




Bovine leukosis is caused by an oncogenic retrovirus of cattle. Most animals remain asymptomatic despite becoming persistently infected by the virus, but a proportion of cattle will develop lymphosarcoma. Clinical signs are associated with the organ system that is affected by the solid tumor. Infected cattle can be identified using serology or PCR assay.


Courtesy of Dr. Peter Constable.
Lymphosarcoma in cattle may arise spontaneously (referred to as "sporadic") or result from infection with bovine leukemia virus (BLV); the latter is often referred to as an enzootic bovine leukosis. Sporadic lymphosarcoma in cattle is unrelated to infection with BLV. Despite the lack of association, animals with sporadic lymphosarcoma may also be concurrently infected with the virus. Sporadic lymphosarcoma manifests in three main forms:
Juvenile lymphosarcoma occurs most often in animals < 6 months old.
Thymic lymphosarcoma affects cattle 6–24 months old.
Cutaneous lymphosarcoma is most common in cattle 1–3 years old.
Etiology, Transmission, and Epidemiology of Bovine Leukosis
Enzootic bovine leukosis is due to BLV, an exogenous C-type oncogenic retrovirus of the BLV-human T-lymphotropic virus group. BLV has a stable genome, does not cause chronic viremia, and has no preferred site of proviral integration. Despite the lack of preferred proviral integration sites, the tumors generated by the virus in a single individual are typically monoclonal and have a single integration site. The virus escapes the immune response by low levels of viral replication. It appears that replication is blocked at the transcriptional level; however, the mechanism is not completely understood.
The prevalence of BLV infection varies from country to country. Many European countries, Australia, and New Zealand have eradication programs in place that have led to negligible rates of BLV infection. Although voluntary control programs are in place in the US, prevalence is high compared with much of the rest of the world. The most recent surveys in the US estimate that 94.2% of dairy herds contain positive cows with approximately 46.5% of cows infected.1 In beef cattle, estimates are lower, with 38.7% of the herds infected and 10.3% of beef cattle carrying the virus. Prevalence tends to increase on dairies with increasing herd size; however, the converse is true in beef cattle. In general, the prevalence of viral infection increases with age.
Cattle are infected with BLV via the transfer of blood and blood products that contain infected lymphocytes. Once infected, cattle develop a lifelong antibody response, primarily to the gp51 envelope protein and the p24 capsid protein. B lymphocytes harbor the integrated provirus but rarely express viral proteins on their cell surface. The exact site of viral replication and expression that drives the immune response remains elusive.
Under experimental conditions, most routes of viral exposure can successfully transmit infection. However, many of these settings are unlikely to be encountered naturally. Many bodily fluids, including urine, feces, saliva, respiratory secretions, semen, uterine fluids, and embryos, have been examined for their ability to transmit BLV and are considered to be noninfectious. Only on rare occasion has virus been found in these fluids. Colostrum from BLV-positive cows contains virus and has been found to be infectious experimentally. However, colostrum also contains large amounts of antibody, and it is believed that the protective effects of colostral antibody outweigh the infectious potential when colostrum is administered in a normal fashion.
Most BLV transmission is horizontal. Close contact between BLV-negative and BLV-positive cattle is thought to be a risk factor. Many common farm practices have been implicated in viral transmission, including tattooing, dehorning, rectal palpation, injections, and blood collection. Vectors such as tabanids and other large biting flies also may transmit the virus. Vertical transmission may occur transplacentally from an infected dam to the fetus or postpartum from the dam to the calf via ingestion of infected colostrum. Any material that is blood contaminated or lymphocyte rich has the potential to infect animals with BLV.
References
LaDronka RM, Ainsworth S, Wilkins MJ, Norby B, Byrem TM, Bartlett PC. Prevalence of Bovine Leukemia Virus Antibodies in US Dairy Cattle. Vet Med Int. 2018 Nov 11;2018:5831278. doi: 10.1155/2018/5831278. PMID: 30534354; PMCID: PMC6252197.
Pathogenesis of Bovine Leukosis
There are three main outcomes in cattle infected with bovine leukosis virus. Most animals remain persistently infected with no outward clinical signs of infection. Approximately 29% of BLV-infected cattle develop persistent lymphocytosis, while < 5% of BLV-infected cattle develop lymphosarcoma.
Persistent lymphocytosis is sometimes referred to as a preneoplastic syndrome; however, there is no convincing evidence that affected cattle have an increased risk of developing lymphosarcoma. The lymphocytes present in persistent lymphocytosis are not neoplastic, although they may have mild reactive changes consistent with normal blood smears in cattle. Persistent lymphocytosis is considered a benign condition associated with BLV infection. For this reason, it is often overlooked.
However, these cows may serve as a reservoir of infection. The increased lymphocyte count is attributed to a 45-fold increase of infected CD5+ and a 99-fold increase in infected CD5− B cells. It has been suggested that cows with persistent lymphocytosis may be at greater risk of passing BLV infection on to their calves in utero and may show decreased milk production and alteration of milk components.
Lymphosarcoma rarely occurs in animals < 2 years old and is most common in the 4- to 8-year-old age group. Lymphosarcoma, including both sporadic and enzootic forms, is one of the main causes of condemnation of adult dairy cows at slaughter in the US.
Clinical Findings:


Courtesy of Dr. Dusty Nagy.


Courtesy of Dr. Dusty Nagy.

Courtesy of Dr. Dusty Nagy.
Clinical signs associated with development of lymphosarcoma are highly variable, because the affected organ(s) will dictate the predominant clinical signs.
Juvenile lymphosarcoma is often characterized by a sudden onset of diffuse lymphoid hyperplasia with or without visceral organ involvement. Weight loss, fever, tachycardia, dyspnea, bloat, and posterior paresis have all been described with this form of lymphosarcoma. Profound lymphocytosis (> 50,000/mcL) often accompanies this fatal form of bovine lymphosarcoma. Thymic lymphosarcoma may involve the cervical or intrathoracic thymus, or both.
Clinical signs associated with this form of lymphosarcoma depend heavily on the location and size of the tumor. A cervical swelling may be evident. Dyspnea, bloat, jugular distention, tachycardia, anterior edema, and fever have been documented. The affected cell population is an immature, poorly differentiated lymphocyte. Cutaneous lymphosarcoma presents as cutaneous plaques, 1–5 cm in diameter, on the neck, back, rump, and thighs. Regional lymph nodes may also be enlarged. This form of lymphosarcoma may undergo spontaneous remission; however, relapses may occur.
Lesions
Animals with BLV-associated lymphosarcoma commonly show lesions in the central or peripheral lymph nodes, leading to lymphadenopathy. Lesions of the abomasum may lead to clinical signs of cranial abdominal pain, melena, or abomasal outflow obstruction. Pelvic limb paresis progressing to paralysis can occur in animals with extradural spinal lesions. Retrobulbar lesions cause protrusion of the globe, resulting in exposure keratitis and eventually proptosis. Lesions of the right atrium may be mild and undetectable clinically, or may cause arrhythmias, murmurs, or heart failure. Uterine lesions may lead to reproductive failure or abortion. Lesions of the internal organs typically involve the spleen, liver, or kidneys and ureters. Lesions of the spleen are often initially asymptomatic but may result in rupture of the spleen and exsanguination into the peritoneal cavity.
Lymphosarcoma of the liver is often asymptomatic but may lead to jaundice and liver failure. Disease of the kidney and ureter can lead to abdominal pain and the subsequent development of hydroureter or hydronephrosis and clinical signs associated with renal failure.
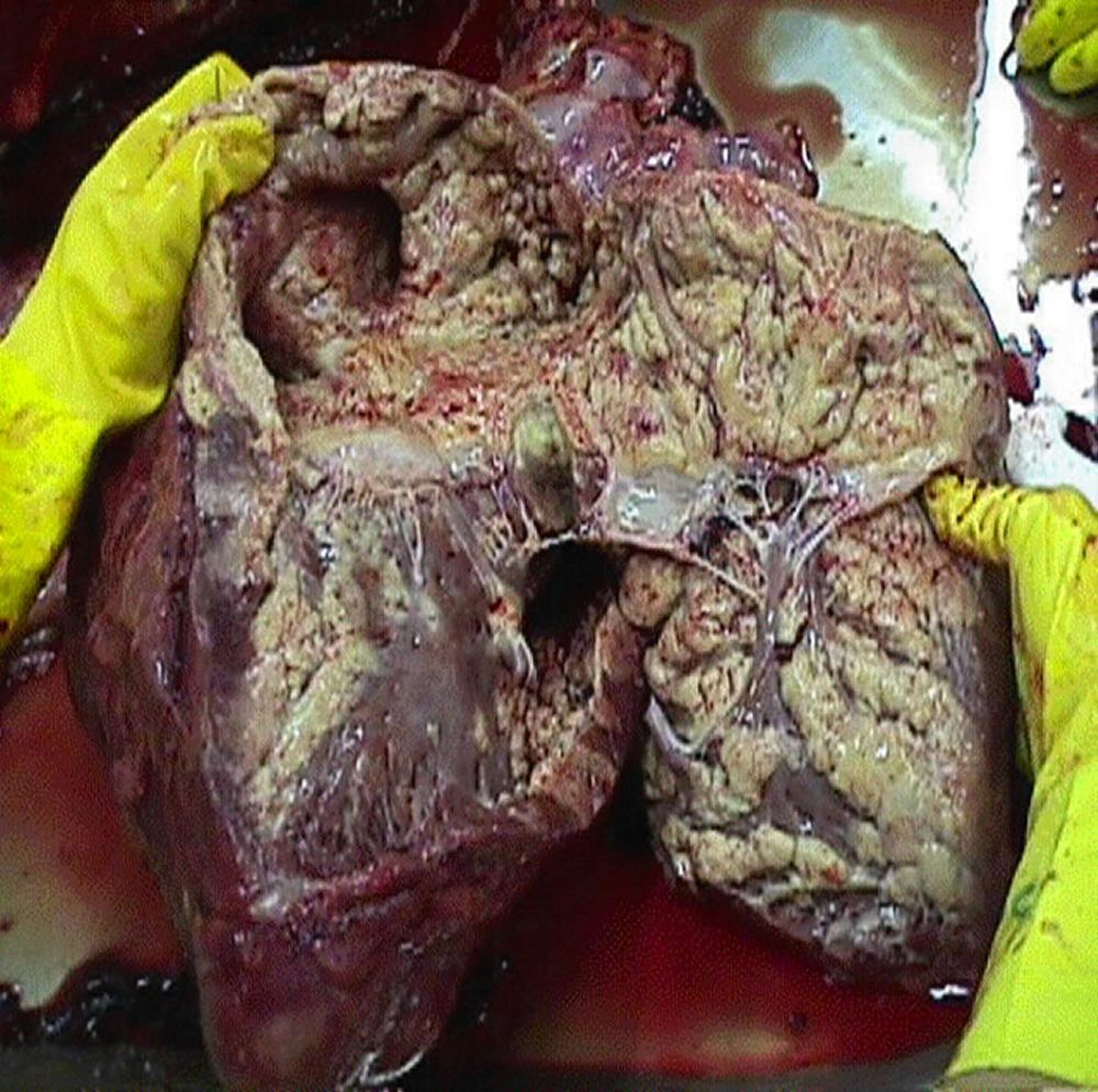
Lymphosarcoma may appear as yellow-tan, discrete nodular masses or a diffuse tissue infiltrate. The latter pattern results in an enlarged, pale organ and can be easily misinterpreted as a degenerative change rather than neoplasia. Histologically, the tumor masses are composed of densely packed, monomorphic lymphocytic cells.
Diagnosis of Bovine Leukosis
Serologic testing
Cytology or histologic examination of biopsy samples
Lymphosarcoma is often included on the differential diagnosis list for many diseases because of the wide range of clinical findings. Viral infection is diagnosed by serology or virology, persistent lymphocytosis is identified by hematology, and neoplastic tumors are identified by histologic examination of biopsies. Positive serology or virology testing for BLV confirms viral infection but not the presence of lymphosarcoma.
Serologic testing by means of ELISA is the most common and reliable way to diagnose infection with BLV. Serology is unreliable in calves that have ingested colostrum from BLV-positive cows because of the passive acquisition of maternal antibodies that typically wane by 4–6 months old. PCR is a sensitive and specific assay for diagnosis of BLV infection in peripheral blood lymphocytes. This test can identify proviral DNA of BLV in the lymphocytes of infected animals and differentiate positive from negative calves in the presence of maternal antibodies.
The diagnosis of lymphosarcoma must be made by cytology or histopathology. Cytologic diagnosis is sometimes difficult because of the frequency of blood contamination of the aspirates.
Treatment and Control of Bovine Leukosis
No viable treatment
Limit transfer of infected lymphocytes from one cow to another
There is no treatment for viral infection or for lymphosarcoma in cattle, although parenteral corticosteroids can transiently decrease the severity of clinical signs. Eradication programs have been developed; however, success has been variable, primarily because of the expense and high prevalence of infection among cattle in the US relative to the economic cost of disease. The most commonly recommended eradication protocol is as follows:
identify infected animals using a serologic test
cull seropositive animals immediately
retest the herd in 30–60 days
use PCR assay to test young calves and as a complementary test to clarify test results in herds with a low prevalence of infection
repeat testing and cull until the entire herd tests negative
Testing is then repeated every 6 months. The herd is declared free when there have been no positive tests for 2 years. Additions to the herd should have two negative tests 30 and 60 days before arrival.
When test and cull programs are economically untenable, test and segregation programs have been recommended but are rarely implemented. These programs necessitate running two completely separate operations and require additional resources, including money, time, and available workforce.
Prevention of Bovine Leukosis
Eliminating the exposure to blood from infected animals to naive animals is the cornerstone of prevention protocols for bovine leukosis. In calves, feeding colostrum from seronegative cows is often advocated. However, most epidemiologic evidence suggests that the protective effect of colostral antibody outweighs the risk of infections, particularly in high-prevalence herds. The replacement of whole milk feeding with high-quality milk replacer may also be considered. Bloody milk should never be fed to calves.
Cautery or other bloodless methods of dehorning should be used. Equipment used for castration, tattooing, or implanting should be adequately cleaned and disinfected between animals.
Transmission can be decreased in adult cattle by changing rectal sleeves in between cows. Artificial insemination or embryo transfer (using negative recipients) may limit transmission. In beef herds, the use of a negative bull may limit transmission; however, natural service is an uncommon method of viral transmission unless breeding is traumatic or the bull has vesiculitis or another reproductive disease that may lead to semen contamination with blood or infected lymphocytes.
Additional recommendations include:
disinfecting equipment that has come in contact with blood or body tissue
using single-use, disposable needles for blood collection and IM injections (It is preferable to use single-use disposable needles for vaccination; however, the risk of transmitting BLV virus via subcutaneous vaccination is low.)
cleaning handling facilities between animals when contaminated with blood
cleaning maternity and calving pens after each animal to prevent contaminated fluids from coming into contact with the next animal
controlling flies to help minimize the potential for tabanid-associated transmission, although this route of infection is considered to be minor
screening blood donors carefully; transfusions and vaccines containing blood, such as those used for babesiosis and anaplasmosis, are particularly potent ways to transmit the disease
Zoonotic Risk of Bovine Leukosis
In veterinary medicine, bovine leukemia virus is not typically thought of as zoonotic. However, there is research within demonstrating viral DNA in human lung, mammary, and buffy coat cells.1-3 There is interest in the virus’s ability to potentially affect regulatory pathways and oncogenesis in human cancer. There is some evidence that the virus is more commonly found in malignant vs benign human tissue samples.4 One study looking at risk factors for human infection found ingesting unpasteurized dairy products such as milk and yogurt to be a risk. Ingestion of other products, such as cheese and commercial milk, as well as contact with cows, were not considered to be risk factors.4 Although the virus has been detected in people, and some associations have been made, there is considerable knowledge needed to clarify the risk of animal interactions with people and of BLV as a human zoonosis.
References
Robinson LA, Jaing CJ, Pierce Campbell C, et al. Molecular evidence of viral DNA in non-small cell lung cancer and non-neoplastic lung. Br J Cancer. 2016;115:497–504.
Mes G, Ulloa JC, Uribe AM, et al. Bovine Leukemia Virus Gene Segment Detected in Human Breast Tissue. Open J Med Microbiol. 2013;3:84–90.
Buehring GC, DeLaney A, Shen H, et al. Bovine leukemia virus discovered in human blood. BMC Infect Dis. 2019;19:297. https://doi.org/10.1186/s12879-019-3891-9
Corredor-Figueroa AP, Olaya-Galán NN, Velandia-Álvarez S, et al. Co-Circulation of Bovine Leukemia Virus Haplotypes among Humans, Animals, and Food Products: New Insights of Its Zoonotic Potential. Int J Environ Res Public Health. 2021;18:4883. https://doi.org/10.3390/ijerph18094883
Key Points
Lymphosarcoma in cattle can be sporadic (juvenile multicentric, thymic, and cutaneous) or secondary to infection with bovine leukosis virus (enzootic bovine leukosis). Prevalence of viral infection and BLV-induced lymphosarcoma vary by country.
Most virally infected animals appear clinically normal, while clinical signs in animals with cancer vary depending on the organ system that is infected.
Prevention relies on eliminating transmission between cattle via exposure to contaminated blood and tissues; fly control; equipment and facility disinfection; and single-use needles.
For More Information
Bovine leukemia virus (BLV). Animal and Plant Health Inspection Service. USDA. Updated March 5, 2021.




