteria are resistant to phagocytosis by neutrophils and possess several virulence factors that contribute to bacterial pathogenicity, including evasion of host defenses. One factor, the SeM protein, plays a central role in the virulence of S equi.
Clinical Findings of Strangles in Horses


Courtesy of Dr. Mariano Mora.

Courtesy of Dr. Sameeh M. Abutarbush.

Courtesy of Auburn University, College of Veterinary Medicine.
The incubation period of strangles is 3–14 days, and the first sign of infection is fever (103°–106°F [39.4°–41.1°C]). Horses begin shedding bacteria within 2–3 days of fever and will continue to shed for 2–3 weeks or longer. Within 24–48 hours of the initial fever spike, the horse will exhibit signs typical of strangles, including mucoid to mucopurulent nasal discharge, depression, and submandibular lymphadenopathy with or without abscessation. Horses with retropharyngeal lymph node involvement have difficulty swallowing, inspiratory respiratory noise, and extended head and neck. Rupture of retropharyngeal lymph node abscesses internally within the guttural pouch results in empyema and coincides with the presence of mucopurulent nasal discharge as exudate drains from the pouches. Uncleared exudate within the guttural pouches may result in chondroid formation, chronic inflammation, and development of a carrier state. Older animals with residual immunity may develop an atypical or catarrhal form of the disease with mucoid nasal discharge, cough, and mild fever.
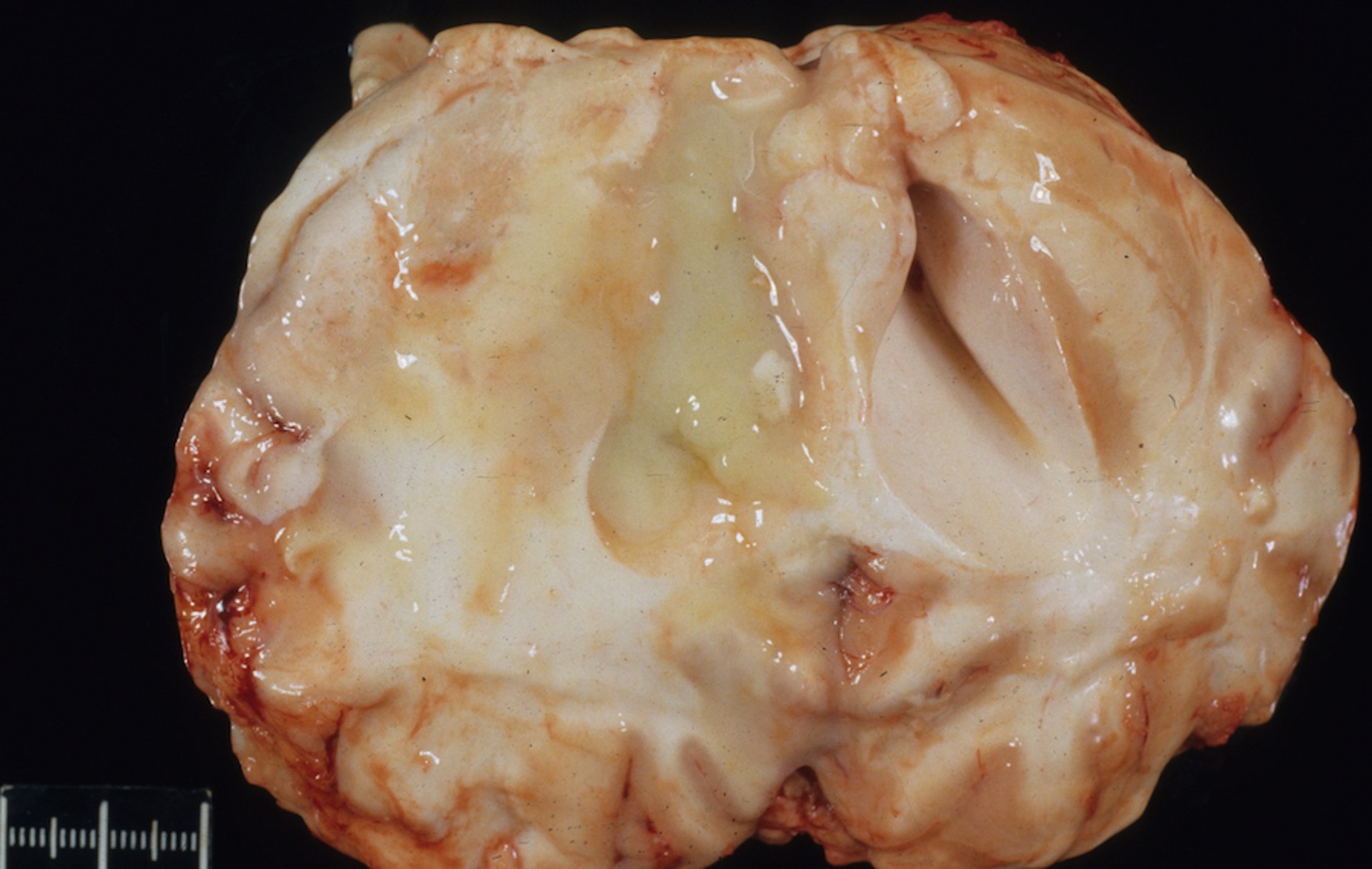
Potential complications associated with S equi infection include metastatic strangles ("bastard strangles") and the immunologic sequelae of purpura hemorrhagica and S equi-associated myositis. Metastatic strangles is characterized by abscessation in other lymph nodes of the body, particularly the lymph nodes in the abdomen and, less frequently, the thorax. S equi is the most common cause of brain abscess in horses, albeit rare.
Diagnosis of Strangles in Horses
Sample collection and diagnostic tests
Direct sampling from an abscessed lymph node is ideal but not always possible and does not allow for sampling of carriers or early in the course of disease. Other sampling techniques include a nasopharyngeal swab or wash or a guttural pouch wash. Of these, swabs are the least sensitive. A nasopharyngeal wash is relatively easy to collect and provides greater sensitivity than a swab. A guttural pouch wash is the most technical and time consuming; however, it provides the greatest sensitivity and is preferred for detecting carrier animals.
Culture has been considered the gold standard for confirming a diagnosis of strangles, and remains the preferred method for detecting S equi on aspirates or exudate from abscesses or in animals with obvious clinical signs of disease. False negative results are possible in early disease or with carriers because of intermittent shedding or shedding of bacteria in low numbers. PCR testing is more sensitive than culture and is preferred, particularly on a guttural pouch wash, to detect carriers. Serologic testing to detect SeM-specific antibody titers or surface antigens is rarely used alone, but it may be useful to detect previous or recent infection, strangles-associated complications, or to guide decisions on vaccination.
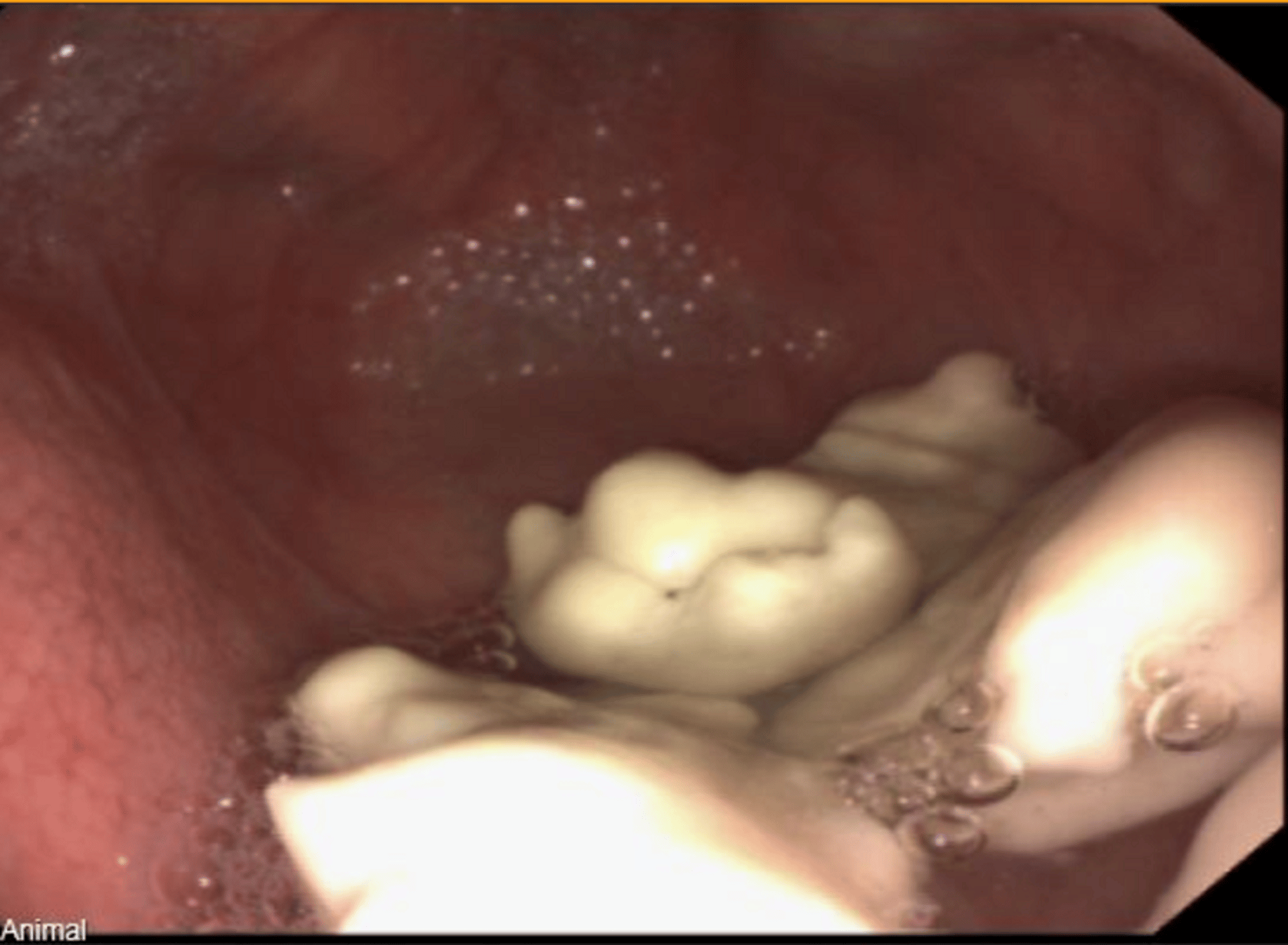
Hematologic analysis is generally nonspecific or unremarkable, although CBC often reveals neutrophilic leukocytosis and hyperfibrinogenemia. Endoscopic examination of the upper respiratory tract is useful and should include evaluation of the guttural pouches for empyema or chondroids (inspissated pus). In complicated cases or cases of metastatic strangles, ultrasonographic or radiographic examination may be helpful to identify the location and extent of abscesses.
Treatment of Strangles in Horses
Antimicrobials, sometimes
Supportive treatment
Treatment for horses infected with S equi depends on disease severity and stage of disease and will vary in cases of metastatic strangles depending on disease manifestation.
Antimicrobial treatment is controversial. Administration during the early stage of infection (≤ 24 hours of onset of fever) may arrest abscess formation and shedding. The disadvantage of early antimicrobial treatment is failure to mount a protective immune response, rendering horses susceptible to infection after cessation of treatment. Antimicrobial administration is not recommended during uncomplicated strangles after abscess formation as it may prolong maturation of abscesses (and thus the course of disease) and can also interfere with the development and persistence of humoral immunity.


Courtesy of Auburn University College of Veterinary Medicine.


Courtesy of Dr. Bonnie R. Rush.
Antimicrobial treatment is indicated in cases with dyspnea, dysphagia, prolonged high fever, and severe lethargy or anorexia, and also in complicated manifestations of the disease (eg, metastatic strangles, purpura hemorrhagica, myositis). If antimicrobial treatment is indicated, procaine penicillin (22,000 IU/kg, IM, q 12 h) is the antimicrobial of choice. Cephalosporins and macrolides are additional antimicrobial options. Untreated guttural pouch infections can result in persistent guttural pouch empyema with or without chondroid formation. Repeated guttural pouch lavage, endoscopic or surgical removal of chondroids, or local administration with antimicrobial gels may be required for resolution of infection in these cases.
Supportive treatment should include provision of a warm, dry, and dust-free environment with palatable feed, warm compresses applied to sites of lymphadenopathy to facilitate maturation of abscesses, and judicious administration of NSAIDs to decrease pain and fever and to improve appetite. Facilitated drainage of mature abscesses will speed recovery. Ruptured abscesses should be flushed with dilute (3%–5%) povidone-iodine solution for several days until discharge ceases. In severe cases, intensive care such as tracheostomy, intravenous fluids, and feeding via an indwelling nasogastric tube may be required.
Prevention of Strangles in Horses
Post-exposure immunity is prolonged after natural disease in most horses not treated with antimicrobials during primary infection. Protection is associated with local (nasal) mucosal production of antibody against the antiphagocytic M protein, and most likely also involves a systemic immune response. Both extract and attenuated live vaccines are available for administration to healthy animals. Vaccination is discouraged during an outbreak and especially in horses that have been in direct contact with horses with strangles. The clinical attack rate of strangles is reduced by 50% in horses vaccinated with intramuscular products and several cell free extract vaccines are available. An intranasal vaccine containing a live attenuated strain of S equi equi was designed to elicit a mucosal immunologic response. Reported complications with the intranasal product include vaccine-associated clinical disease, abscesses at subsequent intramuscular injection sites (due to live bacteria on hands of administrator, after using intranasal vaccine), submandibular lymphadenopathy, serous nasal discharge, and purpura hemorrhagica. ( See also page Other Type III Reactions).
Control of Strangles in Horses
Strangles is a reportable disease and practitioners should be aware of individual state guidelines for reporting. Prevention of strangles relies on isolation of new arrivals to the property for 14–21 days, restricted contact or isolation of resident horses who have been exposed during travel to shows, and quarantine of the premises during an outbreak. Additional screening of new arrivals for subclinical carrier status should also be considered and animals should be monitored for evidence of disease. During an outbreak, horses should be physically separated into groups according to infection status (clinically affected, exposed, clean). Strict biosecurity should be employed and if possible each group cared for by separate caretakers wearing protective clothing. Monitoring, including twice daily rectal temperature of all horses, should be employed to detect new cases of disease. Contaminated equipment should be cleaned with detergent and disinfected using chlorhexidine gluconate or glutaraldehyde. Flies can transmit infection mechanically; therefore, efforts should be made to control the fly population during an outbreak. Farriers, trainers, and veterinarians should wear protective clothing or change clothes before traveling to the next equine facility.
Recovering horses can continue to shed S equi for ~4–6 weeks after recovery. Screening for shedding or carrier status should not be initiated until 3 weeks after resolution of clinical signs of disease. A PCR array of a single bilateral guttural pouch wash (ideally with endoscopy) is the most sensitive means to detect continued infection; however, 3 negative nasopharyngeal washes at intervals of 7 days can also be used for release from quarantine if this is not possible. Prolonged bacterial shedding (up to 18 months) has been identified in a small number of horses. Guttural pouch empyema is the source of infection in most prolonged carrier states and warrants appropriate treatment and retesting when detected.
Key Points
Strangles is caused by the gram positive bacteria Streptococcus equi equi and is a highly contagious and reportable disease.
The most common clinical manifestation of strangles is lymphadenopathy and abscessation of the upper respiratory tract lymph nodes. Unless disease is complicated, treatment is primarily supportive.
Diagnosis relies on culture or PCR of abscess material or washes from guttural pouch or nasopharynx.
Nasal and intramuscular vaccines are available but may be associated with complications, including vaccine-associated disease.
Biosecurity and appropriate screening for carriers are essential for control and prevention of outbreaks.
For More Information
Boyle AG, et al. ACVIM Consensus Statement. Streptococcus equi infections in horses: guidelines for treatment, control, and prevention of strangles–revised consensus statement. J Vet Intern Med 2018; 32:633–647.
AAEP: Infectious disease guidelines: Strangles
Also see pet health content regarding strangles in horses.







