




Feline infectious peritonitis is a severe, immune-mediated coronaviral disease of cats. Effusion and pyogranulomatous inflammation are clinical hallmarks. Diagnosis requires a multimodal approach; analysis of effusion, if present, or fine-needle aspirates from affected organs can be helpful, but histological evaluation with feline coronavirus antigen detection is usually needed for definitive diagnosis. Antivirals such as nucleoside analogues and protease inhibitors show promise for safe, effective treatment; however, they are not available in all countries.
Feline infectious peritonitis (FIP) ranks among the most important infectious diseases and causes of death in cats. Diagnosis is challenging. FIP was once considered universally fatal, but new antivirals show promise for safe, effective treatment.
Etiology and Pathophysiology of Feline Infectious Peritonitis
FIP is caused by certain strains of feline coronavirus (FCoV).
Taxonomy
FCoV is classified in the order Nidovirales, family Coronaviridae, subfamily Coronavirinae, genus Alphacoronavirus, and species Alphacoronavirus 1, which also includes the strains canine coronavirus and porcine transmissible gastroenteritis virus.
Structure
FCoV virions are large (120–160 nm in diameter); roughly spherical, with moderate pleomorphism; and enveloped with a thick biomembrane. The envelope is decorated with 15- to 20-nm club-shaped or petal-shaped surface projections (“peplomers” or “spikes”) composed of trimers of the spike (S) glycoprotein (see genome organization and virion morphology illustration). On images produced by electron microscopy, the characteristic fringe of spikes is said to resemble the solar corona.


Courtesy of Dr. Nicholas Roman.
The nucleocapsid comprises the viral genome and multiple copies of a single basic phosphoprotein species (N). The nucleocapsid is loosely wound and is folded into a compact core separated from the envelope by ~4 nm.
Classification
Like other coronaviruses, FCoV has a positive-sense single-stranded RNA genome (Baltimore classification group IV) of linear topology encoding the structural proteins S (spike), E (envelope), M (membrane), and N (nucleocapsid) and the nonstructural proteins 3a, 3b, 3c, 7a, and 7b. Open reading frames 1a and 1b encode RNA replicase proteins. See genome organization and virion morphology schematic.
Of RNA viruses, the Coronaviridae have the largest and most genetically complex genomes identified to date. As with other coronaviruses, the large genome sequence of FCoV (26–32 kb) is prone to high rates of mutation and subject to considerable genetic variability (owing to the high error rate and lack of proofreading ability of RNA polymerase, rapid and continuous replication, genome recombination as a result of template switching, and reassortment of segmented RNA genomes). Therefore, infected cats shed a heterogeneous cluster of related but distinct viral populations, known as a quasispecies, molecular swarm, or mutant cloud.
Differing antigenicity (neutralizing antibody reactions) enables the division of FCoV into two serotypes, each encompassing numerous strains:
Serotype I is most prevalent in cat populations.
Serotype II is a recombinant form of FCoV and canine coronavirus in which spike genes (S proteins) are replaced by canine coronavirus spikes.
Serotype II is easily grown in cell culture; serotype I is difficult to culture. All FCoV infections have the potential to cause clinical FIP in cats.
The pathogenesis of FIP involves conversion to a virulent biotype or pathotype referred to as the feline infectious peritonitis virus (FIPV). The exact mutation that determines FIPV is unknown, but it may involve the 3c gene. Two single nucleotide polymorphisms leading to amino acid changes (M1058L and S1060A) in the fusion peptide of the S protein have been linked to the biotype switch. Because they are identified also in some healthy cats, however, these changes may be linked only to the systemic dissemination of FCoV and not necessarily to the development of FIP.
For FIP to develop, mutations in FIPV must lead to entry, persistence, and efficient replication within and activation of monocytes or macrophages.
Replication Cycle
In brief, the replication cycle of FCoV includes the binding of virus particles to dedicated host cell surface receptors (aminopeptidase N for FCoV serotype II, and an unknown receptor for FCoV serotype I). Attachment is mediated by spike proteins.
FCoV virions release their genome into the target cell via fusion of the viral envelope with the plasma membrane or the limiting membrane of an endocytic vesicle.
The intracellular site of the FCoV replication cycle is in the cytoplasm, and the virion is assembled in the endoplasmic reticulum or Golgi apparatus. Coronaviruses acquire their lipid envelopes by budding at membranes of the endoplasmic reticulum, intermediate compartment, or Golgi complex.
Mature FCoV particles are released by exocytosis.
Pathogenic Mechanisms
Coronaviruses target primarily epithelial cells and are typically associated with acute or chronic GI and respiratory infections. Some coronaviruses can cause severe or even lethal disease.
Most strains of FCoV are found in the GI tract (ie, feline enteric coronavirus [FECoV]) and often remain subclinical or cause mild, self-limiting clinical signs (eg, GI signs like vomiting or diarrhea).
FCoV replicates in mature apical columnar epithelial cells of small intestinal villi from the distal duodenum to the cecum.
Some cats develop persistent infection of colonic columnar epithelial cells with prolonged shedding of high viral loads; however, most infected cats develop intermittent, temporary, minimal shedding, and in rare cases they either never shed virus or quickly cease shedding.
Cats can be repeatedly infected with the same or different FCoV strains.
According to the internal mutation hypothesis, in a small proportion of cats persistently infected with FCoV, spontaneous mutations alter the biological behavior of the virus, leading to a change in cell tropism from enterocytes to cells of the macrophage or monocyte lineage. FIPV-infected monocytes attach to endothelium or cross the vessel wall (via extravasation), enabling the dissemination of virus throughout the cat’s body.
Both viral genetic factors and host response play a role in the clinical manifestation of FIP as a fatal immune-mediated multisystemic infection.
Antibodies, macrophages, and neutrophils are attracted to FIPV; antibody-dependent enhancement may facilitate uptake of the virus by macrophages. Infected macrophages overproduce neutrophil survival factors, upregulating neutrophil survival.
Complement fixation leads to release of vasoactive amines. The formation of immune complexes contributes to blood vessel damage and vasculitis. With increased vascular permeability and vessel fluid leakage, protein-rich effusions develop.
Perivascular pyogranulomatous inflammation in the tissues where infected cells collect produces widespread granulomatous lesions in multiple sites (commonly abdomen, kidneys, or nervous system).
Epizootiology of Feline Infectious Peritonitis
Geographic Distribution
FCoV is ubiquitous in most feline populations globally, except for isolated populations on a few islands (eg, the Falkland Islands).
Measures of Disease Frequency
The seroprevalence of FCoV in single-cat households and free-roaming cats is ~15%. The seroprevalence of FCoV in high-density environments (eg, multicat households, breeding catteries, shelter and rescue facilities, and hoarding situations) is ~50%–90%.
The incidence of FIP varies. FCoV infection progresses to FIP in ~5%–12% of affected cats (1).
Transmission
FCoV is highly communicable and is transmitted via the fecal-oral route or via fomites. The most common mode of transmission is from infected queens to their kittens.
Infection almost exclusively involves the less virulent, nonmutated FCoV biotype. The FIPV biotype is not considered communicable; rather it is believed to develop independently in individual cats (internal mutation hypothesis), and only minimal amounts of FIPV are shed in their feces.
Outbreaks of FIP have been documented in catteries and shelter environments in the US, the UK, Greece, and Taiwan. In January 2023, an unusual, widespread outbreak of suspected FIP began on the island of Cyprus. Cyprus has a high number of stray and free-roaming owned cats; however, cases were also reported in indoor-only cats. The outbreak raises concern not only that a new, highly virulent strain of FCoV has emerged but that it may be transmitted by mechanical vectors (ie, a postulated explanation for how cats isolated indoors could have contracted the disease). Investigation of this outbreak is ongoing (2, 3).
Risk Factors
Any cat that carries FCoV is potentially at risk of developing FIP; however, several additional risk factors have been identified:
group housing in multicat environments
young (< 2 years old) and geriatric (> 10 years old) ages
sexually intact neuter status
male sex
purebred lineage (including Abyssinian, Bengal, Birman, Himalayan, Ragdoll, and Rex [Cornish and Devon varieties]) (4)
recent stress (eg, rehoming, elective surgery, concurrent illness, boarding)
retroviral infection
Incubation Period
Cats infected with FCoV usually mount an immune response with antibody production within 7–10 days of infection.
The incubation period for FIP is variable, ranging from days or weeks to months or years.
Morbidity and Mortality
FCoV infection progresses to FIP in ~5%–12% of affected cats (1). Once a cat has developed clinical FIP, the disease is usually progressive and, without effective treatment, almost always fatal. FIP is estimated to cause the death of 0.3%–1.4% of all cats examined at veterinary institutions worldwide (4, 5, 6).
Hosts or Species Affected
Both domestic and wild Felidae—particularly cheetahs, but also bobcats, caracals, cougars, jaguars, leopards, lions, lynx, sand cats, and servals—are susceptible to FCoV infection and the development of FIP.
Zoonotic Risk
FCoV infection is not considered a zoonotic risk. However, some coronaviruses that infect animals can be transmitted to and among humans. Examples include severe acute respiratory syndrome coronavirus (SARS-CoV), severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and Middle East respiratory syndrome (MERS).
In 2010, feline-like coronavirus strains were detected in respiratory swabs from humans with acute respiratory signs who tested negative for influenza in Arkansas. This event represented possible evidence of interspecies transmission, a new human strain, or recombination of a feline coronavirus (7).
During an outbreak in 2017–2018, a novel canine-feline recombinant alphacoronavirus was isolated from respiratory samples of a group of children with pneumonia in Malaysia (8).
Clinical Findings of Feline Infectious Peritonitis
Disease Characterization
Cats infected with FCoV may develop mild, self-limiting clinical signs (eg, mild GI signs like vomiting or diarrhea). Often the infection is subclinical.
Onset of FIP is insidious, and the severity increases progressively.
The clinical signs of FIP are variable. Effusion is the most typical; however, it is not always present. On this basis, two main but overlapping clinical forms of FIP are distinguished: effusive FIP (also called wet FIP or nonparenchymatous FIP) and noneffusive FIP (also called dry FIP or parenchymatous FIP).
The signs of effusive FIP are those that characterize vasculopathy (ie, leakage of serum protein and fluids into body cavities).
Ascites may be accompanied by a pot-bellied appearance with or without a palpable fluid wave.
Pleural effusion may be accompanied by tachypnea, dyspnea, cyanotic mucous membranes, or muffled heart sounds.
Uncommonly, pericardial effusion has been associated with FIP.
Other abnormalities may include icterus, lymphadenomegaly, scrotal edema (due to serositis of the tunica vaginalis of the testes), and lameness (due to synovitis).
The signs of noneffusive FIP are those that characterize granuloma formation in organs. Findings depend on the organ systems affected (commonly kidneys, liver, intestines, abdominal lymph nodes, brain, and eyes) and can be vague.
Ocular abnormalities are common.
With anterior uveitis, which may be unilateral or bilateral, aqueous flare, hyphema, hypopyon, fibrinous exudate, miosis, and keratic precipitates in the anterior chamber may be detected (see anterior uveitis photograph). Panuveitis is also possible.
Chorioretinitis can lead to retinal perivascular cuffing due to inflammatory cell infiltrates or focal to diffuse retinal hemorrhages, subretinal edema, or retinal detachment. Blindness may be a sequela.
Neovascularization of the iris may be noted.
With nervous system involvement, neurological sequelae reflect neuroanatomical localization in the brain, meninges, spinal cord, or peripheral nerves (eg, ataxia, seizures, tremors, abnormal mentation or behavior, abnormal postural reflex reactions, hyperesthesia, nystagmus, anisocoria or dyscoria, cranial nerve deficits, paresis, circling, head tilt, urinary incontinence, and cortical blindness).
Abdominal lymphadenomegaly and nodular irregularities on the surface of normal-sized or enlarged kidneys, liver, or other abdominal organs may be palpable.
Focal granulomas in the intestinal tract may produce palpably thickened loops of bowel. Omental and visceral adhesions may be detectable as palpable abdominal masses. Associated GI signs may include vomiting, diarrhea, or obstipation.
With granulomatous pneumonia, dyspnea and other respiratory signs may be noted.
Pyogranulomatous necrotizing dermal phlebitis or vasculitis may produce nodules or papules that may or may not be associated with pruritus.


Courtesy of Dr. Nicholas Roman.
Irrespective of the presence of effusion, nonspecific clinical signs such as lethargy, hyporexia to anorexia, weight loss or failure to gain weight, and fluctuating fever that does not respond to antimicrobials are common in cases of FIP.
The wet and dry FIP forms are not strictly separate clinical entities. A mixed form may be present, cats with the dry form may develop effusion, and pyogranulomatous lesions are found at necropsy in cats with effusive FIP.
Postmortem Lesions
Perivascular pyogranulomatous lesions, especially on serosal surfaces, are the hallmark of FIP (see necropsy photograph). Cavitary fluids (peritoneal, pleural, and, uncommonly, pericardial effusion) may be present. Lymphadenopathy, icterus, and ocular pathological changes are common.


Courtesy of Dr. Nicholas Roman.
Diagnosis of Feline Infectious Peritonitis
Histological evaluation
Effusion analysis
Integration of various diagnostic modalities
Antemortem clinical and laboratory diagnosis of FIP can be difficult, owing to the lack of pathognomonic clinical signs or laboratory changes, particularly when effusion is not evident or there is concurrent disease.
Multiple diagnostic testing modalities may be needed, guided by the history, signalment, clinical signs, physical examination findings, and characteristics of effusion (if present).
Histological Evaluation
Definitive diagnosis of FIP historically has relied on histopathologic findings—usually, the detection of intracellular FCoV antigen associated with macrophages within lesions by immunohistochemistry or immunocytochemistry. Often, postmortem samples (tissues [mesenteric lymph nodes, small and large intestine, omentum, spleen, kidney, liver], effusions, CSF, and aqueous humor) are used.
Because cats suspected of having FIP are generally too ill to undergo invasive sampling, less invasive methods such as fine-needle aspiration may be considered. In cases involving effusions with biochemical and cytological features consistent with FIP, immunostaining of FCoV antigen in effusion fluid samples is also an option.
Effusion Analysis
In cases of wet FIP, tests of effusion fluid generally have higher positive predictive values than do blood tests. Fluid samples can be obtained via centesis (eg, abdominal paracentesis, thoracocentesis) with or without ultrasonographic guidance.
Effusions associated with FIP are characteristically yellow to straw-colored, clear to cloudy, and sticky and viscous (described as similar to egg whites) in consistency. However, these findings are not definitive (some cats with FIP have effusions that are pink or watery), nor are they sufficient for diagnosis.
Effusions associated with FIP are typically classified as modified transudates or exudates. Typically, the fluid contains high protein concentrations (> 35 g/L; albumin:globulin ratio < 0.4), and the cell count is low to moderate (< 5 × 109 cells/L). Some FIP effusions have very high cell counts (eg, in the case of secondary bacterial peritonitis or pleuritis), and chylous effusions have been reported (but these are more characteristic of other causes of effusion).
Typical findings on cytological evaluation of FIP effusion include a highly proteinaceous, granular, eosinophilic-staining background with a nonseptic cellular component consisting of macrophages, nondegenerate neutrophils, and very few lymphocytes (ie, pyogranulomatous inflammation). See cytological effusion image.

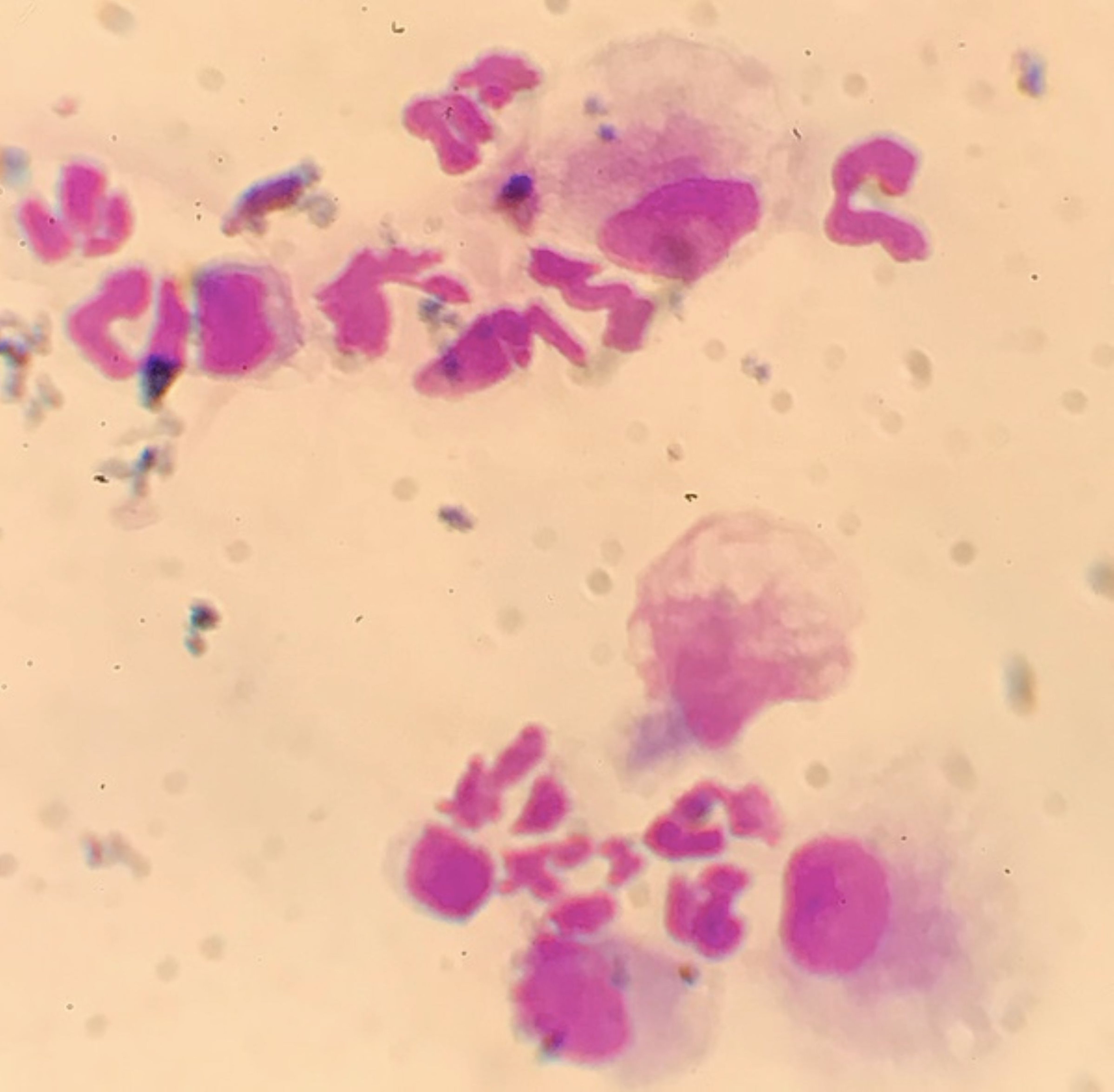
Courtesy of Dr. Nicholas Roman.
The Rivalta test is a useful method to help rule out FIP. A drop of effusion fluid is added to a dilute acetic acid solution (20–30 mcL of 98% acetic acid in 7–8 mL of distilled water).
Positive result: In the presence of highly proteinaceous content, fibrin, and inflammatory mediators, which are common to FIP effusions, the drop precipitates—retaining its shape and staying at the fluid surface or slowly sinking. Although not specific, when combined with other findings (eg, signalment, cytological evaluation of effusions, other diagnostic testing), a positive result raises the index of suspicion of FIP.
Negative result: If the drop dissipates, FIP is very unlikely (high negative predictive value).
Interpretation of the Rivalta test is somewhat subjective and can be challenging, depending on the interpreter’s experience.
PCR Assays and Molecular Characterization
Reverse transcription quantitative real-time PCR (RT-qPCR) assay can detect FCoV RNA in a variety of samples (eg, blood, effusion, CSF, aqueous humour, tissue, feces), potentially supporting a diagnosis of FIP in the context of other evidence. However, FCoV viremia does not necessarily predispose to development of FIP. False-negative results are also possible (eg, because of degradation of RNA by RNases, mutations of the virus, invalid primers).
PCR primers generally are not able to distinguish between FIPV and FCoV biotypes. There is a discriminative RT-qPCR assay or gene sequencing (or combination in a multiplex assay) which can detect gene mutations at two nucleotide positions in the fusion peptide of the spike (S) protein of FCoV, which is linked to biotype conversion of FCoV to FIPV. However, compared with PCR assay detection of FCoV alone, detection of S gene mutations may only minimally improve the ability to diagnose FIP. False-positive results have been documented (indicating a lack of specificity), and there are many different FCoV strains or variants with variable spike gene nucleotide sequences (9, 10).
Diagnostic Imaging
For cats that are suspected of having FIP but lack a noticeable abdominal fluid wave, abdominal focused assessment with sonography for trauma (AFAST) is a useful point-of-care test for screening or serial monitoring.
If free fluid is not detected on AFAST but the clinical suspicion for FIP is high, abdominal ultrasonography more readily detects small amounts of fluid. Abdominal ultrasonographic findings consistent with FIP include peritoneal or retroperitoneal effusion and soft tissue abnormalities (abdominal lymphadenomegaly, abdominal masses, thickened loops of intestines, and changes in visceral echogenicity [renal, hepatic, etc]).
Thoracic and abdominal radiography may provide evidence of cavitary effusions, as well as mass effects (see ascites radiograph). Thoracic radiography is usually diagnostic for pleural effusion.

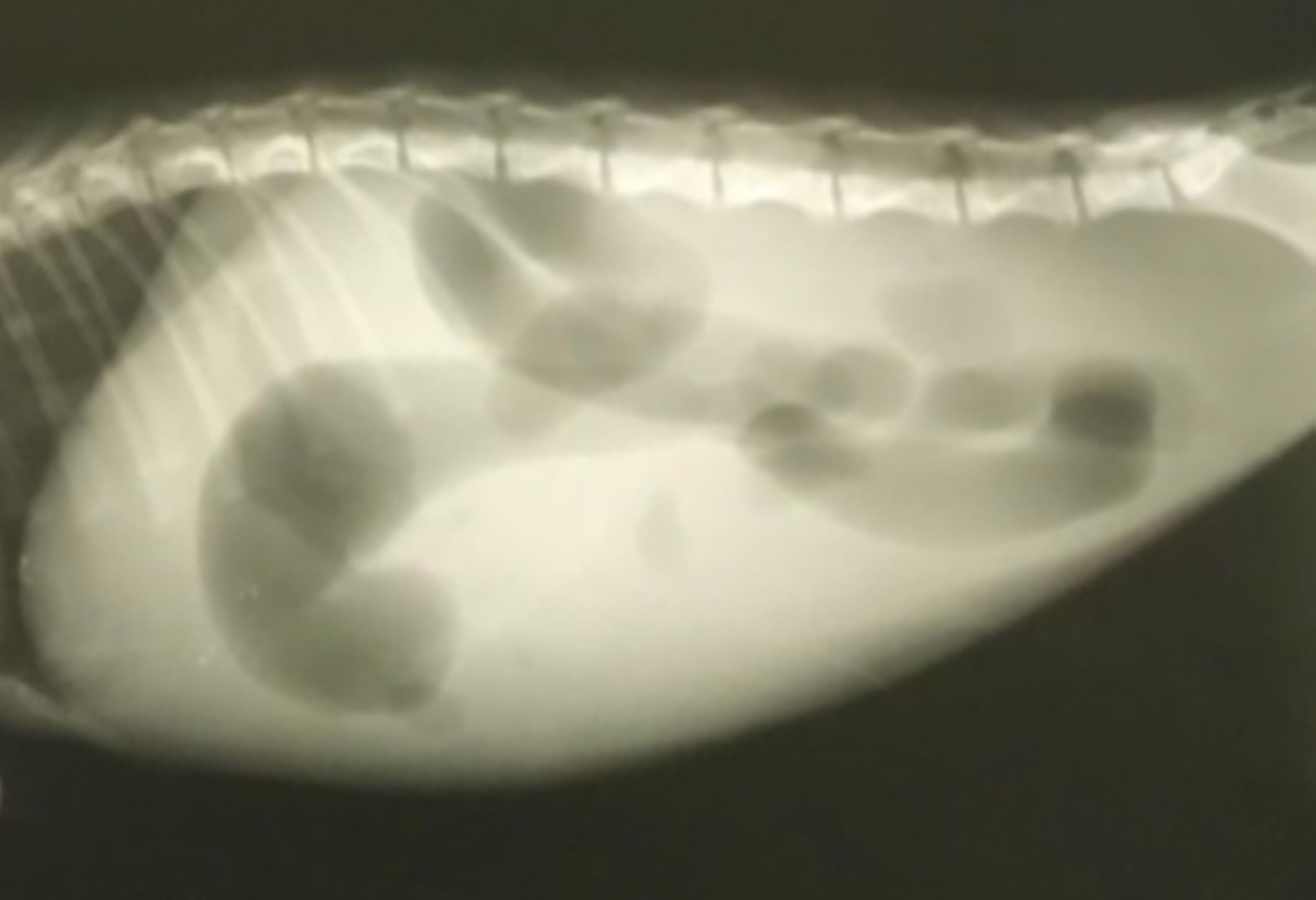
Courtesy of Dr. Nicholas Roman.
Advanced imaging such as MRI or CT may be useful, especially in cases involving neurological signs, for characterizing the extent of disease and ruling out differential diagnoses.
Clinicopathologic Data
Hematologic abnormalities considered typical for FIP include lymphopenia, neutrophilia, anemia, and thrombocytopenia.
Serum biochemical abnormalities considered typical for FIP include hyperproteinemia (polyclonal increase in gamma globulins), hyperglobulinemia, hypoalbuminemia, and hyperbilirubinemia. Hyperglobulinemia also occurs in lymphoma, multiple myeloma, and chronic infection.
FIP-associated glomerulonephritis often results in proteinuria.
Concentrations of the acute phase protein alpha-1-acid glycoprotein (AGP) can be elevated (> 1.5 mg/mL) in plasma and effusions from cats with FIP. However, AGP concentrations can be elevated with other infectious diseases and neoplasia as well.
Cerebrospinal Fluid Analysis
In cats with neurological signs of FIP, CSF analysis may reveal marked pleocytosis (> 100 cells/mcL, mostly neutrophils), a high protein concentration (> 200 mg/dL), and an FCoV antibody titer > 1:25.
Serological Testing
Whether performed on effusion fluid or serum, measurement of FCoV antibody titers is often unhelpful. Because most cats in the general population have been exposed to the virus, interpretation is fraught (ie, titers can be elevated as a result of prior exposure to FCoV and not because of FIP, and most seropositive cats never develop FIP). Furthermore, some cats with FIP have low FCoV antibody titers or seronegative results (because binding by the virus may prevent antibodies from reacting with test antigens).
Differential Diagnoses
The following diagnoses may be accompanied by pathological manifestations and clinical signs similar to those of FIP:
septic peritonitis or pleuritis
retroviral disease (feline immunodeficiency virus [FIV] or feline leukemia virus [FeLV] disease)
lymphoma or other neoplasia
pyothorax or chylothorax
trauma
lymphocytic plasmacytic cholangitis
mycobacteriosis
The following diagnoses may be accompanied by ocular signs similar to those of FIP:
toxoplasmosis
retroviral disease (FIV or FeLV)
systemic mycosis
These differential diagnoses can sometimes be challenging to rule out.
Treatment, Control, and Prevention of Feline Infectious Peritonitis
Antivirals
Supportive care
Historically, FIP was considered to have no effective treatment. Several antiviral drugs under study have shown promise as potentially safe, effective treatments; however, they remain unlicensed or are not legally available in many countries at this time.
Antiviral Treatment
The nucleoside analogue GS-441524 is the active metabolite of the prodrug remdesivir (GS-5734). Both remdesivir and GS-441524 have been found to be effective for FIP treatment (11). Reported dosages are 2–15 mg/kg, IM, every 24 hours for at least 12 weeks.
These drugs hamper viral replication via delayed chain termination. Once the drug is inside the cell, phosphorylation by cellular kinases produces a nucleoside monophosphate and then an active nucleoside triphosphate metabolite, which competes with natural nucleoside triphosphates used as substrates in viral RNA synthesis. Incorporation of the nucleoside analogue into the nascent viral RNA transcript results in the premature termination of the nucleic acid chain.
GS-441524 remains under patent and is not approved for veterinary use in some countries. Unlicensed GS-441524–like antiviral drugs for oral administration are commercially available. Reported adverse effects include injection-site discomfort, nonprogressive renal toxicosis, steroid-responsive vasculitis-type reactions, and urolithiasis (12, 13, 14).
Clinical improvement of FIP has been demonstrated with the 3c-like protease inhibitor GC376 (15 mg/kg, SC, every 12 hours for 12 weeks). In the US, FDA approval is pending. Adverse effects of GC376 include injection-site discomfort and interference with adult dentition development in kittens (15, 16, 17, 18).
Clinical remission of FIP has been reported with the nucleoside analogue molnupiravir (12.8–14.6 mg/kg, PO, every 12 hours for 10–15 weeks [median, 12 weeks]) as a rescue treatment in cats with persistent or relapsed clinical signs of FIP after treatment with GS-441524 or GC376. Reported adverse effects of molnupiravir include folded ears, broken whiskers, and leukopenia (19, 20, 21, 22).
FCoV replication is inhibited by feline interferon omega in vitro; however, no effect on survival time or quality of life has been demonstrated. Additional study is needed to determine efficacy in vivo (23).
Other drugs that inhibit viral replication, including ribavirin, vidarabine, and nelfinavir, are not recommended, because they are toxic in cats.
Supportive Care
Treatment of FIP with corticosteroids (prednisolone at 2–4 mg/kg, PO, every 24 hours) or cyclophosphamide (2–4 mg/kg, PO, every 48 hours), alone or in combination, may result in temporary clinical improvement or slowed progression of disease. Use of chlorambucil has also been reported.
Thoracic effusions are usually associated with dyspnea and should be drained via thoracocentesis. Other than for sampling, the volume of abdominal effusion should be drained via abdominocentesis only if it is interfering with respiration; drained effusion fluid will rapidly reaccumulate.
Pearls & Pitfalls
|
Nonspecific supportive care for FIP includes fluid therapy, nutritional support, and ancillary treatments such as administration of vitamin B12. Ocular disease and other concurrent illness should be treated. Antimicrobials are indicated only for secondary bacterial infections.
Other Treatments
Additional treatments with some evidence of in vitro or in vivo efficacy against FIP include the following:
polyprenyl immunostimulant (24)
ozagrel hydrochloride (25)
feline TNF-alpha–neutralizing monoclonal antibodies (26)
human interferon alpha (29)
itraconazole (30)
Other potential treatments that have been suggested for FIP include small molecule inhibitors (eg, viroporins, chloroquine, mefloquine, hexamethylene amiloride) and small interfering RNAs (siRNAs) (31, 32, 33, 34).
Pentoxifylline or propentofylline are used to treat vasculitis; however, they have not been shown to be effective against FIP (35).
Prevention
The following measures can help prevent FIP in catteries and shelters:
antibody testing to limit new introductions to only FCoV-seronegative cats
adequate husbandry and environmental enrichment to minimize stress
adequate numbers of litter trays and thorough daily cleaning to minimize viral transmission via fecal contamination of the environment
Vaccination
An intranasal, modified live virus vaccine against FCoV is available; however, the risk-benefit profile remains unclear. The 2020 AAHA/AAFP Feline Vaccination Guidelines list the vaccine as not generally recommended. Previous vaccines were unsuccessful because of antibody-dependent enhancement.
Disinfection
FCoV particles are susceptible to inactivation by disinfectants (eg, dilute bleach), heat, lipid solvents, nonionic detergents, formaldehyde, oxidizing agents, and ultraviolet irradiation.
Prognosis of Feline Infectious Peritonitis
The prognosis for cats with FIP is poor without treatment. FIP has historically been considered a terminal diagnosis. Supportive care prolongs survival time; without specific antiviral treatment, however, FIP is fatal. With antiviral treatment, the prognosis, based on available case numbers thus far, appears to be fair to good.
Median survival time for FIP without treatment has been reported as 9 days (range, 3–200 days) (23).
Cats with effusive FIP usually survive for only days to weeks.
Cats with noneffusive FIP can survive longer (weeks to months).
Once neurological signs of FIP are apparent, death is generally imminent without treatment.
Key Points
Feline infectious peritonitis is a severe, immune-mediated coronaviral disease of cats.
There is no single, minimally invasive, antemortem diagnostic test for FIP.
Antiviral drugs offer hope for safe, effective treatment.
For More Information
Thayer V, Gogolski S, Felten S, Hartmann K, Kennedy M, Olah GA. 2022 AAFP/EveryCat feline infectious peritonitis diagnosis guidelines. J Feline Med Surg. 2022;24(9):905-933. doi:10.1177/1098612X221118761
European Advisory Board on Cat Diseases: Feline Coronavirus & Feline Infectious Peritonitis: ABCD Guideline With Literature Review.
Also see pet health content regarding feline infectious peritonitis.
References
Addie DD, Jarrett O. A study of naturally occurring feline coronavirus infections in kittens. Vet Rec. 1992;130(7):133-137. doi:10.1136/vr.130.7.133
Attipa C, Gunn-Moore D, Mazeri S, et al. Concerning feline infectious peritonitis outbreak in Cyprus. Vet Rec. 2023;192(11):449-450. doi:10.1002/vetr.3143
Weese S. Cyprus cat deaths. August 7, 2023. Worms & Germs Blog.
Pesteanu-Somogyi LD, Radzai C, Pressler BM. Prevalence of feline infectious peritonitis in specific cat breeds. J Feline Med Surg. 2006;8(1):1-5. doi:10.1016/j.jfms.2005.04.003
Riemer F, Kuehner KA, Ritz S, Sauter-Louis C, Hartmann K. Clinical and laboratory features of cats with feline infectious peritonitis—a retrospective study of 231 confirmed cases (2000–2010). J Feline Med Surg. 2016;18(4):348-356. doi:10.1177/1098612X15586209
Rohrbach BW, Legendre AM, Baldwin CA, Lein DH, Reed WM, Wilson RB. Epidemiology of feline infectious peritonitis among cats examined at veterinary medical teaching hospitals. J Am Vet Med Assoc. 2001;218(7):1111-1115. doi:10.2460/javma.2001.218.1111
Silva CS, Mullis LB. Human respiratory coronaviruses detected in patients with influenza-like illness in Arkansas, USA. Virol Mycol. 2014;(Suppl 2):004. doi:10.4172/2161-0517.S2-004
Vlasova AN, Diaz A, Damtie D, et al. Novel canine coronavirus isolated from a hospitalized patient with pneumonia in East Malaysia. Clin Infect Dis. 2022;74(3):446-454. doi:10.1093/cid/ciab456
Barker EN, Stranieri A, Helps CR, et al. Limitations of using feline coronavirus spike protein gene mutations to diagnose feline infectious peritonitis. Vet Res. 2017;48(1):60.doi:10.1186/s13567-017-0467-9
Felten S, Weider K, Doenges S, et al. Detection of feline coronavirus spike gene mutations as a tool to diagnose feline infectious peritonitis. J Feline Med Surg. 2017;19(4):321-335. doi:10.1177/1098612X15623824
Taylor SS, Coggins S, Barker EN, et al. Retrospective study and outcome of 307 cats with feline infectious peritonitis treated with legally sourced veterinary compounded preparations of remdesivir and GS-441524 (2020–2022). J Feline Med Surg. 2023;25(9):1098612X231194460. doi:10.1177/1098612X231194460
Pedersen NC, Perron M, Bannasch M, et al. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J Feline Med Surg. 2019;21(4):271-281. doi:10.1177/1098612X19825701
Murphy BG, Perron M, Murakami E, et al. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet Microbiol. 2018;219:226-233. doi:10.1016/j.vetmic.2018.04.026
Allinder M, Tynan B, Martin C, et al. Uroliths composed of antiviral compound GS-441524 in 2 cats undergoing treatment for feline infectious peritonitis. J Vet Intern Med. Published online November 30, 2023. doi:10.1111/jvim.16954
Kim Y, Liu H, Galasiti Kankanamalage AC, et al. Reversal of the progression of fatal coronavirus infection in cats by a broad-spectrum coronavirus protease inhibitor. PLoS Pathog. 2016;12(3):e1005531. doi:10.1371/journal.ppat.1005531
Kim Y, Shivanna V, Narayanan S, et al. Broad-spectrum inhibitors against 3C-like proteases of feline coronaviruses and feline caliciviruses. J Virol. 2015;89(9):4942-4950. doi:10.1128/JVI.03688-14
Kim Y, Mandadapu SR, Groutas WC, Chang KO. Potent inhibition of feline coronaviruses with peptidyl compounds targeting coronavirus 3C-like protease. Antiviral Res. 2013;97(2):161-168. doi:10.1016/j.antiviral.2012.11.005
Pedersen NC, Kim Y, Liu H, et al. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J Feline Med Surg. 2018;20(4):378-392. doi:10.1177/1098612X17729626
Roy M, Jacque N, Novicoff W, Li E, Negash R, Evans SJM. Unlicensed molnupiravir is an effective rescue treatment following failure of unlicensed GS-441524-like therapy for cats with suspected feline infectious peritonitis. Pathogens. 2022;11(10):1209. doi:10.3390/pathogens11101209
Evans SJM. Evaluation of unlicensed molnupiravir and GC376 as rescue therapy for cats with feline infectious peritonitis. In: 2022 International Society for Companion Animal Infectious Diseases Symposium Proceedings.
Sase O. Molnupiravir treatment of 18 cats with feline infectious peritonitis: a case series. J Vet Intern Med. 2023;37(5):1876-1880. doi:10.1111/jvim.16832
Cook S, Wittenburg L, Yan VC, et al. An optimized bioassay for screening combined anticoronaviral compounds for efficacy against feline infectious peritonitis virus with pharmacokinetic analyses of GS-441524, remdesivir, and molnupiravir in cats. Viruses. 2022;14(11):2429. doi:10.3390/v14112429
Ritz S, Egberink H, Hartmann K. Effect of feline interferon-omega on the survival time and quality of life of cats with feline infectious peritonitis. J Vet Intern Med. 2007;21(6):1193-1197. doi:10.1892/06-302.1
Legendre AM, Bartges JW. Effect of Polyprenyl Immunostimulant on the survival times of three cats with the dry form of feline infectious peritonitis. J Feline Med Surg. 2009;11(8):624-626. doi:10.1016/j.jfms.2008.12.002
Watari T, Kaneshima T, Tsujimoto H, Ono K, Hasegawa A. Effect of thromboxane synthetase inhibitor on feline infectious peritonitis in cats. J Vet Med Sci. 1998;60(5):657-659. doi:10.1292/jvms.60.657
Doki T, Takano T, Kawagoe K, Kito A, Hohdatsu T. Therapeutic effect of anti-feline TNF-alpha monoclonal antibody for feline infectious peritonitis. Res Vet Sci. 2016;104:17-23. doi:10.1016/j.rvsc.2015.11.005
Tanaka Y, Sato Y, Osawa S, Inoue M, Tanaka S, Sasaki T. Suppression of feline coronavirus replication in vitro by cyclosporin A. Vet Res. 2012;43(1):41. doi:10.1186/1297-9716-43-41
Tanaka Y, Sato Y, Takahashi D, Matsumoto H, Sasaki T. Treatment of a case of feline infectious peritonitis with cyclosporin A. Vet Rec. 2015;3(1):e000134. doi:10.1136/vetreccr-2014-000134
Weiss RC, Toivio-Kinnucan M. Inhibition of feline infectious peritonitis virus replication by recombinant human leukocyte (alpha) interferon and feline fibroblastic (beta) interferon. Am J Vet Res. 1988;49(8):1329-1335.
Doki T, Takahashi K, Hasegawa N, Takano T. In vitro antiviral effects of GS-441524 and itraconazole combination against feline infectious peritonitis virus. Res Vet Sci. 2022;144:27-33. doi:10.1016/j.rvsc.2022.01.005
Takano T, Nakano K, Doki T, Hohdatsu T. Differential effects of viroporin inhibitors against feline infectious peritonitis virus serotypes I and II. Arch Virol. 2015;160(5):1163-1170. doi:10.1007/s00705-015-2370-x
McDonagh P, Sheehy PA, Norris JM. Combination siRNA therapy against feline coronavirus can delay the emergence of antiviral resistance in vitro. Vet Microbiol. 2015;176(1-2):10-18. doi:10.1016/j.vetmic.2014.12.009
Anis EA, Wilkes RP, Kania SA, Legendre AM, Kennedy MA. Effect of small interfering RNAs on in vitro replication and gene expression of feline coronavirus. Am J Vet Res. 2014;75(9):828-834. doi:10.2460/ajvr.75.9.828
McDonagh P, Sheehy PA, Norris JM. Identification and characterisation of small molecule inhibitors of feline coronavirus replication. Vet Microbiol. 2014;174(3-4):438-447. doi:10.1016/j.vetmic.2014.10.030
Fischer Y, Ritz S, Weber K, Sauter-Louis C, Hartmann K. Randomized, placebo controlled study of the effect of propentofylline on survival time and quality of life of cats with feline infectious peritonitis. J Vet Intern Med. 2011;25(6):1270-1276. doi:10.1111/j.1939-1676.2011.00806.x




