

Parturition tends to be uneventful in goats, with the incidence of dystocia < 5%. Induction of parturition is a useful technique to increase survival in dairy goat kids and to catch and separate kids from dams before they suckle in herds with control programs for caprine arthritis and encephalitis virus and mycoplasma. Induction with synthetic PGF2alpha analogues such as cloprostenol (125 mg) or dinoprost tromethamine (10 mg) usually results in delivery of kids ~30–35 hours after injection, whereas dexamethasone (20 mg) requires ~48 hours to induce kidding. Viability of multiple fetuses may be compromised if parturition is induced before day 144.
If the doe has been in active labor for 30 minutes with no progress, assistance is likely required. Most kids present cranially, in dorsosacral position, with front limbs extended. If kids present caudally, which is more common in twins, triplets, and quadruplets than in singletons, assistance for delivery is more likely to be required. The most common cause of dystocia is when two or more kids present simultaneously, which requires an experienced practitioner to identify and correct. Other causes of dystocia in does include malposition, fetomaternal mismatch, failure of cervical dilation (ringwomb), vaginal prolapse, uterine torsion, and uterine inertia. Most dystocias can be corrected by repositioning kids and providing lubrication and traction. However, in more severe cases, fetotomy or cesarean section may be necessary.
When assisting with kidding, extreme care must be taken to prevent uterine tears, which can be diagnosed on palpation of the uterus after the dystocia. Small tears (< 1 cm) can be treated by hastening involution of the uterus with oxytocin administration. Larger tears may require surgical intervention to minimize excessive bleeding and peritonitis. Systemic antimicrobials, anti-inflammatory drugs, and a clostridial vaccine booster should be administered to does after a prolonged dystocia.
Retained placenta (defined as placenta not passed 12 hours after parturition) is uncommon in goats and is usually associated with selenium deficiency, the birth of a mummified or rotten fetus, or a difficult delivery. It can be treated by gentle traction or oxytocin administration to facilitate expulsion; however, diagnosis and treatment of the underlying cause will usually solve the problem.

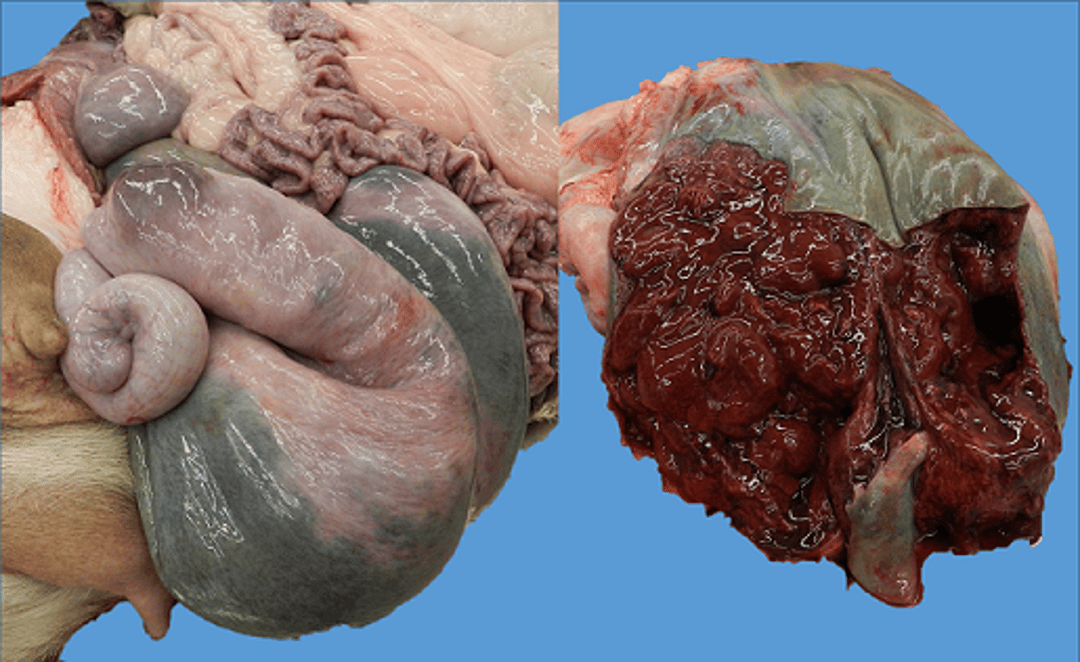
Postmortem examination of a uterus from a doe that succumbed to toxic metritis after a dystocia. Left:A uterus that became necrotic, likely due to prolonged ischemia when a kid was lodged in the pelvic canal. After the doe delivered the kid, the uterus became colonized with Clostridium perfringens, and the doe became toxic. Right: Total protein decreased to 4 g/L due to the massive inflammatory response within the uterus.
Courtesy of Dr. Jamie Stewart and the Veterinary Diagnostic Laboratory at the University of Illinois, Urbana-Champaign.
Metritis is almost always a sequela of dystocia and/or retained placenta, and systemic antimicrobials are warranted. Clostridial organisms (Clostridium tetani and C perfringens) may colonize the uterus, resulting in a frequently fatal toxemia that requires aggressive supportive care, antimicrobials, and antitoxin therapy. Less severe causes of metritis may lead to a chronic endometritis and cause infertility if not treated.
Uterine prolapse is uncommon in goats but may occur after dystocia. Treatment is similar to that in other species, and prognosis is good if recognized and treated early.
In extremely cold weather, newborn kids should be dried (especially the ears) to prevent frostbite. Heat lamps are not necessary if the kids are dry, well fed, and out of a draft. Kids born in intensive systems should have their navels dipped in tincture of iodine to prevent infection. Angora, pygmy, and meat kids are typically raised on the dam. Dairy goat kids often are removed at birth and, after receiving colostrum, fed from a bottle or nipple-pail.





