




Ceruminous gland tumors are discussed in Tumors of the Ear Canal.
Benign, Nonvirus-associated Papillomatous Lesions
For a discussion of papillomas (viral warts), the most common, viral-induced neoplasms of the skin, see Papillomas. Benign, proliferative lesions not associated with papilloma virus infection can have a gross morphology similar to that of papillomas.
Epidermal hamartomas (nevi) are rare proliferations identified only in dogs, most often in the young. The disease may be heritable in Cocker Spaniels. Grossly, epidermal nevi appear as pigmented, hyperkeratotic, vaguely papillated papules and plaques that are occasionally arranged in a linear pattern. Some forms are associated with pustules and acantholytic cells. They are benign; however, their appearance is unpleasant, and the extensive hyperkeratosis is prone to secondary bacterial infection. Localized lesions can be excised; dogs with multiple lesions or lesions too large to be surgically removed may be responsive to isotretinoin or etretinate. Hyperkeratosis may be transiently controlled by use of topical keratolytic shampoos and emollients.
Congenital papillomas of foals are rare and probably a developmental defect rather than a result of papilloma virus infection. They are found anywhere on the body but most commonly on the head. Thoroughbreds may be predisposed. Present at birth, the lesions are often several centimeters in diameter, hairless, pedunculated, and exophytic, with a papillated surface reminiscent of a cauliflower. They are benign, and excision is curative.
Canine warty dyskeratomas are rare, benign neoplasms of uncertain derivation but with histologic features of follicular or apocrine neoplasms (or both). They appear grossly as verrucous papules or nodules with a keratotic, umbilicated center. Excision is curative.
Basal Cell Tumors and Basal Cell Carcinomas
Basal cell tumors represent a heterogeneous group of cutaneous epithelial neoplasms recognized most commonly in cats, less commonly in dogs, occasionally in horses and sheep, and seldom in other domestic animals. These neoplasms are composed of a proliferation of small basophilic cells that exhibit morphology reminiscent of the progenitor cells of the epidermis and adnexa. As these tumors have been examined more closely, evidence of differentiation (follicular, sebaceous, etc) has been discovered, giving justification for reclassification. For example, in dogs, what in the past was called a basal cell tumor is best characterized as a trichoblastoma, a tumor of hair bulb (the site of the follicle that produces the hair shaft) origin.
Some reclassification schemes have suggested that the use of the term basal cell tumor be restricted to a benign neoplasm in cats (the derivation of which has yet to be defined). Because this revised terminology is being adopted slowly, traditional terminology will be used herein. That is, a benign proliferation of basal cells will be called a basal cell tumor; a malignant proliferation will be called a basal cell carcinoma. In domestic animals, most basal cell tumors are benign and originate in the mid to deep dermis, indicating probable adnexal derivation. These features distinguish basal cell tumors in domestic animals from those in people, the latter being locally invasive (ie, they are true carcinomas) and originating in the epidermis. In addition, solar injury is a common cause of neoplasms derived from basal cells in people, but its role in inducing basal cell tumors of other animals is unknown.
Canine basal cell tumors generally develop in middle-aged to older dogs of predisposed breeds such as Wirehaired Pointing Griffons, Kerry Blue Terriers, and Wheaten Terriers. These tumors are found most commonly on the head (especially the ears), the neck, and forelimbs. Older domestic longhair, Himalayan, and Persian cats are the breeds most at risk. Feline basal cell tumors may develop almost anywhere on the body. In both dogs and cats, these tumors generally appear as firm, solitary, encapsulated, and often hairless or ulcerated nodules that may be pedunculated; they vary in size from < 1 cm to >10 cm in diameter. In cats more often than dogs, these tumors are often densely pigmented, and on cut section they can be difficult to distinguish from dermal melanocytomas. Cystic variants are also more common in cats. Although basal cell tumors are benign, they are expansive neoplasms and may be associated with extensive ulceration and secondary inflammation. Complete excision is curative.


Courtesy of Dr. Alice Villalobos.
Basal cell carcinomas are more frequently recognized in senior cats than in dogs. Persian-type breeds are predisposed. They often appear as ulcerated plaques on the head, extremities, or neck. Unlike benign basal cell tumors, these carcinomas generally have continuity with the epidermis, are locally invasive, and may be multicentric. Although evidence of vascular invasion may be identified on histologic sections, local or systemic metastasis rarely occurs. Consequently, surgical excision is the treatment of choice.
In dogs, most basal cell carcinomas have histologic evidence of cornification, a feature they have in common with squamous cell carcinomas. Therefore, they are generally called basosquamous cell carcinomas. These tumors are generally recognized in older dogs. Saint Bernards, Scottish Terriers, and Norwegian Elkhounds are most at risk. Unlike canine basal cell tumors, basosquamous cell carcinomas do not tend to develop on the head and can be found almost anywhere on the body where they have continuity with the epidermis and appear as exoendophytic nodules or plaques. These tumors are locally invasive but seldom metastasize. Surgical excision is the treatment of choice.
Intracutaneous Cornifying Epitheliomas


Courtesy of Dr. Alice Villalobos.
Intracutaneous cornifying epitheliomas are benign neoplasms of dogs and possibly cats. As in human keratoacanthomas, these lesions most likely arise from the hair follicle and not from the interfollicular epidermis. They can develop anywhere on the body, with the back, tail, and extremities the most common sites affecting middle-aged dogs. Norwegian Elkhounds, Belgian Sheepdogs, Lhasa Apsos, and Bearded Collies are most likely to develop these tumors, with Norwegian Elkhounds and Lhasa Apsos at risk of developing generalized lesions.
The most characteristic presentation is a papule or nodule with a central cornified pore that may protrude above the epidermal surface, giving the appearance of a horn; however, many of these tumors never have continuity with the epidermis and may appear solely as cornified cysts. These tumors are benign, and treatment is optional, provided a definitive diagnosis has been established and there is no self-trauma, ulceration, or secondary infection. Tumor wall rupture releases keratin into surrounding tissues, evoking a pyogranulomatous and granulomatous inflammatory response. Excision is curative; however, dogs are prone to develop additional tumors over time. For animals with a generalized form of the disease, oral retinoids (eg, isotretinoin or etretinate) may be of therapeutic benefit.
Squamous Cell Carcinomas
Thought to arise from either the epidermis or the epithelium of the superficial (infundibular) regions of the outer root sheath of the hair follicle, squamous cell carcinomas have been recognized in all domestic animals. Although most arise without prior cause, in many species, especially in the face and ear tips of white cats and in the ventral nonpigmented skin of dogs, prolonged exposure to sunlight on sparsely haired, minimally pigmented areas of the body is a major predisposing factor. The grooming habits of cats also expose them to particulate carcinogens from cigarette smoke and flea collars. In addition, a unique form of feline squamous cell carcinoma associated with papilloma virus infection has been described.


Courtesy of Dr. Alice Villalobos.


Courtesy of Dr. Alice Villalobos.
In dogs, squamous cell carcinomas are the most frequently diagnosed carcinomas arising in the skin. Two forms are recognized: cutaneous and subungual.
Cutaneous squamous cell carcinomas are tumors of older dogs, with Bloodhounds, Basset Hounds, and Standard Poodles at greatest risk. Lesions commonly arise on the head, distal aspects of the extremities, ventral abdomen, and perineum. Most cutaneous squamous cell carcinomas appear as firm, raised, frequently ulcerated plaques and nodules; sometimes they can be extremely exophytic and have a wart-like surface. The etiology of most of these tumors is undefined; however, some are induced by prolonged solar injury. These usually develop on ventral abdominal, preputial, scrotal, and inguinal skin in white-skinned, shorthaired breeds such as Dalmatians, Bull Terriers, Pit Bulls, and Beagles. Lesions develop in a ventral location because the poorly haired skin has minimal shielding from ultraviolet radiation, many animals sun themselves lying on their backs, and perhaps because solar radiation reflects from the ground. Before a carcinoma develops, animals acquire focal zones of lichenification, hyperkeratosis, and erythema known as solar keratosis (solar dermatosis, actinic keratosis, senile keratosis).
Subungual squamous cell carcinomas are most commonly found in older Giant Schnauzers, Standard Schnauzers, Gordon Setters, Briards, Kerry Blue Terriers, Standard Poodles, and Scottish Terriers. Generally, all are dark-haired breeds, and a dark coat color has been associated with development of subungual squamous cell carcinomas that arise from the nailbed epithelium and invade the medullary and cortical bone of the third phalanx (P3). They may arise on multiple digits, often appear on different extremities, and may metastasize via lymphatics to regional lymph nodes and lungs in as many as 13% of cases. Females have a slight predilection, and both fore- and hind limbs are equally predisposed to tumor development.

Courtesy of Dr. Alice Villalobos.


Courtesy of Dr. Alice Villalobos.


Courtesy of Dr. Alice Villalobos.


Courtesy of Dr. Alice Villalobos.


Courtesy of Dr. Alice Villalobos.
In cats, cutaneous squamous cell carcinomas most commonly develop in conjunction with chronic solar injury. Consequently, they usually develop on the pinnae, frontal ridges, eyelids, nose, or lips of cats that have white skin in these regions. There is no breed or sex predilection. As in dogs, solar keratosis or carcinoma in situ (early superficial stage) often precedes development of a malignant tumor. Coat-associated particulate carcinogens from exposure to cigarette smoke and flea collars have been identified as risk factors for cats with oral squamous cell carcinoma. Lesions not caused by sun exposure may develop on the digits and are presumed to be metastatic from primary squamous cell carcinomas of the lung, but primary subungual forms are uncommon in cats.
Cutaneous squamous cell carcinomas are the most common malignant neoplasm in horses. They generally develop in adult or senior horses with white or part-white coats; breeds at risk include Appaloosa, Belgian, American Paint, and Pinto. Although they can arise anywhere on the body, these tumors most commonly arise in nonpigmented, poorly haired areas near mucous membranes. Thus, the periorbital regions, lips, nose, anus, and external genitalia (especially the penile sheath) are sites most likely to be affected.

Courtesy of Dr. Sameeh M. Abutarbush.
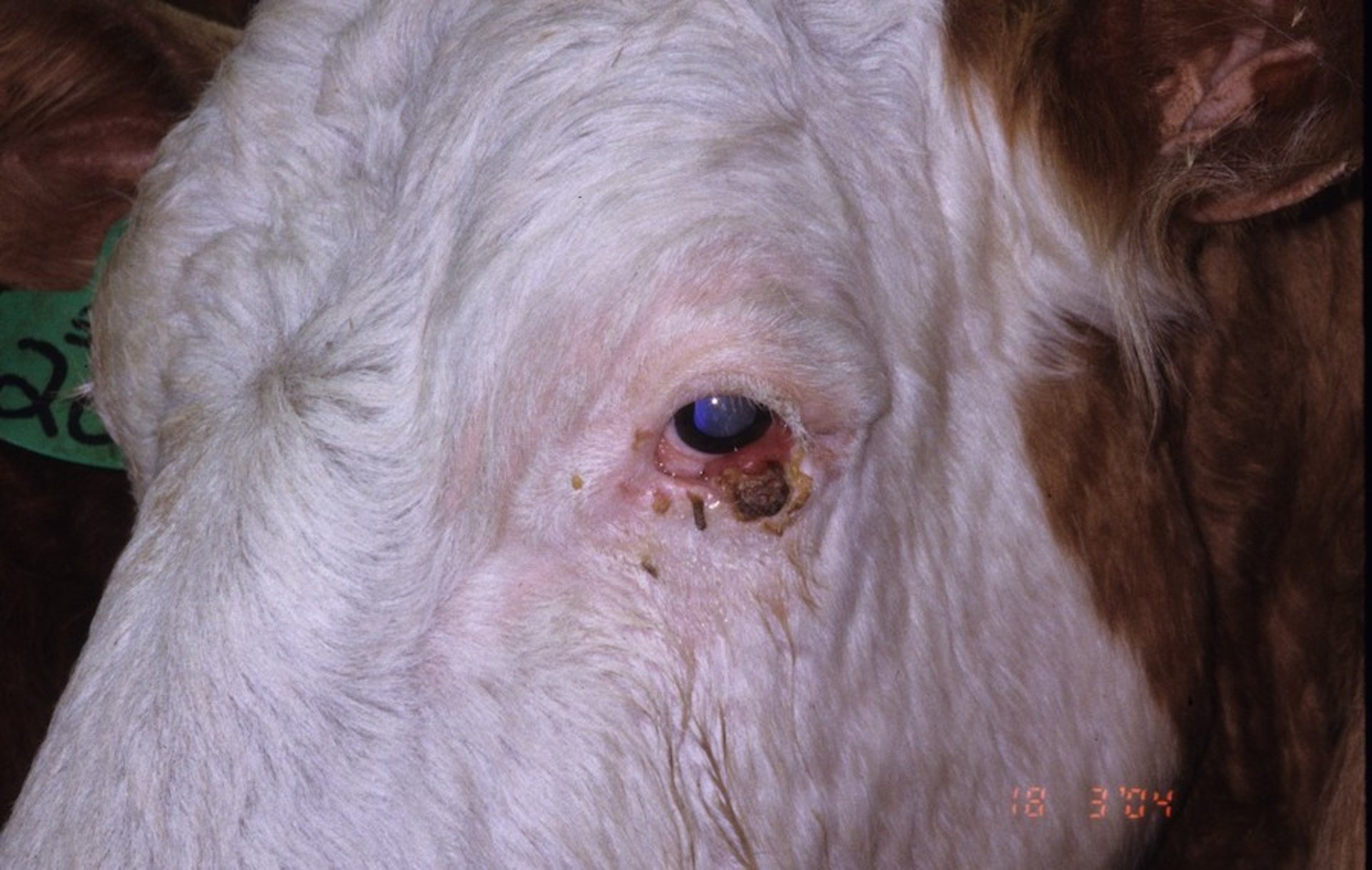
In cattle, squamous cell carcinomas are most common in breeds with white hair and poorly pigmented skin (especially Holsteins and Ayrshires) and, as in horses, develop around the mucous membranes, usually at the mucocutaneous junctions, particularly the periocular and vulvar regions. In India, squamous cell carcinomas of the horn core are common in older bulls. The most common cause is actinic injury. Solar keratoses often precede development of an invasive tumor; genetic factors, immunodeficiency, and viruses may also play a role.
In sheep, squamous cell carcinomas are of economic significance in some parts of the world. In a study in Australia, they were responsible for more than one-third of all condemnations before slaughter. The Merino breed is most at risk, and females more so than males. The most common sites are the poorly haired skin of the ears, lips, muzzle, and the vulvar lips after they have been externalized by a Mules operation to prevent fly strike. Tumors at these sites develop in conjunction with solar injury, which is heightened when animals ingest photosensitizing plants. Tumors of the ears also develop more frequently after a procedure such as ear tagging. Squamous cell carcinomas can develop from follicular cysts on sites not commonly exposed to sunlight.
In goats, squamous cell carcinomas develop most frequently in females, in which tumors develop on the perineal and vulvar regions and on the skin of the teats and udders. Both males and females can develop sun-induced tumors on the ears. Although Angoras are most at risk, Saanen goats occasionally develop squamous cell carcinomas on the udder in association with papillomas. The role papilloma viruses play in tumor progression is considered contributory.
Squamous cell carcinomas are extremely uncommon in swine.

Courtesy of Dr. Alice Villalobos.
Most squamous cell carcinomas are solitary lesions; however, multiple tumors may develop in conjunction with solar injury in the field cancerization model. They appear as endophytic or exoendophytic lesions, the former as raised, irregular dermal masses with an ulcerated surface, and the latter as raised, irregular dermal masses covered by a papillated epidermis. Cats initially exhibit small, crusting facial sores that do not heal. The lesions often persist for months before defects appear on the ear tips, nares, and eyelids. Subungual squamous cell carcinomas of dogs are first identified by lameness or nail malformation, an infection that mimics chronic osteomyelitis, or loss of the claw of the affected digit. In cattle with involvement of the horn, the first sign is distorted growth.
Squamous cell carcinomas are characteristically invasive into adjacent soft and bony tissues. Infrequently, in cattle, they regress spontaneously. In small animals, long-term survival and the likelihood of metastasis are correlated with histologic differentiation. Well-differentiated tumors are slowly progressive or remain localized; undifferentiated tumors are more likely to metastasize or recur within 20 weeks following excision. In general, failure of treatment is due to late diagnosis and lack of control of local disease rather than metastasis.
For dogs and cats, surgical excision, such as excision of lesions or amputation of the involved digit or pinnae, is the treatment of choice, and margins of at least 2 cm are recommended. One review of 117 digit masses in dogs found that 25% of the lesions were squamous cell carcinomas and 66% were subungual lesions. These dogs had a 95% 1-year survival rate after amputation; however, if the lesion originated in other parts of the digit, 1-year survival rate was 60%. Excision may be combined with radiation or chemotherapy.
Feline squamous cell carcinomas are more radiosensitive than their canine counterparts. Still, the 1-year survival rate is < 10% for invasive neoplasms. Electroporation, cryosurgery, and hyperthermia therapy can be very helpful for local therapy especially in early (carcinoma in situ) lesions, but controlled studies have not been done to determine their effectiveness. Intralesional implant chemotherapy with 5-fluorouracil (dogs only), cisplatin (dogs only), or carboplatin along with retinoids and photodynamic therapy has been used with variable success.
Nosectomy may resolve superficial nasal lesions. Intratumoral injection of nasal planum squamous cell carcinomas in cats using carboplatin in a water-sesame seed oil emulsion resulted in a 70% general response with 1-year progression-free survival rate of ~50%. In dogs with multiple ventral actinic keratoses, topical dinitrochlorbenzene or 5-fluorouracil (5%) may be of benefit. Cats should not be given any form of 5-fluorouracil therapy. The use of topical immunomodulating antineoplastics such as imiquimod cream applied topically on lesions twice daily for 2 weeks creates a local application site inflammatory reaction and often resolves lesions. Imiquimod stimulates Toll-like receptor 7 and dendritic cells, modifying immune responses to destroy the targeted carcinoma cells. The response may be enhanced by the application of 6 joules of cold laser therapy to the lesions every 2 weeks until regression.
Limiting exposure to ultraviolet radiation helps to prevent solar-induced squamous cell carcinomas in dogs and cats. This may be accomplished by using UV window screens, sunscreen, and keeping companion animals indoors during hours of peak sunlight between 10:00 AM and 2:00 PM. Tattoos, magic markers, and sunscreen are used with variable success.
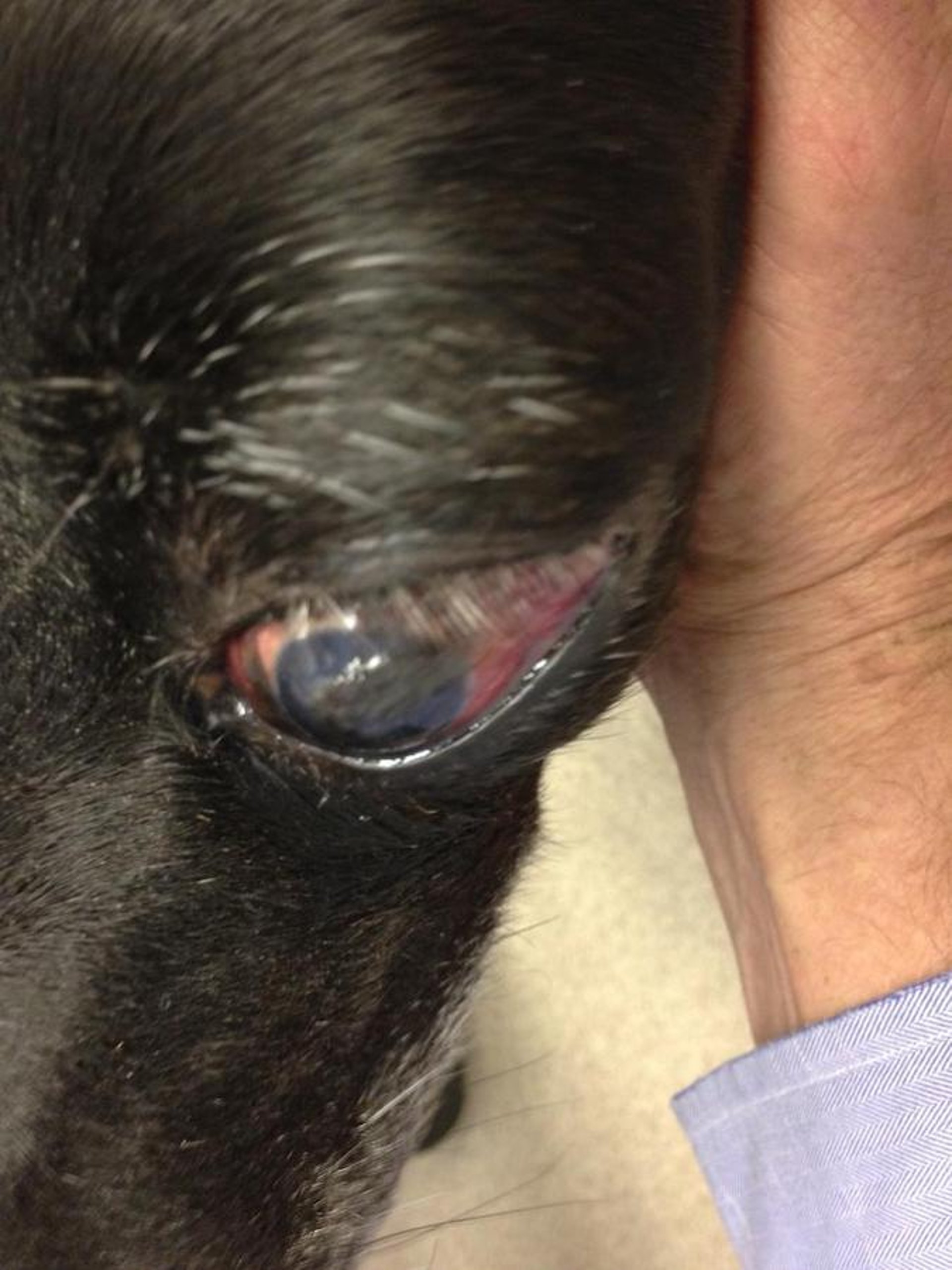
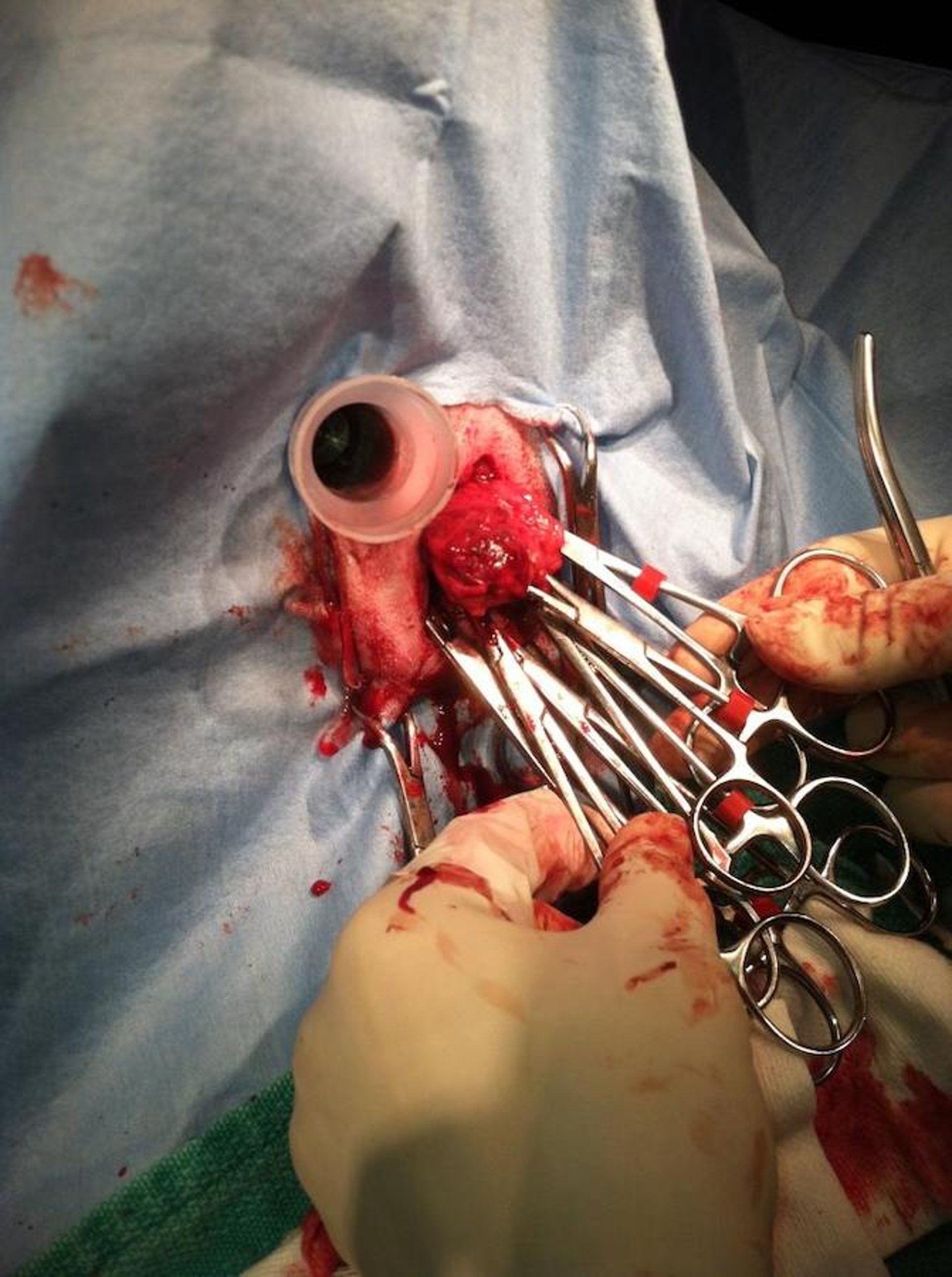
In horses, radiotherapy using surface or interstitial brachytherapy is the treatment of choice for squamous cell carcinomas. Other options include 90Sr or 192Ir implants, wide surgical excision (especially for neoplasms of the third eyelid, penis, and prepuce), and cryosurgery. Immunotherapy, with either an autogenous vaccine made from the patient's own tumor tissue suspended in Freund’s adjuvant, or nonspecific immunomodulation using Corynebacterium parvum, has had some success in treating ocular or horn core squamous cell carcinomas in cattle.

Courtesy of Dr. Alice Villalobos.
Feline multicentric squamous cell carcinoma in situ (feline Bowen disease) is a disease of cats >10 years of age and may be associated with immunosuppression. There is no defined breed or sex predilection. Clinically, lesions appear as multiple discrete, erythematous, black or brown hyperkeratotic plaques and papules. Lesions are nonpruritic, and ulceration is uncommon. Their development is associated with the presence of a papilloma virus. The term in situ refers to a malignant proliferation of epidermal and follicular outer sheath cells that are not invasive into the underlying dermis. Unfortunately, lesions may progress over time into an invasive carcinoma. Metastasis is extremely uncommon. These lesions usually develop in systemically ill or immunosuppressed cats and are believed to be virally induced. They have not been amenable to therapy; however, cryotherapy or electroporation of local lesions and topical imiquimod as described above may increase time to progression.
Keratinized Cutaneous Cysts
Most keratinized cutaneous cysts are malformations of the hair follicle. They are common in dogs; occasionally identified in cats, horses, goats, and sheep; and rare in cattle and pigs. Excision is the treatment of choice. Vigorous squeezing of these lesions is contraindicated because it often incites a severe foreign body inflammatory response due to the release of keratin into surrounding tissues.
Infundibular follicular cysts (epidermoid cysts, epidermal inclusion cysts, erroneously called sebaceous cysts) are the most common. They are a cystic dilatation of the upper portion of the outer sheath of the hair follicle (the infundibulum) lined by a layer of stratified cornifying epithelial cells indistinguishable from the epidermis. These cysts vary in size from 2 mm to >5 cm (lesions < 5 mm in diameter are often called milia). The only domestic animals identified at risk are Merino sheep, in which these cysts are often multiple and may progress to squamous cell carcinomas. As with all follicular cysts, these are usually solitary, papular to nodular lesions that are freely movable. They are generally partially compressible on palpation and occasionally have a small opening through the epidermis from which the cystic contents can be extruded. On cut surface, they are filled with a gray, brown, or yellowish, granular, caseous material that is lumenal keratin.
Isthmus catagen cysts (trichilemmal cysts, pilar cysts, cystic intracutaneous cornifying epithelioma) are follicular cysts that have the keratinization pattern of the lower portion of the outer root sheath. They have been definitively identified only in dogs and (rarely) in cats.
Matrix cysts are follicular cysts in which the wall resembles the epithelium of the hair bulb (the matrix portion of the hair follicle) and the inner root sheath. They occur predominantly in dogs and cats. Many progress to pilomatricomas.
Hybrid cysts (panfollicular cysts) are follicular cysts that have a combination of the characteristics of epidermal inclusion, trichilemmal, and matrix cysts and that are found predominantly in dogs and cats. Many progress to trichoepitheliomas.
Dermoid cysts are congenital malformations found most commonly on the dorsal midline of the head or along the vertebral column. They are most commonly identified in Boxers, Kerry Blue Terriers, and Rhodesian Ridgeback dogs; Thoroughbred horses; and possibly Suffolk sheep. Typically multiple, they differ from other follicular cysts in that on cut surface they contain fully formed hair shafts. They are arguably the only true epidermal inclusion cysts, because they most likely represent an embryonal invagination of the epidermis with associated adnexa. These adnexa are responsible for the hair shafts within the cyst lumens.
Keratomas are cystic lesions in the hoof wall of the toe or, less frequently, the quarter or heel in simple or cloven-hoofed animals. They often develop secondary to a traumatic injury. Although often asymptomatic, they commonly induce lameness and deformity of the hoof wall or sole and may be associated with distal phalangeal lysis. Keratomas are seldom >5 cm in diameter and contain white to brown laminated keratin, often with a necrotic center associated with secondary inflammation. When lameness is present, surgical excision and curettage of the underlying bone, if affected, is the treatment of choice.
Dilated pores of Winer are rare, hair-follicle neoplasms recognized only in senior cats. Males may be predisposed. These lesions most often develop on the head. Clinically, they appear as solitary, dome-shaped lesions with the appearance of a giant comedo. Compact keratin may protrude through (above) the surface, giving them the appearance of a cutaneous horn. These lesions are benign, and complete excision is curative.
Tumors of the Hair Follicle
The hair follicle is a complex structure composed of eight different epithelial layers. Hair-follicle tumors display a similar complexity, and much work needs to be done to characterize them further. They are most common in dogs, less frequent in cats, and rare in other domestic animals.
Trichilemmomas are rare, benign, hair-follicle neoplasms of dogs, most commonly found on the head. Poodles may be predisposed. These tumors are derived from the lower portion of the outer root sheath and often have areas of transition into basal cell tumors. They have little in common with a tumor of the same name in people that represents an old wart. They appear as firm, ovoid masses, 1–7 cm in diameter, that are encapsulated but expand over time. Excision is curative.
Trichofolliculomas are extremely rare follicular tumors of dogs composed of the inferior and isthmic regions of multiple abortive follicles that extrude their lumenal contents into a dilated abnormal cystic infundibulum. Too few have been recognized to determine age, breed, or sex predilection. Considered by some to be more a hamartoma than a true neoplasm, these tumors are benign, and complete surgical excision is curative.
Trichoepitheliomas are cystic hair follicle neoplasms of dogs and, less commonly, cats, in which all elements of the hair follicle (infundibulum, isthmus, and inferior portions) and the patterns of cornification they produce are represented. The epithelium and cornification of the infundibular and isthmic portions predominate. Benign and malignant forms are recognized.
In dogs, these lesions can be seen at any age but are found most commonly during late middle age. Many breeds are predisposed, including Basset Hounds, Bull Mastiffs, Irish Setters, Standard Poodles, English Springer Spaniels, and Golden Retrievers. There is no defined sex predilection. Tumors can develop anywhere on the body but are most common on the trunk in dogs and on the head, tail, and extremities in cats. Benign forms appear as palpably encapsulated cystic nodules (1–5 cm in diameter) in the dermis and subcutaneous fat. Expansion of cysts or self-trauma may induce ulceration associated with extrusion of lumenal keratin that appears as a condensed, yellow, granular, caseous material. Excision is curative; however, animals that develop one such tumor are prone to develop additional lesions at other sites. This is especially true for Basset Hounds and English Springer Spaniels.
Malignant trichoepitheliomas are much less common than benign trichoepitheliomas and are differentiated by their local invasiveness, continuity with the epidermis, and association with extensive inflammation, necrosis, and fibrosis. Metastasis is uncommon. Wide surgical excision is the treatment of choice and is often curative in those tumors that are invasive but have minimal metastatic potential.
Pilomatricomas (hair matrix tumors, calcifying epitheliomas of Malherbe) are cystic hair-follicle neoplasms recognized almost exclusively in dogs. Unlike trichoepitheliomas, in which all elements of the follicle are represented, in pilomatricomas only the cells of the matrix region of the inferior part of the hair follicle and the cornification patterns they produce (hair shaft and inner root sheath) are present. Benign and malignant forms are recognized. Benign tumors are most common on the trunk of middle-aged dogs. Kerry Blue and Wheaten Terriers, Bouviers des Flandres, Bichons Frises, and Standard Poodles are most at risk. Grossly, these tumors are indistinguishable from trichoepitheliomas, but their cystic contents are often gritty because of mineralization. Excision is the treatment of choice. As in trichoepitheliomas, when one such lesion develops, additional lesions often develop over time.
Malignant pilomatricomas (malignant hair matrix tumor, matrical carcinoma) are rare and have been identified most often in dogs. They are a tumor of old dogs and grossly characterized as solitary or multinodular, variably cystic tumors that are often firmly attached to subjacent soft tissues. Because they are invasive, they are difficult to excise, and recurrence is common after attempts at surgical excision. They often metastasize to draining lymph nodes and internal organs, especially the lungs. Aggressive surgery is recommended. It is unknown whether they respond to radiation or chemotherapy.
Cutaneous Apocrine Gland Tumors

Courtesy of Dr. Alice Villalobos.
Sweat glands are of two types: apocrine and eccrine. Apocrine glands are tubular glands with a coiled secretory portion and a long, straight duct that flows into the follicular infundibulum. In domestic animals, all hair follicles have apocrine glands. Apocrine glands in dogs and cats are also present in association with the anal sac, and modified apocrine glands, known as ceruminous glands, are present in the external auditory meatus. In most mammals, apocrine glands produce an odiferous, oily compound that is a sexual attractant, a territorial marker, and a warning signal. In horses and cattle, these glands play a role in thermoregulation by producing sweat.
Apocrine gland tumors and malformations are most common in dogs and cats. Three diseases of apocrine glands of haired skin have been characterized.
Cystic apocrine gland dilations (apocrine gland cysts, cystic apocrine gland hyperplasia, apocrine cystomatosis) are best characterized as hamartomas. Two forms exist: a cystic form in which one or more cysts develop in the mid to upper dermis with a poor association with hair follicles, and a more diffuse form characterized by cystically dilated apocrine glands associated with multiple hair follicles in nontraumatized skin. Both are found in middle-age or older dogs and, less commonly, cats. The head and neck are the most common sites where these lesions develop. In both species, lesions appear as fluctuant dermal cysts or as translucent bullae. Complete excision is curative; however, this may be difficult to accomplish in the more diffuse form.
Apocrine gland adenomas are diagnosed almost exclusively in dogs, cats, and rarely horses. Two types are recognized based on whether their histologic appearance primarily resembles the secretory or ductular portion of the apocrine gland. Apocrine adenomas resemble the secretory region of the apocrine glands. They are found in older dogs and cats. Great Pyrenees, Chow Chows, and Alaskan Malamutes are the most commonly affected breeds. The head, neck, and extremities are the most frequent sites of development. In cats, apocrine adenomas are more likely to be seen in males, and no breed appears at greater risk than any other. The vast majority of apocrine adenomas occur on the head, especially the pinnae.
In horses, no age, sex, or breed association is known. The pinnae and vulva are the most likely regions to develop these tumors.
In all species, these tumors appear as firm to fluctuant cysts, seldom >4 cm in diameter. They contain varying amounts of clear to brownish fluid. In cats, the luminal fluid may be darkly pigmented, and apocrine cysts can be confused clinically with melanocytomas, especially when present on the inner aspect of the ears. Apocrine ductular adenomas are less common. They are found in older dogs and cats and are putatively derived from or show differentiation toward apocrine ducts. In dogs, these tumors are most commonly recognized in Peekapoos, Old English Sheepdogs, and English Springer Spaniels. They are often smaller, firmer, and less cystic than apocrine adenomas. Because they often consist of a large population of basal cells and because evidence of ductular differentiation can be extremely subtle, these tumors are often diagnosed histologically as basal cell tumors. Apocrine adenomas and apocrine ductular adenomas are benign, and complete surgical excision is curative.

Courtesy of Dr. Alice Villalobos.
Apocrine gland adenocarcinomas of haired skin are rare in all domestic animals but most frequently identified in older dogs and cats. In dogs, Treeing Walker Coonhounds, Norwegian Elkhounds, German Shepherd Dogs, and mixed-breed dogs are most at risk; in cats, Siamese may be predisposed. In both species, this tumor most commonly arises in axillary and inguinal regions—sites that allow it to be easily confused clinically and histologically with mammary gland ductular adenocarcinomas. Apocrine gland adenocarcinomas generally are larger than adenomas and have a variable clinical appearance ranging from fibrotic dermal nodules to ulcerated plaques. They are locally invasive and frequently metastasize to draining lymph nodes. Less commonly, skin and lung metastasis may occur. Complete surgical excision is the treatment of choice. Little is known about response to adjunct chemotherapy.
Apocrine Gland Tumors of Anal Sac Origin

Courtesy of Dr. Alice Villalobos.
Apocrine gland tumors of anal sac origin have been definitively identified in dogs and anecdotally in cats. Older English Cocker Spaniels, Springer Spaniels, Dachshunds, Alaskan Malamutes, German Shepherd Dogs, and mixed-breed dogs are most at risk. Unlike hepatoid gland tumors, these apocrine gland tumors have no sex predilection. They most commonly appear as deep, firm, nodular masses near the anal sac. As these lesions grow, they may compress the rectum and induce constipation.
Some of these tumors are associated with humoral hypercalcemia of malignancy, which causes anorexia, weight loss, polyuria and polydipsia, and mineralization of renal tissue with increased BUN and creatinine concentrations. These tumors are often highly infiltrative into the pelvic canal and commonly (90%) metastasize to the sublumbar lymph nodes or to distant internal organs (40%). Wide surgical excision, including involved lymph nodes, is the treatment of choice. Even if the tumor cannot be totally resected, debulking can be of value in dogs with pseudohyperparathyroidism, because the paraneoplastic hypercalcemia is related to the production of parathyroid hormone-related protein (PTHrP) from the total tumor volume. Intracavitary chemotherapy with 5-fluorouracil mixed with the animal's serum may help local control. Follow-up radiation therapy, intralesional chemotherapy, or systemic chemotherapy may increase the tumor-free interval. Adjunctive chemotherapy along with tyrosine kinase inhibitors, metronomic chemotherapy, immunotherapy, and radiation therapy may also delay progression, but few dogs are reported to live >1 year after the tumor has been recognized.
Eccrine Gland Tumors
Eccrine glands are the coiled, tubular, sweat glands present on the footpads of carnivores, the frog of ungulates, the carpus of pigs, and the nasolabial region of ruminants. Tumors derived from these glands are extremely rare and have been identified only on the footpads of dogs and cats. Most are malignant and invasive. These tumors are reported to have a high potential to metastasize to draining lymph nodes.
Sebaceous Gland Tumors
Tumors and tumor-like conditions of sebaceous glands are common in dogs, infrequent in cats, and rare in other domestic animals. Based on morphologic more than on behavioral features, four categories of benign sebaceous gland proliferations have been described. In people, in which a roughly similar classification scheme is traditionally used, it has been proposed that all benign sebaceous gland tumors be called sebaceomas.
Sebaceous gland hamartomas are solitary lesions reported only in dogs. These lesions are distinguished from sebaceous gland hyperplasias and adenomas because they are linear or circumscribed, several centimeters in length or diameter, and usually identified shortly after birth.
Sebaceous gland hyperplasias (senile sebaceous hyperplasias) represent a senile change in dogs and cats. In dogs, Manchester Terriers, Wheaten Terriers, and Welsh Terriers are at greatest risk. In cats, there is no breed predilection, but females develop these lesions more frequently than males. In both species, the skin of the head and abdomen are affected most commonly. Sebaceous hyperplasias commonly appear as papillated masses seldom >1 cm in diameter, often with a shiny, keratotic surface.
Sebaceous gland adenomas are seen in all domestic animals but are so common in older dogs and cats they can be considered primarily a small animal neoplasm. Coonhounds, English Cocker Spaniels, Cocker Spaniels, Huskies, Samoyeds, and Alaskan Malamutes are the canine breeds most likely to develop these tumors; Persians are the feline breed most predisposed. In dogs, these tumors frequently are clinically indistinguishable from sebaceous hyperplasias, but they tend to be larger (typically >1 cm). They are often multiple and may develop anywhere on the body; however, are commonly found on the head. Sebaceous adenomas may be covered with a serocellular crust and exhibit pleocellular inflammation and superficial pyoderma.
Sebaceous gland epitheliomas are a variant of sebaceous adenoma distinguished by lobules composed primarily of basal progenitor cells rather than mature sebocytes. Because they often have irregular lobules that extend into the deep dermis, they can occasionally be confused with sebaceous carcinomas. These tumors are found in older dogs and rarely in cats. They appear as ulcerated nodules that may be several centimeters in diameter. A papillated epidermal surface and pigmentation are variable findings.
Sebaceous gland adenocarcinomas are rare in domestic animals. They are recognized almost exclusively in dogs and cats, generally in middle-aged or older animals. Cavalier King Charles Spaniels; Cocker Spaniels; and Scottish Terriers, Cairn Terriers, and West Highland White Terriers are most at risk. Male dogs and female cats may be predisposed. These lesions are often ulcerated and may be indistinguishable from sebaceous epitheliomas or other cutaneous carcinomas. They are locally infiltrative and may metastasize to regional lymph nodes late in the disease.
Once a diagnosis is established, treatment is optional for benign sebaceous gland tumors unless they are secondarily inflamed and infected. For malignant adenocarcinomas, excision is the treatment of choice, but complete removal can be difficult because of the infiltrative nature of this tumor; adjunctive electroporation or radiotherapy may be required. Even benign sebaceous gland growths recur if remnants are left at the surgical site. In addition, animals that develop one sebaceous gland hyperplasia or adenoma often develop new lesions at other sites over time. No established protocol of chemotherapy for any of these lesions has been defined. Oral retinoids may prevent recurrence of sebaceous hyperplasia; however, their use remains poorly defined, and consultation with a veterinary oncologist or dermatologist is strongly recommended.
Hepatoid Gland Tumors

Courtesy of Dr. Alice Villalobos.
Hepatoid gland tumors are common neoplasms that arise from modified sebaceous glands that are most abundant in the cutaneous tissues around the anus but may also be present along the ventral midline from the perineum to the base of the skull, the dorsal and ventral tail, and in the skin of the lumbar and sacral regions. Because androgens stimulate the development of hepatoid glands, the incidence of proliferative lesions of hepatoid glands in sexually intact male dogs is three times that in females.

Courtesy of Dr. Alice Villalobos.
Benign hepatoid gland tumors are divided into hepatoid gland hyperplasias and adenomas; however, as with benign sebaceous gland tumors, there is a continuum from hyperplasia to adenoma. Here, they will be considered as a single entity.
Hepatoid gland adenomas are most common in senior dogs. Siberian Huskies, Samoyeds, Pekingese, and Cocker Spaniels are most commonly affected. Tumors may develop at any site where hepatoid glands are present; however, 90% are found in the perianal region. Grossly, they appear as one or (more commonly) multiple intradermal nodules 0.5–10 cm in diameter. Larger lesions commonly ulcerate, and hemorrhagic, proteinacious material can often be extruded with local pressure. Large tumors can compress the anal canal and make defecation difficult. Up to 95% of male dogs respond completely to castration; in those that do not, the pituitary-adrenal axis should be evaluated and, if no abnormality is detected, the dog should be reevaluated for the presence of a low-grade hepatoid gland adenocarcinoma.
Excision or laser ablation surgery may be used concurrently to remove extremely large or ulcerated tumors that have become secondarily infected. Surgery is the treatment of choice for females with hepatoid gland adenomas but may need to be repeated, because recurrence is common.
Radiation therapy is also an option and has a 2-year cure rate of 69% for benign tumors. Cryosurgery or electroporation are additional therapeutic alternatives; however, because of the complication of fecal incontinence, these techniques should be used only when tumors are not amenable to surgical intervention. Diethylstilbestrol has been used as an alternative to castration; however, because of severe adverse effects, including aplastic anemia and cystic prostatic hyperplasia, it should be used with extreme caution, if at all. Antiandrogens may have a role as an alternative to castration.
Hepatoid gland adenocarcinomas are uncommon canine neoplasms that generally appear as nodular lesions affecting the perianal region. These tumors are found in male dogs 10 times more commonly than in females. Siberian Huskies, Alaskan Malamutes, and Bulldogs are most likely to develop this tumor.
Histologic evaluation is the best means of diagnosis; however, there is debate about how to distinguish low-grade malignant tumors from hepatoid adenomas, because well-differentiated forms can be confused with adenomas, and anaplastic forms can be confused with apocrine gland adenocarcinomas of anal sac origin. These tumors have metastatic potential and often spread to regional lymph nodes.
Treatment consists of wide surgical excision including involved lymph nodes and, possibly, subsequent radiation. These tumors are generally not responsive to castration or to estrogen therapy; however, some studies show that the administration of masitinib, toceranib, and other tyrosine kinase inhibitors may overcome chemoresistance, inhibit the proliferation of tumor cells, and prevent the emergence of metastasis. These findings may increase the benefit of combining targeted agents with various forms of chemotherapy such as oral piroxicam and capecitabine or with metronomic chemotherapy to prevent or treat local recurrence and metastatic disease. The overall prognosis is guarded.
Primary Cutaneous Neuroendocrine Tumors
In veterinary medicine, the diagnosis of tumors derived from Merkel cells (tactile, neurosecretory cells of epithelial derivation present in the basal cell layer of the epidermis) has fallen in disfavor, and most pathologists consider this tumor to be an extramedullary plasmacytoma. Merkel cell tumors most likely develop in animals but are not recognized as such.
Papillomas

Courtesy of Dr. Alice Villalobos.


Courtesy of Dr. Alice Villalobos.
Papilloma viruses are small, double-stranded DNA viruses of the Papovaviridae family. Some mammals have several distinct papilloma viruses: people have >20; cattle, 6; dogs, 3; and rabbits, 2. Different papilloma viruses often have considerable species, site, and histologic specificity. The virus is transmitted by direct contact, fomites, and possibly by insects. Papillomas have been reported in all domestic animals, birds, and fish. Multiple papillomas (papillomatosis) of skin or mucosal surfaces generally are seen in younger animals and are usually caused by viruses. Papillomatosis is most common in cattle, horses, and dogs. Single papillomas are more frequent in older animals; however, they may not always be caused by viral infection.
When lesions are multiple, they may be sufficiently characteristic to confirm the diagnosis; however, there are many stimulants of warts, and a definitive diagnosis requires identification of the virus or its cytopathic effects on individual cells—a change known as koilocytic atypia or koilocytosis.
In cattle, warts commonly are found on the head, neck, and shoulders, and occasionally on the back and abdomen. The extent and duration of the lesions depend on the type of virus, area affected, and degree of susceptibility. Warts appear ~2 months after exposure and may last ≥1 year. Papillomatosis becomes a herd problem when a large group of young, susceptible cattle becomes infected. Immunity usually develops 3–4 weeks after initial infection, but papillomatosis occasionally recurs, probably due to loss of immunity.
Although most warts appear as epidermal proliferations that have a keratotic surface resembling a cauliflower (verruca vulgaris), some bovine papilloma viruses (bovine papilloma types 1 and 2) involve dermal fibroblasts and keratinocytes and appear as a papulonodule with a warty surface. Such fibropapillomas may involve the venereal regions, where they can cause pain, disfigurement, infection of the penis of young bulls, and dystocia when the vaginal mucosa of heifers is affected.
A form of persistent cutaneous papillomatosis with smaller numbers of papillomas may be seen in herds of older cattle. A bovine papilloma virus has been demonstrated in bladder tumors associated with bracken fern ingestion and in upper GI tract papillomas of cattle in Scotland. It is believed that the papilloma virus acts as a co-carcinogen. When bovine papilloma virus type 1 or 2 is injected into the skin of horses, a dermal tumor similar to equine sarcoid develops.


Courtesy of Dr. Thomas Lane.
In horses, small, scattered papillomas develop on the nose, lips, eyelids, distal legs, penis, vulva, mammary glands, and inner surfaces of the pinnae, often secondary to mild abrasions. They can be a herd problem, especially when young horses are kept together, but regress in a few months, as a foal’s immune system matures. When they develop in older horses, they often persist for >1 year. So-called aural plaques are also thought to be a flat form of papilloma (verruca planum). Equine papillomas are disfiguring but benign. They should be distinguished from verrucous equine sarcoid.
In dogs, three clinical presentations of canine papilloma virus infection have been described. The first is canine mucous membrane papillomatosis, which primarily affects young dogs. It is characterized by the presence of multiple warts on oral mucous membranes from lips to (occasionally) the esophagus and on the conjunctival mucous membranes and adjacent haired skin. When the oral cavity is severely affected, there is interference with mastication and swallowing. A viral etiology has been clearly established for these lesions. Azithromycin therapy has been shown to speed up regression in dogs.
The second clinical presentation of canine papilloma virus infection is cutaneous papillomas, which are indistinguishable from the warts that develop on or around mucous membranes. However, they are more frequently solitary and develop on older dogs. Cocker Spaniels and Kerry Blue Terriers may be predisposed. A definitive viral etiology has not been established, and lesions may be confused with cutaneous tags. A syndrome characterized by papillomatosis of one or more footpads has also been described. Clinically, lesions appear as multiple, raised keratin horns. A viral etiology has been suggested but not proved. Cryotherapy is useful.
The third clinical presentation of canine papilloma virus infection is cutaneous inverted papillomas, which have more in common clinically with intracutaneous cornifying epitheliomas. In this disease of young, mature adult dogs, lesions most commonly develop on the ventral abdomen, where they appear as raised papulonodules with a keratotic center. Infrequently, viral papillomas in dogs may progress to invasive squamous cell carcinomas.
In cats, papilloma virus infection appears most commonly as a multicentric squamous cell carcinoma. The typical warty lesions associated with papilloma virus infection in most species are not present. Papillomas may affect the skin of goats, and infection on the teats has been reported to induce malignant transformation. In sheep, papillomas are rare and most commonly appear as fibropapillomas. In pigs, they are very rare and when present are identified as solitary or multiple lesions on the face or genitalia. (Also see papillomatosis in rabbits.)
A cutaneous fibroma occurs in white-tailed, black-tailed, and mule deer, and in antelope, moose, and caribou. It is caused by a papilloma virus that resembles a bovine papilloma virus and is found only in the epithelium that covers the tumors.
Infectious papillomatosis is a self-limiting disease, although the duration of warts varies considerably. Various treatments have been advocated without agreement on efficacy. Surgical removal is recommended if the warts are sufficiently objectionable. However, because surgery in the early growing stage of warts may lead to recurrence and stimulation of growth, the warts should be removed when near their maximum size or when regressing. Affected animals may be isolated from susceptible ones, but with the long incubation period, many are likely to have been exposed before the problem is recognized.
Vaccines are of some value as a preventive but are of little value in treating cattle that already have lesions. Because wart viruses are mostly species-specific, there is no merit in using a vaccine derived from one species in another. An intralesional lymphocyte T-cell immunomodulator (LTCI), which stimulates T cells and endogenous IL-2 levels, may benefit individual animals that develop multiple or persistent warts. In addition to azithromycin, topical imiquimod cream may also help the immune system to resolve these warts in dogs.
When the disease is a herd problem, it can be controlled by vaccination with a suspension of ground wart tissue in which the virus has been killed with formalin. Autogenous vaccines may be more effective than those commercially available. It may be necessary to begin vaccination in calves as early as 4–6 weeks of age with a dose of ~0.4 mL intradermally administered at two sites. The vaccination is repeated in 4–6 weeks and at 1 year of age. Immunity develops in a few weeks but is unrelated to whatever mechanism is involved in spontaneous regression. If the animal was exposed to the virus before vaccination, immunity may develop too late to prevent warts. A vaccination program must be in effect for ~3–6 months before its preventive value will be evident. Vaccination should be continued for ≥1 year after the last wart disappears, because the premises may still be contaminated. Stalls, stanchions, and other inert materials can be disinfected by fumigating with formaldehyde.







