




Lyme borreliosis is a vector-borne zoonotic disease transmitted by ticks infected with spirochetal bacteria belonging to the genus Borrelia. Affected dogs typically present with intermittent, lameness, fever, inappetance, lethargy, and focal lymphadenopathy. Although infrequently reported, clinical manifestations in horses include neurologic abnormalities, uveitis, and cutaneous lymphoma. Diagnosis is based on a combination of history, clinical signs, laboratory findings, exclusion of other diseases, and response to treatment. Treatment consists of an extended (eg, 30-day) course of antibiotics, supportive measures including analgesia, and immunosuppressive therapy in the case of autoimmune reaction.
Lyme borreliosis is a bacterial, tick-transmitted disease of animals (dogs, horses, possibly cats) and people. Many additional mammalian and avian species become infected but do not develop overt clinical signs. This disease is endemic to temperate areas in the northern hemisphere and is seen sporadically in Europe and Asia. Within the USA, endemic areas include the Northeast (particularly the New England states), the upper Midwest, and the Pacific coast. Globally, the incidence of Lyme borreliosis is increasing due to the expanding geographic range of tick vectors.
Diagnosis can be challenging, because most animals do not develop clinical illness after infection. Clinical signs of Lyme borreliosis have been well documented in dogs, in which the characteristic presentation includes an intermittent, shifting lameness. Horses with Lyme borreliosis may exhibit neurologic signs, uveitis, or cutaneous lymphoma. Although other clinical signs such as lameness have been reported in horses, they have yet to be conclusively linked to infection. Along with prevention, early diagnosis and treatment with antibiotics appear to be important to treatment success.
Etiology and Transmission of Lyme Borreliosis in Animals
Lyme borreliosis is caused by infection with spirochetal bacteria belonging to the Borrelia burgdorferi sensu lato species complex. Within this complex, the following spirochete species are well-established causes of Lyme borreliosis in people: B burgdorferi sensu stricto (North America, Europe), B mayonii (North America), B afzelii (Europe, Asia), B bavariensis (Europe, Asia), and B garinii (Europe, Asia). The predominant species responsible for Lyme borreliosis in animals is B burgdorferi sensu stricto (henceforth B burgdorferi). It is unclear whether other Borrelia species within the sensu lato complex can cause Lyme borreliosis in animals. Tick vectors of B burgdorferi sensu lato are hard-shelled Ixodes ticks. In the USA, I scapularis (colloquially known as the deer tick) is the predominant vector in the Northeast and Midwest, whereas I pacificus is the predominant vector on the Pacific coast. In Europe and Asia, I ricinus and I persulcatus are the primary vectors.

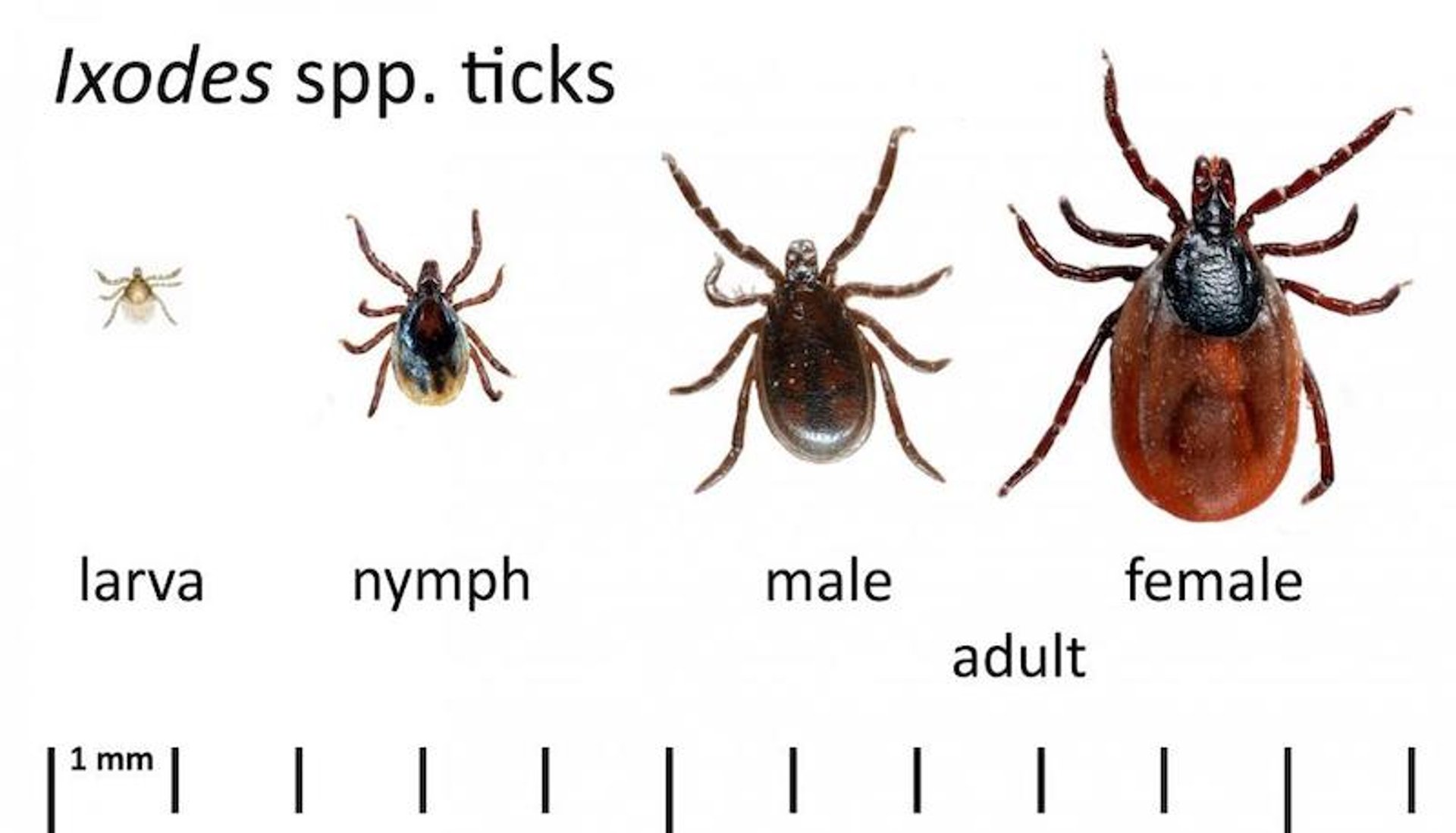
Courtesy of Dr. Reinhard K. Straubinger.
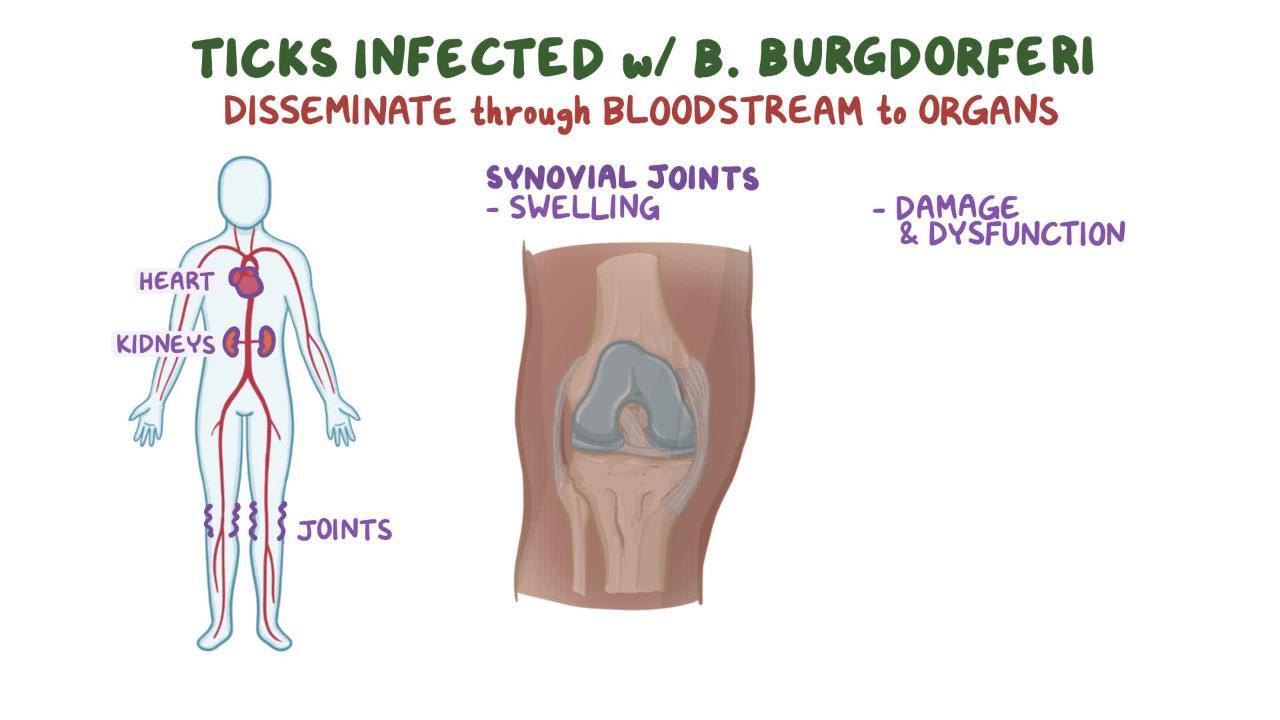
Ticks become infected with spirochetes on having a blood meal from a Borrelia-carrying host. A variety of wildlife species act as reservoir hosts for B burgdorferi. Rodents in particular are a major reservoir for Borrelia species. Infection rates of the vectors vary according to region and season and can be as high as 50% in adult ticks. Transmission is most likely to occur during warmer months of the year, when ticks are most active. However, transmission is also possible during the winter, because ticks may be active as long as temperatures are >4°C (40°F). After tick attachment, at least 24 hours are required for the transmission of spirochetes from the infected tick into the host, and transmission usually occurs 36–48 hours into the blood meal. Early removal of attached ticks, therefore, reduces the likelihood of spirochete transmission. B burgdorferi sensu lato organisms are not transmitted by insects, bodily fluids (urine, saliva, semen), or bite wounds. Experimental studies have shown that dams infected before gestation may transmit spirochetes to their pups in utero.
Clinical Findings of Lyme Borreliosis in Animals
Numerous clinical syndromes have been attributed to Lyme borreliosis in domestic animals, including limb and joint disease, as well as renal, neurologic, and cardiac abnormalities. However, the clinical syndromes seen in different animal species vary considerably. Certain clinical signs of Lyme borreliosis are well documented in horses and dogs.
Although cats can become infected with B burgdorferi and mount an antibody response, it is unknown whether they develop subsequent clinical disease.
In dogs, the most common clinical signs are intermittent, shifting lameness, fever, anorexia, lethargy, and lymphadenopathy with or without swollen, painful joints.
Additionally, a renal syndrome has been attributed to B burgdorferi infection in dogs, though a causal relationship has yet to be established. This renal syndrome is characterized by uremia, hyperphosphatemia, and severe protein-losing nephropathy, often accompanied by peripheral edema. It is thought to be immune-mediated, and dogs typically present with either acute or chronic kidney failure, with or without additional cardiac or neurologic signs (eg, blindness, hypertension, heart murmurs, thromboembolic events).
In horses, well-documented clinical signs of Lyme borreliosis include neuroborreliosis, uveitis, and cutaneous lymphoma. Horses with neuroborreliosis may exhibit any of the following clinical signs: atrophy of spinal muscles, dysphagia, laryngeal dysfunction, facial paresis, spinal cord ataxia and paresis, behavioral changes, and hyperesthesia. Horses with neuroborreliosis may also exhibit clinical signs common to other neurologic disorders (eg, meningitis, cranial nerve dysfunction). Other clinical signs in horses, such as intermittent, shifting lameness, have not been conclusively linked to Lyme borreliosis.
Most seropositive dogs and horses are asymptomatic. This stands in contrast to people, in whom infection with B burgdorferi causes illness in an estimated 90% of people. Soon after infection via a tick bite, most individuals develop a characteristic bull's-eye rash (erythema migrans) at the site of infection, and some experience flu-like symptoms. Common signs and symptoms of Lyme borreliosis in people include arthritis with severe joint pain and swelling, facial paralysis, dizziness, heart palpitations, nerve pain, and severe headaches.
Diagnosis of Lyme Borreliosis in Animals
Based on a combination of history, clinical signs, laboratory data, response to therapy, and exclusion of other diseases
Serology is important, but positive results have a low positive predictive value of clinical disease
Culture and PCR do not reliably detect spirochetes
Cytology and histopathology of affected tissues may show characteristic inflammatory changes
A diagnosis of Lyme borreliosis is generally reached through the exclusion of other diseases, in tandem with a history of exposure to ticks, clinical signs, supporting laboratory data, and response to therapy. Because clinical signs are nonspecific, other diseases may mimic the signs of Lyme borreliosis. Moreover, most infected animals are asymptomatic, so a positive test result for B burgdorferi has a low positive predictive value for clinical disease. In other words, a positive test neither demonstrates that current clinical signs are caused by infection with B burgdorferi, nor suggests that the animal is likely to develop clinical illness in the future. Thus, a positive test result in a clinically ill animal may be an incidental finding.
A number of infectious agents may be transmitted by ticks (eg, Ehrlichia, Anaplasma, Babesia, Rickettsia), some of which can cause clinical signs similar to those of Lyme borreliosis. Thus, infection with these agents, or mixed infections with B burgdorferi, should be considered. Anaplasma phagocytophilum, for example, is also transmitted by Ixodes ticks and can cause clinical signs resembling those of Lyme borreliosis in dogs and horses. In addition to excluding infectious causes, orthopedic disorders (eg, trauma, immune-mediated diseases) should be excluded as well.
Autoimmune panels, CBC, serum chemistry, radiographs, and other laboratory data are generally normal, except for results pertaining directly to the affected system (eg, soft-tissue swelling in limbs, neutrophil accumulation in synovial fluids of affected joints). Serologic testing for antibodies specific for B burgdorferi sensu lato is an adjunct to clinical diagnosis. Antibodies can be detected with ELISA (which test for C6 peptide) and with multiplex fluorescence assays. Because of possible cross-reactions with other spirochetal infections, the following serologic testing methods are no longer recommended: whole cell ELISA, immunofluorescent antibody assays, and Western blot.
The standard procedure for antibody detection is a two-tiered approach in which samples are screened with a sensitive rapid assay (ELISA or multiplex fluorescence) and only positively reacting samples are rechecked with specific confirmatory tests. Although quantitative antibody assays are available to test for C6, titer magnitude is a poor predictor of current or future illness.
Some vaccines can interfere with serologic tests, in particular, those that stimulate production of OspC (outer surface protein C) antibodies. Antibodies against C6 peptide, VlsE (variable major protein-like sequence, expressed), and OspF (outer surface protein F) indicate natural exposure, because these antigens are not contained in any vaccines. False-negative serologic results may occur in the case of an acute infection (< 1 month), infection of an immune-privileged site (eg, eye), or an abnormal host response (ie, immunodeficiency). In particular, horses with neuroborreliosis are often found to be seronegative.
Isolation of B burgdorferi sensu lato by culture or detection of specific DNA by PCR from joints, skin tissue samples, or other affected tissues may also help in diagnosis. Direct detection of the organism, however, is difficult and time-consuming (up to 6 weeks for culture) and yields negative results in most cases. Blood samples are generally negative, because the organism resides in tissue and not in the circulation. Characteristic inflammatory changes seen in histologic or cytologic samples of affected tissues may also be used to support a diagnosis.
Treatment of Lyme Borreliosis in Animals
A long course of antibiotics (4 weeks) is indicated to treat infection in clinically ill animals
Symptomatic therapy should be directed toward the affected organ system and toward pain management
Immunosuppressive therapy is indicated in the case of infection-related autoimmune reactions
Some animals may remain seropositive after successful treatment
Antibiotic therapy is indicated in all animals with clinical signs attributed to Lyme borreliosis. Treatment of healthy seropositive animals is problematic because of the inability to monitor response to treatment and the potential for adverse drug effects. Antimicrobials in the tetracycline and beta-lactam families have been shown to be effective in treating Lyme borreliosis in dogs and horses. A long course of antibiotics (4 weeks) is indicated. Chronic infection in dogs and horses is not well documented, so the utility or efficacy of treatment beyond 4 weeks is unknown. Symptomatic therapy directed toward the affected organ system and clinicopathologic abnormalities is also important.
In dogs, doxycycline (10 mg/kg, PO, every 12 hours) and amoxicillin (20 mg/kg, PO, every 8 hours) are effective, and a rapid response (1–3 days) to treatment is seen in most cases, although incomplete or transient resolution of signs occurs in a significant number of affected animals. Doxycycline is preferred over penicillins because mixed infections with other tick-borne pathogens are often found in animals with clinical signs. Symptomatic treatment for neuropathic pain may be indicated, in which case gabapentin is the recommended therapy; NSAIDs are less preferable because a wash-out period is required if the animal subsequently develops immune-mediated disease and requires immunosuppressive therapy. In dogs with kidney failure that is suspected to be related to Borrelia infection, supportive therapy is indicated, and immunosuppressive agents such as mycophenolate may be required for severe, rapidly progressing cases.
In horses, a number of tetracycline (administered orally and parenterally) and beta-lactam (administered parenterally) antibiotics have been successful in treating Lyme borreliosis. Treatment is more challenging in horses because of the poor bioavailability of antibiotics and because horses are often diagnosed long after they have been infected. Four-week courses of doxycycline (10 mg/kg, PO, twice a day) or minocycline (4 mg/kg, PO, twice a day) have reportedly been successful in treating Lyme borreliosis in horses. Although beta-lactams may be less practical because of parenteral administration and carry a risk of toxicity, they are preferable for treatment of neuroborreliosis. In these cases, parenteral high-dose penicillin (44,000 U/kg, IV, every 4–6 hours) or cefotaxime (25–50 mg/kg, IV, every 6–8 hours) may be useful. Certain antimicrobials (eg, ceftriaxone) have resulted in a high incidence of adverse effects in horses and should not be used.
Quantitative C6 antibody assays are sometimes performed before and after treatment to monitor response to therapy, although titers do not always decrease after treatment, and some animals remain seropositive. Successful treatment is therefore focused on the resolution of clinical signs rather than serologic data. An increased titer after treatment may represent a relapse or reinfection.
Control and Prevention of Lyme Borreliosis in Animals

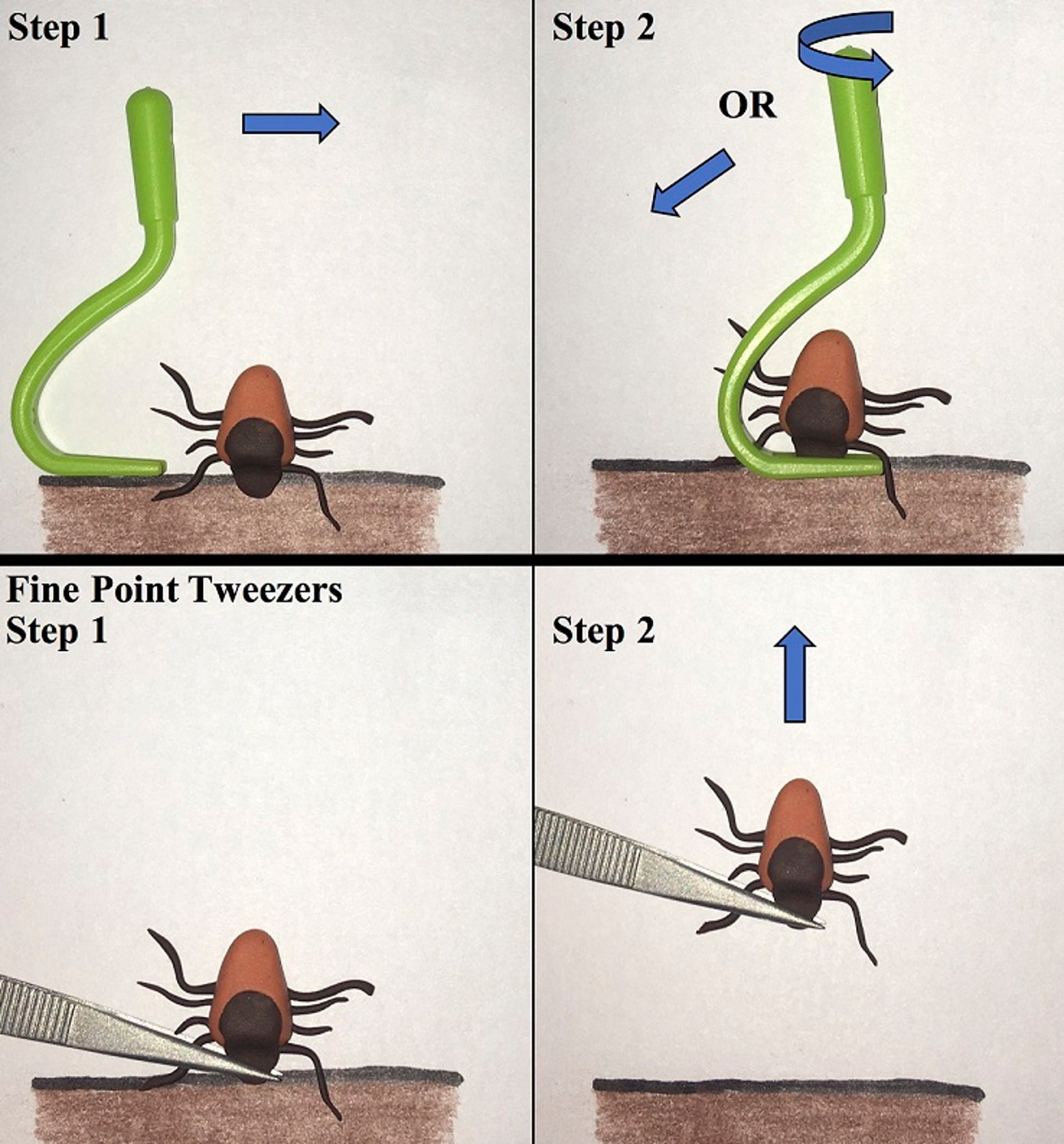
Courtesy of Dr. Nadine A. Vogt.
Tick avoidance plays an important role in the control of Lyme borreliosis. A number of effective repellents and acaricides in collars, sprays, and spot-ons are available for use in dogs. Tick checks and prompt removal of ticks can reduce the likelihood of transmission, because at least 24 hours are required for transmission of spirochetes from tick to host. Ticks must be removed carefully. If the tick mouth parts are damaged and left in the animal, transmission of spirochetes may still occur, even after the tick has been removed.
A number of bacterin and recombinant vaccines are also licensed for use in dogs. Reported efficacies are variable (50%–100%), and evaluation of efficacy is challenging because of the lack of a disease model. The duration of immunity is 1 year. Dogs that have been exposed to ticks should be tested serologically for established infection before vaccination. Postinfection vaccination has little to no therapeutic effect on established infections.
Zoonotic Risk of Lyme Borreliosis in Animals
Lyme borreliosis is a vector-borne zoonotic disease. Ticks transmit spirochetes from wildlife reservoirs to people. Companion and farm animals are not a reservoir, though they may harbor unattached infected ticks that can subsequently attach to a person and transmit spirochetes.
Key Points
Lyme borreliosis is a bacterial, tick-transmitted disease of animals (dogs, horses, possibly cats) and people.
Transmission of Borrelia burgdorferi occurs during the blood meal of Ixodes spp ticks, and ticks may be active anytime temperatures are >4°C (40°F).
Dogs typically present with intermittent, shifting lameness, whereas horses may present with neurologic signs and/or uveitis.
Diagnosis is based on a combination of history of tick exposure, clinical signs, laboratory data, response to therapy, and exclusion of other diseases.
Clinically ill animals should be treated with a long course (4 weeks) of antibiotics (eg, doxycycline), and symptomatic therapy is used to manage pain and other conditions. Immunosuppressive therapy may be needed if an autoimmune reaction occurs.
The following preventive measures are available to reduce the risk of Lyme borreliosis: tick avoidance, prompt removal of ticks, acaricides, and vaccines.
In terms of zoonotic risk, companion and farm animals are not a direct source of infection but may harbor unattached infected ticks that can attach to people.
For More Information
University of Rhode Island: Tick identification guide
Centers for Disease Control: Lyme disease information
Also see pet health content regarding Lyme borreliosis in dogs, cats, and horses.




