




Avian Polyomavirus
Avian polyomavirus (APV) causes disease in young parrots. There are two forms of the disease based on affected species: budgerigar fledgling disease and non-budgerigar polyoma infection. Both are characterized by peracute to acute death of preweaned neonates. Clinical signs occur 7–10 days after exposure and include lethargy, crop stasis, and death within 24–48 hours. Surviving budgerigars >3 weeks old often exhibit feather dystrophy (French molt or feather dusters). Older nonbudgerigar psittacines may have subclinical disease or hemorrhages and coagulopathies. Adult birds typically are resistant to infection; they will seroconvert and shed the virus for up to 90 days, then clear the infection. Antemortem diagnosis is accomplished with DNA probes of cloacal swab and blood samples. Aviary control methods include not housing budgerigars or lovebirds with other species, strict hygiene, limiting traffic in the nursery, and strict quarantine and testing of new birds. A vaccination is available.
Clinical Findings of Avian Polyomavirus
The typical presentation of budgerigar fledging disease is a well-fleshed juvenile, just before fledgling age, with acute onset of lethargy, crop stasis, and death within 24–48 hours. Other clinical signs are cutaneous hemorrhage, abdominal distention, and feather abnormalities. Surviving budgerigars >3 weeks old often exhibit feather dystrophy (French molt or feather dusters). In other species of psittacines < 4 months old, the infection is often fatal. Older nonbudgerigar psittacines may have subclinical disease or hemorrhages and coagulopathies.
Diagnosis of Avian Polyomavirus
Antemortem diagnosis is accomplished with DNA probes of cloacal swab and blood samples and virus-neutralizing antibody tests of blood samples to identify birds with previous viral exposure. Diagnosis in a flock setting is typically based on clinical signs, signalment, and necropsy findings.
Gross necropsy findings in deceased chicks often include pale skeletal musculature and subcutaneous ecchymotic hemorrhages. The kidneys and liver are enlarged and may be pale, congested, and mottled, or have pinpoint, white foci. Petechial or ecchymotic hemorrhages may also be present on viscera, particularly the heart. The heart is sometimes enlarged and may show hydropericardium. Intranuclear inclusion bodies are often seen in the liver, kidneys, heart, spleen, bone marrow, uropygial gland, skin, feather follicles, etc.
Treatment and Control of Avian Polyomavirus
Aviary control methods include avoiding the housing of budgerigars or lovebirds on premises where other species are bred, adhering to standard hygiene procedures, preventing access to the nursery by visitors, and not introducing birds into the aviary without 90 days quarantine and testing. Eliminating APV infection from an infected budgerigar aviary is challenging. First, all breeding must be stopped for 6 months. The presence of infected neonates, fledglings, and adults propagates the disease. During this time, adult birds are moved to a noninfected area while the entire aviary is disinfected. Nest boxes should be disinfected or discarded and replaced. After 6 months, adult breeding birds can be returned to a clean aviary and breeding resumed.
Pet store prevention should include separating neonates from different sources, purchasing birds from sources where polyomavirus testing and vaccination are performed, and ideally, not purchasing or selling unweaned birds.
Treatment is supportive care. A vaccine is available. For breeding birds, two doses of the vaccine are administered at a 2-week interval; this should be done off-season. The manufacturer recommends administration of the first dose when the chick is >35 days old, with a booster vaccination in 2–3 weeks.
Psittacine Beak and Feather Disease
Psittacine beak and feather disease (PBFD) is caused by a psittacine circovirus. The virus was first recognized in the 1970s in cockatoos with beak and feather lesions. Since then, it has been recognized in most species of parrots and also in Passeriformes and Columbiformes. It primarily affects young parrots. Infected birds present with abnormal feathers, beak lesions, and immunosuppression. Infected birds shed virus in their feathers, feather dander, feces, and oral secretions. Transmission occurs by inhalation and/or ingestion of the virus and can occur vertically. The virus is very stable in the environment, so fomites are a notable source of infection. Diagnosis is based on clinical signs and results of PCR testing. Treatment is supportive care. Due to its contagious nature and terminal outcome, humane euthanasia may be warranted. Control involves strict hygiene, testing, and quarantine of all new birds.
The name is not as representative of the current typical clinical presentation, which often does not include beak abnormalities and is less likely to have the severe, classic feather abnormalities seen in cockatoos when the disease was first documented. Use of screening PCR assays has greatly decreased the prevalence of the virus in captive bred Cacatua spp. However, disease is still seen in African grey parrots, Eclectus parrots, lovebirds (Agapornis), lorikeets, and other species, but is rare. The natural infection appears to occur primarily in juvenile birds, with few instances of clinical infection seen in birds >3 years old.


Courtesy of Dr. Louise Bauck.
Clinical Findings of Psittacine Beak and Feather Disease
In the classic PBFD infection, the first indication of the presence of disease is a lack of powder down on the beak. The virus causes abnormal formation of growing feathers and immunosuppression. Feathers are pinched or clubbed at their base and may have hemorrhage within the developing shaft. The feathers fall out easily and grow back slowly or not at all. The distribution of affected feathers depends on the age of the bird and the stage of the molt when infected. Pigment loss may occur in colored feathers. The bird may live with these lesions for months to years.
As the disease progresses, the immune system is affected, and most birds die of secondary infections. A peracute form of the disease occurs in young birds, which develop enteritis and pneumonia, lose weight, and die. African grey parrots may develop a pancytopenia, because the virus attacks the bone marrow. These birds die suddenly with viral inclusions in the thymus, bursa, and bone marrow.
Diagnosis of Psittacine Beak and Feather Disease
Diagnosis of psittacine beak and feather disease is based on clinical appearance; results of PCR assay of feces, feather dander, or blood; and biopsy of affected feather follicles showing basophilic intracytoplasmic inclusions. Testing by PCR assay may detect infection in birds that still appear healthy. These birds may subsequently become ill or may mount an effective response to the virus. Because of the stability of the virus, PCR analysis can also be used for environmental testing. Quarantine and retesting are recommended for PCR-positive, asymptomatic birds. At necropsy, affected birds often have no gross lesions internally, but intranuclear or intracytoplasmic inclusions may be seen histologically in the feathers, bursa, thymus, liver, or other organs.
Treatment and Control of Psittacine Beak and Feather Disease
There is no specific treatment for PBFD, and treatment of infected birds is supportive. The contagious nature of PBFD and its generally terminal outcome in clinically affected birds warrant isolation and eventual euthanasia in most clinical cases. Strict hygiene with attention to dust control, screening protocols including PCR testing of both birds and the environment, and lengthy quarantines are highly recommended in breeding facilities with susceptible species. All new susceptible birds should be tested before introduction to the aviary. In infected breeding colonies, removing all eggs for cleaning and artificial incubation may also be required. Since the development of a PCR assay, prevalence of the disease has decreased.
Pacheco’s Disease
Psittacine herpesvirus is an alpha herpesvirus that is the causative agent of Pacheco’s disease and internal papillomatosis in parrots. Pacheco’s disease causes a viral hepatitis seen predominantly in New World species (Amazon parrots, macaws, and conures).
Internal papillomatosis occurs in parrots that have survived Pacheco’s disease. Papillomatosis is most commonly observed in macaws, Amazon parrots, conures, and Hawk-headed parrots. Disease is associated with stress, which can cause clinically healthy carriers to shed virus and initiate infection in susceptible birds, as often occurs during introduction of new birds, relocation, or in those with underlying illness or during breeding. It is spread by direct contact, aerosol, or fecal contamination of food or water, with an incubation period of 3–14 days. The outcome of the infection depends on the genotype of the virus, the species of bird infected, and the bird's overall health. Infected birds become chronic carriers and will remain persistently infected and intermittently shed the virus throughout their lives. Old World species are less likely to be either inapparent carriers or clinically susceptible. Patagonian species and some Aratinga spp may be natural hosts in the wild, and some individuals of these species may asymptomatically shed virus when stressed. Other species can also act as carriers.
Clinical Findings of Pacheco's Disease of Pet Birds
Terminal signs of Pacheco's disease include acute death in well-fleshed birds and bright yellow urates with scant feces. Other clinical signs are diarrhea, green urates, lethargy, regurgitation, weakness, and depression.
Diagnosis of Pacheco's Disease of Pet Birds
Diagnosis of Pacheco's disease in a live bird can be done by DNA probes of combined oral and cloacal swabs and blood samples. Increases in plasma AST activity and marked leukopenia have been reported.
Because of the acute nature of the disease, histologic lesions may not be evident. However, most affected birds will have hepatomegaly, splenomegaly, and renomegaly. The liver may be mottled or grossly discolored. Ecchymotic and petechial hemorrhages may be present on the pericardium and within the mesenteric fat. Intranuclear inclusions are seen histologically in the liver, spleen, intestinal epithelium, and pancreas.
Treatment and Prevention of Pacheco's Disease of Pet Birds
In addition to supportive care, acyclovir (80 mg/kg, 3 times a day, or 400 mg/kg in feed) can be used during an outbreak; however, the risk of increased transmission because of handling is great. Autogenous vaccines have been developed during outbreaks and have effectively decreased morbidity and mortality. An inactivated vaccine is available.


Courtesy of Dr. Louise Bauck.
The lesions of papillomatosis are predominantly present in the oral and cloacal mucosa but may also be found internally in the intestinal tract, or less commonly, in the conjunctiva or bursa. Owners usually first notice blood from a papilloma in the droppings, and/or the papilloma prolapses through the cloaca. Lesions may be mild or severe (ulcerated and bleeding) and often wax and wane. Ulcerated lesions may need to be cauterized or surgically removed, although they typically recur. Treatment is supportive, such as analgesics, cautery, and antimicrobials to prevent secondary infection. Antiherpesviral drugs are not curative and do not appear to impact the course of disease.
Avian Bornavirus / Proventricular Dilatation Disease

Courtesy of Dr. Sharman Hoppes.
Avian bornavirus (ABV) is a neurotropic virus that causes proventricular dilatation disease (PDD). PDD is a progressive neurologic disease that uniquely affects the nervous system and is fatal once clinical signs develop. PDD, also known as macaw wasting disease, neuropathic ganglioneuritis, lymphoplasmacytic ganglioneuritis, psittacine encephalomyelitis, and avian ganglioneuritis, was first recognized in the late 1970s in macaws imported into the US and Germany. The disease primarily affects macaws, conures, and African grey parrots, although all parrots are considered susceptible. Avian bornavirus has been reclassified. The two species known to cause PDD in parrots are psittaciform bornavirus 1 and 2 and include parrot bornavirus (PaBV) genotypes 1–8. PaBV-2 and PaBV-4 are the most commonly reported genotypes in parrots.
Clinical Findings of Avian Bornavirus / Proventricular Dilatation Disease


Courtesy of Dr. Louise Bauck.
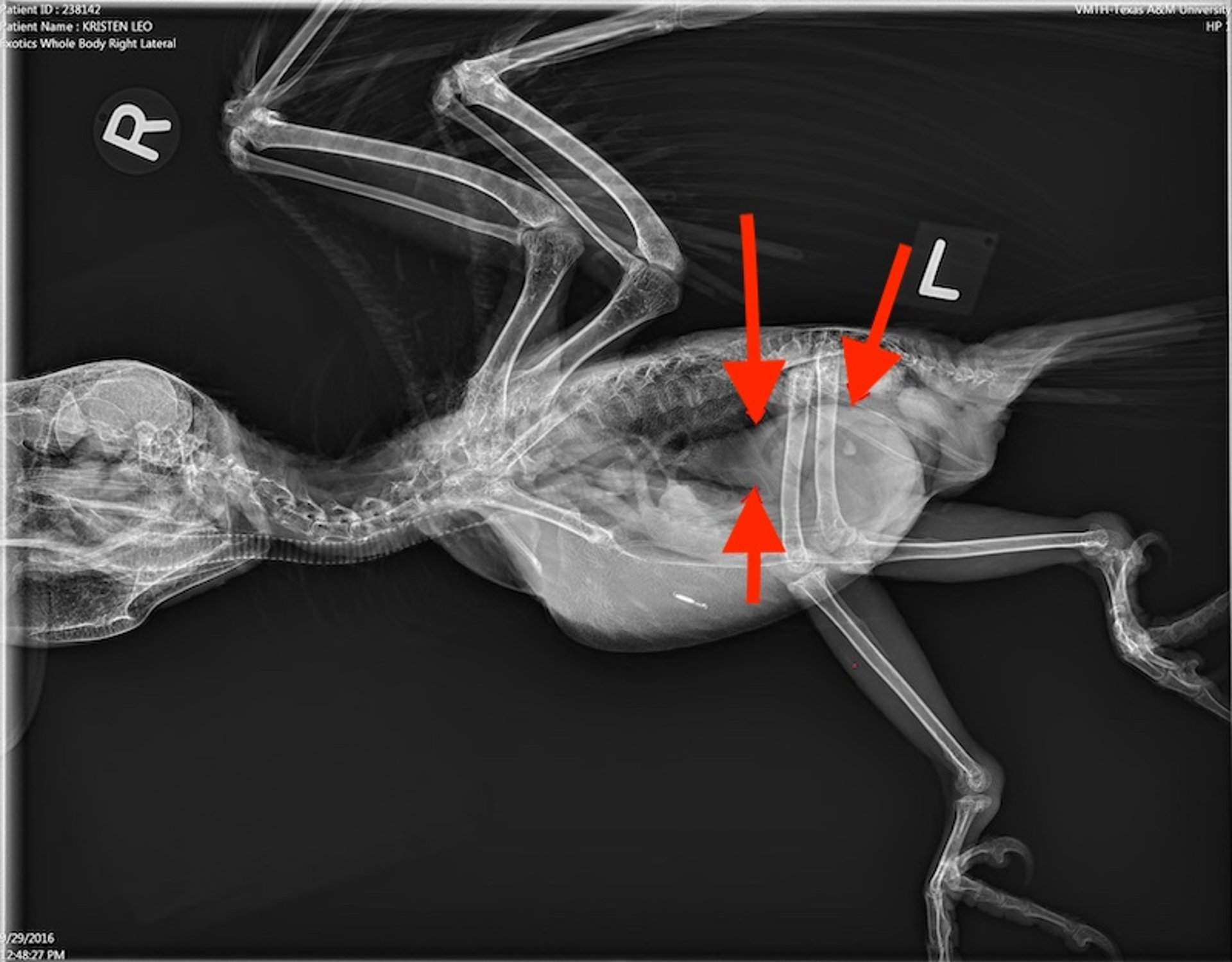
The most common presentation of affected birds is chronic weight loss (often following an initial increase in appetite), passage of undigested food (most easily recognized when whole seeds are found in the droppings), and regurgitation. A dilated proventriculus may be seen radiographically. GI tract signs often reflect pathology of the terminal ganglia of the vagus nerve (cranial nerve X). Secondary bacterial or fungal infections of the nonmotile proventriculus can result in chronic infections and sepsis. Myocarditis related to avian bornavirus/PDD has been reported. Neurologic signs (convulsions, tremors, weakness, ataxia, blindness) may occur in some species, with or without concurrent GI signs. Avian bornavirus is shed in the urine as well as the feces, and some birds may experience polyuria. Clinical signs may be slowly progressive or develop acutely. Outbreaks are sporadic, with a low morbidity and a high mortality.
Transmission of Avian Bornavirus / Proventricular Dilatation Disease in Pet Birds
Avian bornavirus/PDD is contagious, but the actual mode of transmission is not clear. The spread of PaBV and PDD has been well documented, detailing how diseases spread after introduction of an adult bird with fatal PDD into an aviary. Because ABV can be detected in droppings (feces and urine), the fecal-oral route of transmission is considered the most likely, although a recent article investigating different infection routes of parrot bornavirus in cockatiels revealed that transmission of PaBV by oral or intranasal routes was unsuccessful. A second article indicated that transmission of PaBV by direct contact is inefficient in immunocompetent, fully fledged birds.
PaBV is widely distributed in captive and wild bird populations, and the infection is common among captive psittacines in North America and Europe. However, infection does not always cause PDD. Many healthy or subclinical carriers of several species have been documented. In studies in Europe and in North America, as many as 15%–40% of healthy parrots are positive for PaBV. Vertical transmission has not been proved but seems likely.
Diagnosis of Avian Bornavirus / Proventricular Dilatation Disease in Pet Birds
A presumptive diagnosis can be made based on history, clinical signs, and radiographic evaluation. Survey films, radiographs of the GI tract with contrast, and fluoroscopy can aid in diagnosis. The proventriculus is often severely dilated. Contrast studies often reveal delayed transit times throughout the GI tract. Decreased motility may lead to gram-negative or clostridial enteritis. Serum chemistry and hematology are typically normal, although there may be an increased CPK concentration, mild anemia, heterophilia, and/or hypoproteinemia.
PCR assay of the cloaca or feces is the most common test performed. Because shedding of the virus is intermittent, one negative result on a fecal or cloacal PCR test does not exclude disease. Testing at least three times at monthly intervals, with all three tests being negative, is the best evidence to declare a bird negative for ABV. Serologic assays such as ELISA, IFA, and Western blot can also confirm exposure but may not detect early infections, because some PaBV-infected birds do not develop a detectable antibody response until late in the disease process. The assessment of PaBV infection and the diagnosis of PDD is difficult because, although PaBV infection is common, development of clinical PDD is rare. Thus, tests that simply detect the presence of PaBV may not be especially useful for the antemortem diagnosis of PDD.
Some researchers have proposed serologic testing for antiganglioside antibodies, stating that it appears to more accurately detect clinically affected birds. Antiganglioside antibodies are used as markers of immune-mediated disease and are triggered by a variety of pathogens. Other studies have not supported this.
Definitive diagnosis is confirmed by histopathology with characteristic myenteric ganglioneuritis lesions in the crop, ventriculus, or adrenal gland. Ventricular and adrenal gland biopsies are risky and seldom performed. Crop biopsies are reported to be diagnostic of PDD in only about 30%–35% of cases. Failure to observe lesions in the crop does not exclude disease. Proventricular biopsies in affected birds are not done routinely because the proventriculus is prone to dehiscence. Often, PDD is diagnosed at necropsy. Histologic examination should be done on the crop, proventriculus, ventriculus duodenum, adrenal gland, heart, kidney, spleen, and brain.
Interpretation of diagnostic tests for PDD:
A choanal and cloacal RT-PCR with a serologic assay, recognizing that one negative test on all does not exclude infection
A bird that tests positive on both PCR assay and serology should be considered positive and housed separately from birds with negative results
A bird positive by PCR only should be retested in 4–6 weeks and housed separately from other birds until it has three negative tests or is confirmed positive on additional tests
A bird positive on a serology test only should be considered positive and housed separately from birds testing negative
Positive ABV PCR and serology results in a healthy bird do not predict future clinical illness with PDD
Treatment of Avian Bornavirus / Proventricular Dilatation Disease in Pet Birds
Treatment for PDD includes providing supportive care, including easily digestible foods, and may be aided by administration of an NSAID (eg, meloxicam, celecoxib, or robenacoxib). Supportive care may include GI prokinetic agents such as cisapride and metoclopramide to improve GI tract transit. Antimicrobials or antifungals may be necessary for secondary infections. Flaxseed oil at 0.1 mL/kg, PO, daily or a veterinary omega 3 and 6 fatty acid supplement at 0.22–0.44 mL/kg, PO, daily have been advocated and used to reduce inflammation.
Anecdotally, stress has been a factor in development of clinical signs; therefore, methods to reduce stress should be implemented, including practicing good hygiene, providing nutritionally adequate diets, and avoiding overcrowded conditions. Reproductive stress may also exacerbate clinical signs. Leuprolide or the deslorelin implant have been used to reduce reproductive hormones. Gabapentin has been recommended for central or peripheral nervous system signs such as seizures or ataxia. The dose for gabapentin is 10–25 mg/kg, PO, every 12 hours. For birds that self-mutilate, the gabapentin dose is 50 mg/kg, PO, every 12 hours. To date, no antivirals have been effective in treatment or prevention of ABV.
NSAIDs for PDD treatment:
Meloxicam 0.5–1 mg/kg, PO or IM, every 12 hours
Robenacoxib 7–10 mg/kg, IM, every 7 days × 4 weeks then every 4 weeks
Celecoxib 15–30 mg/kg, PO, every 12 hours
Control of Avian Bornavirus / Proventricular Dilatation Disease in Pet Birds
Isolation of positive birds is important in disease prevention. Testing by PCR and serology (a minimum of three tests done 4–6 weeks apart) and separating birds that test positive from those that test negative is a recommended control measure. However, the number of false-negative tests (because of intermittent shedding) makes this a long and potentially difficult task, and clinically healthy birds that test positive for ABV should not be euthanized. ABV is not a long-lived virus in the environment; therefore, good hygiene and ultraviolet light can help to limit spread of disease in a home or aviary setting.
The control of ABV in aviaries and homes requires a multimodal approach:
Practicing good hygiene
Housing birds outdoors when temperatures allow
Avoiding overcrowding and stress and providing good nutrition
Isolating of all new, sick, or ABV-positive birds
Testing existing and newly presenting birds using both serology and multiple (up to three) PCR assays, and housing birds separately based on results.
With the possibility of vertical transmission, chicks from infected birds should be incubator hatched and hand raised, separated from other noninfected birds and monitored for development of disease.
Due to the intermittent shedding and inconclusive serology results, it may take years of testing and separating birds to obtain ABV-negative aviaries.
There is no vaccine available. Vaccine studies are in their infancy.
Poxvirus Infections
The three clinical forms of poxvirus infection are:
Cutaneous form or “dry pox” –wart-like lesions typically on the face, beak, and legs (most common form)
Diphtheritic form or “wet pox” –lesions on the mucosa of the oral cavity and respiratory tract
Septicemic “generalized pox” –internal lesions affecting the respiratory and GI tracts, causing systemic disease
Transmission is primarily via insect vectors (mosquito bites).
Poxviruses are large DNA viruses that induce intracytoplasmic, lipophilic inclusion bodies (Bollinger bodies) in the epithelial cells of the integument, respiratory tract, and oral cavity. All birds are considered susceptible to poxvirus infection, but many companion and aviary birds are rarely exposed to a susceptible strain. In pet bird practice, veterinarians will generally encounter only canary and , pigeon poxviruses, and fowlpox, which have specific host ranges. Poxviruses are environmentally stable, increasing the likelihood that a viable organism will come into contact with a susceptible host. Poxviruses cannot penetrate intact skin, and a break in the skin or mucous membrane must be present for infection to occur.

Courtesy of Dr. Katherine Quesenberry.
Poxvirus infection may cause cutaneous, diphtheritic, or systemic infections based on the strain of virus, route of exposure, affected species, and age and health of the bird. The cutaneous form appears as nodular proliferations or wartlike lesions on the unfeathered skin around the eyes, beak, nares, and legs. The diphtheritic form is characterized by lesions on the mucosa, tongue, pharynx, and larynx. The septicemic form is characterized by a ruffled appearance, depression, cyanosis, anorexia, and wartlike tumors of the skin. The cutaneous form is most commonly seen in psittacines and raptors.
Clinical signs depend on the form of disease, location of the lesions (eye, oral, ear), and overall health of the bird and may include lethargy, respiratory distress, partial blindness, difficulty eating, weight loss, emaciation, and skin lesions.
Diagnosis of poxvirus infection is typically confirmed through history, physical examination findings, and histologic findings of Bollinger bodies in affected tissues.
Treatment is usually nonspecific and may include supportive care, fluids, parenteral vitamin A, ophthalmic ointments for eye infections, assisted feedings, and antimicrobials to prevent or treat secondary infections. Lesions on the skin may need daily cleaning.
Transmission is via insect vectors (mosquito bites) or other entry through breaks in the skin. Therefore, mosquito control and indoor housing are vital to prevent outbreaks. Vaccines for canarypox, fowlpox, and pigeonpox are available but are specific for their host species.
Viscerotropic Velogenic Newcastle Disease
Viscerotropic velogenic Newcastle disease (VVND), caused by a paramyxovirus group 1, affects most avian species and is an important threat to the poultry industry. It is rare in captive-bred parrots housed indoors. Transmission is by respiratory aerosols, fecal contamination of food or water, direct contact with infected birds, and fomites.
Birds may be asymptomatic or die acutely. Clinical signs include depression, anorexia, weight loss, sneezing, nasal discharge, dyspnea, conjunctivitis, bright yellow-green diarrhea, ataxia, head bobbing, and opisthotonos. In prolonged cases, unilateral or bilateral wing and leg paralysis, chorea, torticollis, and dilated pupils also may be seen. Primary differential diagnoses include other paramyxoviruses (non-Newcastle), psittacine proventricular dilatation syndrome, and heavy metal toxicosis. Lesions include hepatomegaly, splenomegaly, petechial or ecchymotic hemorrhages on serosal surfaces of all viscera and air sacs, airsacculitis, and excess straw-colored peritoneal fluid. Diagnosis is traditionally via viral isolation, but agar gel immunodiffusion tests that can be performed on whole blood or serum are available.
Only symptomatic treatment is possible and thus not advised. If suspected, VVND must be reported to appropriate federal and state authorities.
Other Paramyxovirus Infections of Pet Birds
There are several less pathogenic strains of paramyxovirus. Paramyxovirus groups 2 and 3 are endemic in aviculture. Paramyxovirus group 2 causes mild illness in passerines and a more serious disease in psittacines. Clinical signs in psittacines include tracheitis, pneumonia, and enteritis. Paramyxovirus group 3 is reported most frequently in Neophema spp, lovebirds, and gouldian finches and typically causes mild disease. Clinical signs may be absent, and disease results in acute death. In disease of longer duration, respiratory signs, pancreatitis, and torticollis may occur.
Diagnosis is the same as for paramyxovirus group 1. Treatment for paramyxovirus groups 2 and 3 infections is supportive care. The vaccine for paramyxovirus group 1 should not be used in psittacines, because it can cause fatal reactions.
West Nile Virus
West Nile virus (WNV) infection is an arthropod-borne virus in the genus Flavivirus (family Flaviviridae). WNV was first reported in birds in the US in August 1999. WNV has been reported in >320 species of birds. The American crow (Corvus brachyrunchus) and other corvids have suffered particularly high morbidity and mortality. Other affected species include canaries, psittacines, and raptors. Although psittacines appear to be somewhat resistant, the disease has been reported in parakeets, cockatoos, conures, rosellas, caiques, lorikeets, and a King parrot. Affected parrots have been adults housed outdoors with documentation of mosquito populations present. Mosquitoes (Culex spp) are the principal vectors of disease.
Clinical signs include depression, anorexia, weight loss, head tremors, ataxia, blindness, seizures, and death. Juvenile birds are the most commonly affected. Ophthalmologic findings in raptors are anterior uveitis, exudative chorioretinal lesions, and chorioretinal scarring.
Antemortem diagnosis can be difficult. Initial diagnosis may be based on clinical signs, species, and age; however, many diseases may cause similar clinical signs. Serologic tests (serum neutralization) may indicate antibody response to infection. Paired samples submitted 2 weeks apart may reveal a rise in antibody levels and give a more definitive diagnosis. Adult birds may have high circulating antibody levels in endemic areas. PCR assay is available. Diagnosis is often determined at necropsy. The brain and kidney are the preferred tissues to submit for histopathologic examination.
There is no specific treatment for WNV in birds. Some birds may improve with supportive care (fluids, feeding, antimicrobials/antifungals as needed) and time. A vaccination protocol using a recombinant vaccine has been successful in some birds. The recommendation is vaccination of captive birds 2–4 weeks before mosquito season, with a booster 3 weeks after the initial dose.
For control, during the mosquito season, birds should be housed indoors or in completely covered outdoor facilities. Mosquito netting and mosquito traps should be used, and any standing or stagnant water sources eliminated.
Avian Influenza
Avian influenza is caused by an orthomyxovirus. Because of the zoonotic potential of some strains and the recent discovery of new mutations, this virus may become a more important pathogen. Both the zoonotic potential and the economic effects on the poultry industry are causes for concern.
For More Information
Also see pet health content regarding disorders and diseases of pet birds.







