



Also text Bloodborne Organisms in Poultry.
Parasitic disease has become less common in captive parrots throughout the past 20 years with the restrictions against importation of wild-caught birds; many pet birds now are incubator hatched and hand raised and have little to no access to the outdoors or to other birds. Commonly reported parasitic diseases include protozoal infections such as giardiasis in cockatiels, sarcocystis in larger parrots, and mites in budgerigars and passerines.
Parasites of the Circulatory System
Also text Bloodborne Organisms in Poultry.
Protozoal Parasites of the Circulatory System of Pet Birds

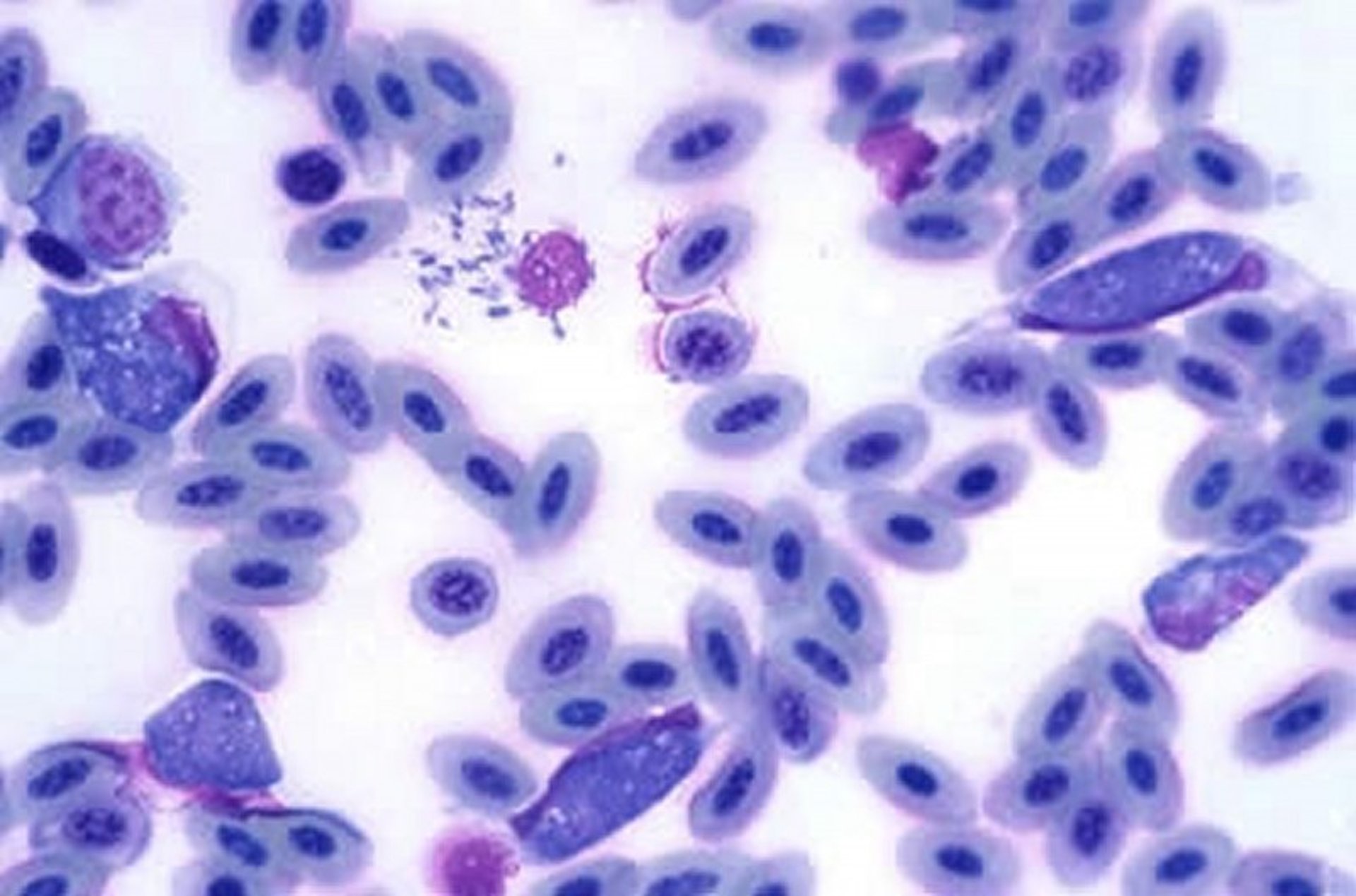
Leukocytozoon in an avian blood smear, 400X. Several of the large basophilic organisms are seen distending the avian WBCs (note flattened or malformed nucleus of host cell). A ruptured granulocyte is also present in the center of the field (artifact).
Courtesy of Dr. Louise Bauck.
Haemoproteus was previously documented with great frequency in imported Cacatua spp. Leucocytozoon, Plasmodium, and Atoxoplasma spp are all seen occasionally in various species, most commonly in raptors, canaries, and Columbiformes, and are currently not of major significance in psittacines. Atoxoplasmosis is still diagnosed in canaries.
Parasites of the Gastrointestinal System
Giardiasis of the Gastrointestinal System of Pet Birds

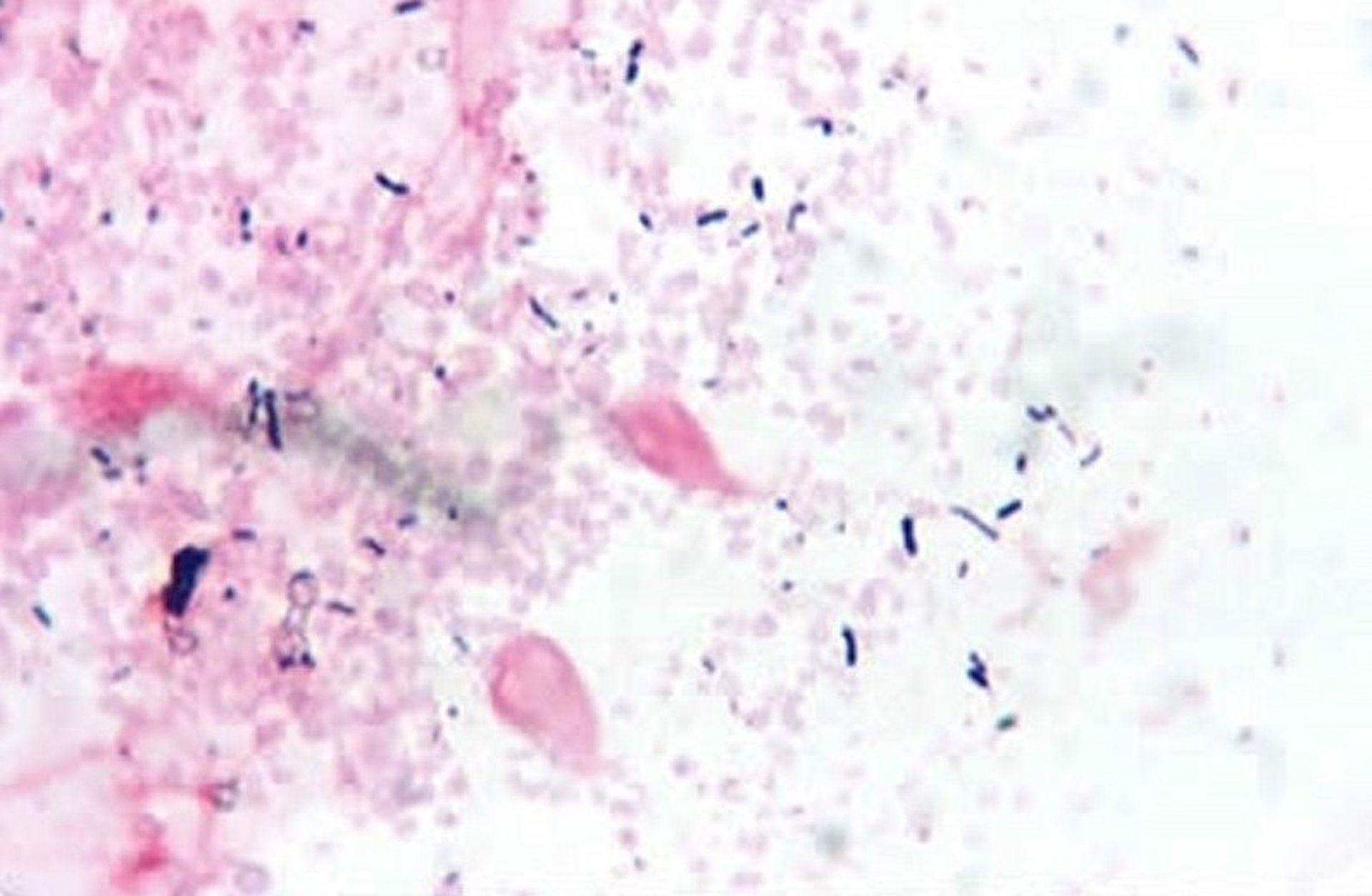
Giardia psittaci, 100X. Two pear-shaped organisms are visible in this Gram stain of an impression smear from the small intestine of a parakeet.
Courtesy of Dr. Louise Bauck.
Giardiasis has been reported in many species of birds but is most commonly seen in cockatiels. Adult birds may be latent carriers. Transmission is presumably direct (ingestion of infective cysts). Affected cockatiels occasionally exhibit feather pulling in the axillary and inner thigh regions, along with vocalization. A true causal relationship between giardiasis and these clinical signs has not been proved. Droppings of affected cockatiels may be voluminous and aerated (a “popcorn” appearance).
Diagnosis
There are several ways to diagnose Giardia spp infection:
zinc sulfate flotation test of feces to detect cysts
direct saline smear of fresh feces to detect motile trophozoites
ELISA test for Giardia spp antigen in feces
PCR assay
Because the presence of cysts is variable, serial tests may be needed.
Treatment
Metronidazole (25–50 mg/kg, PO, every 12–24 hours for 5–7 days)
Carnidazole (20–30 mg/kg/day, PO, for 1–2 days)
Trichomoniasis of Pet Birds
Trichomoniasis has been reported in many orders of birds, including Columbiformes, Galliformes, Falconiformes, Psittaciformes, and Passeriformes. Trichomonas gallinae (termed "frounce" in birds of prey and "canker" in Columbiformes) is occasionally seen in pet birds, notably budgerigars. Clinical signs may include anorexia, dysphagia, weight loss, and dyspnea. Whitish yellow, caseous lesions adherent to the mucosa of the oropharynx, crop, and esophagus may be seen in raptors and Columbiformes. Budgerigars generally do not have grossly visible oral lesions but do have increased salivation and regurgitation. Transmission is by direct (parents feeding young) or indirect (ingestion of contaminated food and water) contact; raptors may become infected by ingesting infected pigeons or doves.
Microscopic examination of a warm saline mount of material from the oral cavity may reveal the flagellated organism. Treatment protocols include carnidazole (20–30 mg/kg, PO, for 1–2 days), ronidazole (6–10 mg/kg/day, PO, for 7–14 days), or metronidazole (25–50 mg/kg, PO, every 12–24 hours for 5 days).
Other Protozoal Diseases of Pet Birds
Cryptosporidiosis has been seen in a variety of avian species but is thought to be a secondary rather than a primary pathogen.
Plasmodium spp infection (malaria) is highly pathogenic in gyrfalcons, canaries, and penguins. Plasmodium is spread by mosquitoes.
Atoxoplasmosis is a highly pathogenic protozoal disease that causes hepatomegaly and splenomegaly in canaries, with coccidia-like oocysts shed in the feces.
Other protozoan parasites such as coccidia are much more common in gallinaceous or Columbiforme birds, although coccidial oocysts are seen occasionally in psittacine and passerine birds.
Roundworms of Pet Birds
Various genera and species of roundworms infect pet birds, and wild birds may transmit nematodes to captive parrots housed outdoors. Transmission is direct by ingestion of embryonated ova. Clinical findings include loss of condition, weakness, emaciation, and death; intestinal obstruction is common in heavy infections. Diagnosis of intestinal nematode infection is by fecal flotation, although shedding of ova may be intermittent. Ivermectin (0.2 mg/kg, PO, SC, or IM, repeated in 10–14 days), pyrantel pamoate (4.5 mg/kg, PO, repeated in 10–14 days), or fenbendazole (20–50 mg/kg, PO, repeated in 14 days) are generally effective. In warm climates where exposure via outdoor aviaries is likely, routine deworming (every 6 months) with one of these anthelmintics is often practiced.
Cestodes of Pet Birds
Cestodes are uncommon in domestically bred birds. The most common pet birds infected with tapeworms are cockatoos, African grey parrots, and finches. Intermediate hosts are most likely insects and arachnids of various types, earthworms, and slugs. Infected birds are asymptomatic or are unthrifty, with or without diarrhea. Diagnosis is based on visualization of eggs on a fecal flotation.
Praziquantel (5–10 mg/kg, PO or IM, once) is the recommended treatment. Recurrence is rare in cases in which the intermediate host is not indigenous to the area where the bird is housed.
Parasites of the Integumentary System
Scaly Face (Leg) Mite of Pet Birds


Mange (Knemidocoptes) on the beak and face of a parakeet. Pale, crusty lesions are present, and the beak is malformed due to the presence of mites.
Courtesy of Dr. Louise Bauck.
Scaly face, or Knemidocoptes pilae (also Cnemidocoptes pilae), is common in budgerigars and rare in all other psittacine species. In budgerigars, white, porous, proliferative encrustations involving the corners of the mouth, cere, beak, and occasionally the periorbital area, legs, or vent are typical. In passerine birds (particularly canaries and European goldfinches), crusts form on the legs and surfaces of the digits (“tassel foot”). The mites can be recovered from facial scrapings of budgerigars, although the clinical appearance is generally pathognomonic. In passerines affected with Knemidocoptes, skin scrapings of the legs often result in hemorrhage and are generally not recommended. Ivermectin (0.2 mg/kg, PO or IM) or moxidectin (0.2 mg/kg, PO or topically) is generally effective. The treatment is repeated in 2 weeks.
Feather Mites of Pet Birds
Psittacine birds are seldom affected by feather mites. Occasionally, infestation with the red mite (Dermanyssus gallinae) may be found in outdoor aviaries, especially in nest boxes. A causative relationship between mites and feather picking is often assumed by owners of feather-picking birds, although this is rarely the case. More commonly, behavioral, husbandry, and/or systemic factors are linked to feather loss.
Mite-infested birds may be treated with pyrethrin sprays, 5% carbaryl powder, or ivermectin (0.2 mg/kg, PO or IM) repeated in 2 weeks. Nest box treatment includes mixing 5% carbaryl powder into the nest box substrate. Cages should be cleaned thoroughly, and wooden nest boxes should be discarded and replaced.
Parasites of the Respiratory System
Air Sac Mites of the Respiratory System in Pet Birds
Sternostoma tracheacolum parasitizes the entire respiratory tract, most frequently of canaries and gouldian finches. The mites are found in the trachea, syrinx, lungs, and air sacs. All stages of the mite are found within the respiratory tissues. The life cycle is poorly understood.
In mild infections, birds are usually asymptomatic; in heavy infections, audible dyspnea (high-pitched noises and clicking), sneezing, tail bobbing, and open-mouthed breathing are noted. Copious amounts of saliva are seen in the oropharynx, and ptyalism may be present. Signs are exacerbated by handling, exercise, and other stresses. Mortality can be high. Transillumination of the trachea in a darkened room occasionally reveals the mite. Response to treatment can help reach a diagnosis.
Treatment should be administered quickly and with minimal handling. Ivermectin (0.2–0.4 mg/kg, PO or IM) repeated in 2 weeks or moxidectin (0.2 mg/kg, PO or topically) repeated in 2 weeks may be administered.
Sarcocystosis of the Respiratory System of Pet Birds
Sarcocystosis is a major cause of mortality in parrots housed outdoors in the southern US. It is not a contagious disease but may occur in clusters because of the life cycle of the protozoan parasite. Protozoal oocysts are passed from infected opossum feces by insects or rodents into the enclosure of the birds. The feces of these transport hosts are then consumed by the birds, and a rapidly fatal disease can develop. Old World birds are most susceptible and may die acutely. Clinical signs include depression, respiratory distress, weakness, ataxia, and anemia. Antemortem diagnosis and treatment can be challenging.
In severely affected areas, even indoor birds can be infected via contaminated food. The oocysts of this protozoan parasite are passed from infected opossum feces by insects (eg, flies, cockroaches) or mice and rats into the feed cups or enclosure of the birds. The feces of these transport hosts are then consumed by the birds, and a rapidly fatal disease can develop. Old World species are immunologically naive to this disease, and a high mortality rate is observed in untreated birds such as cockatoos, African grey parrots, and Eclectus parrots. Cockatiels are also susceptible, and renal as well as pneumonic lesions are often noted at necropsy in this species. Although not contagious, cases tend to occur in clusters because the infected opossum feces are spread via insects around the aviary grounds. Large die-offs have been documented.
Clinical signs of sarcocystosis in birds may include lethargy, passive regurgitation of water, respiratory distress, weakness, ataxia, and anemia. In Old World parrots (eg, cockatoos, African grey parrots), disease occurs in the early stages of infection as the parasite is undergoing schizogony or merogony (asexual reproduction) in the lung. This causes lung damage, and the birds die acutely with or without signs of respiratory distress. In New World parrots (eg, macaws, conures), the organism encysts in the muscle or CNS, causing weakness, ataxia, or neurologic signs. The disease can manifest as an asymptomatic or clinically apparent muscular disease, cardiac disease, acute pulmonary disease, or encephalitis. Encephalitis (paresis, intention tremors, and head tilt) has been seen in psittacines and raptors.
No specific diagnostic test is available, although results of plasma protein electrophoresis may indicate infection (marked increase in beta-globulin concentrations with or without a marked increase in gamma globulin concentrations). An indirect immunofluorescence antibody (IFA) test has been developed that may aid in antemortem diagnosis of the nonperacute form of sarcocystosis in psittacine birds. The sensitivity and specificity of the IFA test ranges from 83%–86%. PCR assay is also available. Results of muscle biopsy may be conclusive for the encysted stages but is not commonly performed. When a muscle biopsy is done, the quadriceps muscle has been reported to be a better site than the pectoral muscle. Increases in enzyme activities of LDH, AST, and CK have been reported.
Gross necropsy findings include increased lung density, hemorrhage, and renal lesions. Histopathologic samples should include lung, kidney, muscle, and CNS tissue if neurologic signs are apparent.
Protracted treatment of sarcocystosis with trimethoprim/sulfamethoxazole (30 mg/kg, 2 times a day) and pyrimethamine (0.5 mg/kg, PO, 2 times a day) has had limited success in birds. Response to treatment is generally monitored by serial PCV sampling. Newer drugs used to treat infection by the related protozoa, Sarcocystis neurona, that affects horses have not yet been evaluated for treatment in birds.
For More Information
Also see pet health content regarding disorders and diseases of pet birds.





