




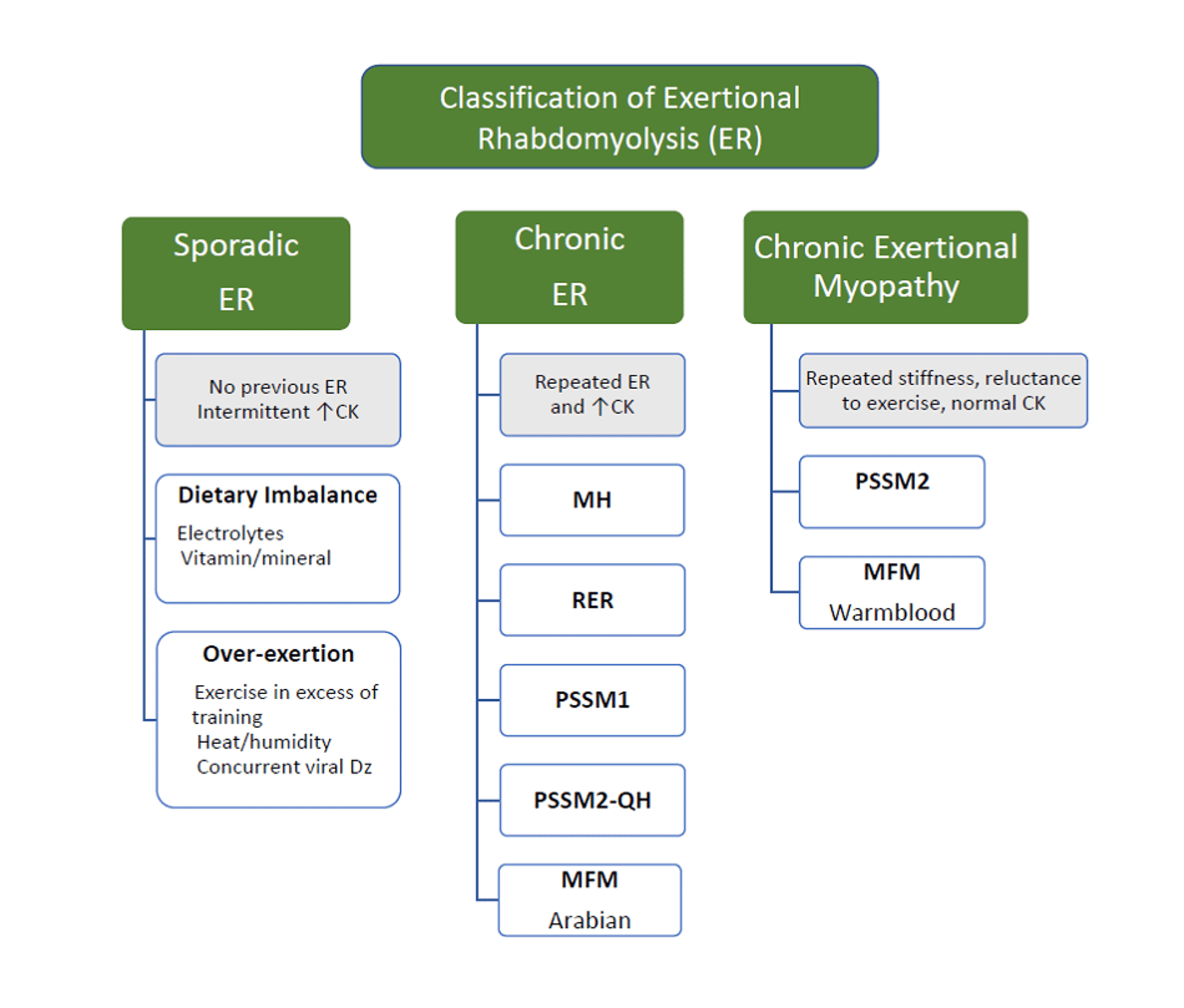
Exertional myopathy in horses is a syndrome of muscle fatigue, pain, or cramping associated with exercise. Less common exertional myopathies that cause exercise intolerance without muscle necrosis include mitochondrial myopathies, type 2 polysaccharide storage myopathy, and myofibrillar myopathy in Warmblood and Arabian horses. Most commonly, exertional myopathies produce necrosis of striated skeletal muscle and are termed exertional rhabdomyolysis. Although exertional rhabdomyolysis was previously considered a single disease described as azoturia, tying-up, or cording up, it is now known to comprise several myopathies, which, despite similarities in clinical presentation, differ notably in etiopathogenesis.

Courtesy of Dr. Stephanie Valberg.
Clinical signs usually are observed shortly after onset of exercise. Excessive sweating, tachypnea, tachycardia, muscle fasciculations, reluctance or refusal to move, and firm, painful lumbar and gluteal musculature are common clinical signs. Episodes range from subclinical to severe muscle necrosis with recumbency and myoglobinuric renal failure. Severity varies extensively between individuals and to some extent within the same individual. A diagnosis of exertional rhabdomyolysis is based on demonstration of abnormal increases in serum CK, lactate dehydrogenase, and AST activities.
Exertional rhabdomyolysis can be either sporadic, with single or very infrequent episodes of exercise-induced muscle necrosis, or chronic, with repeated episodes of rhabdomyolysis and increased serum CK or AST activities with mild exertion.
Sporadic Exertional Rhabdomyolysis
All breeds of horses are susceptible to sporadic exertional rhabdomyolysis. The most common cause is exercise that exceeds the horse’s state of training. The incidence of muscle stiffness also has been found to increase during an outbreak of respiratory disease. Dietary deficiencies of sodium, vitamin E, selenium, or a calcium-phosphorus imbalance may also be contributory factors.
A diagnosis of sporadic exertional rhabdomyolysis is made on the basis of a horse with no previous history or a brief history of exertional rhabdomyolysis, clinical signs of muscle cramping and stiffness after exercise, and moderate to marked increases in serum CK and AST activities.
Immediately on detection of clinical signs of exertional rhabdomyolysis, exercise should stop and the horse should be moved to a well-bedded stall with access to fresh water. The objectives of treatment are to relieve anxiety and muscle pain and to correct fluid and acid-base deficits. Tranquilizers with opioids can provide immediate relief of anxiety and stiffness; NSAIDs can be administered to a well-hydrated horse. Most horses are relatively pain free within 18–24 hours.
Severe rhabdomyolysis can lead to renal compromise due to ischemia and the combined nephrotoxic effects of myoglobinuria, dehydration, and NSAID treatment. The first priority in horses with hemoconcentration or myoglobinuria is to reestablish fluid balance and induce diuresis. In severely affected animals, regular monitoring of BUN or serum creatinine concentration is advised to assess the extent of renal damage. Diuretics are contraindicated in the absence of IV fluid therapy and are indicated in combination with IV fluid therapy if the horse is in oliguric renal failure.
Horses should be stall rested on a hay diet with a dietary vitamin and mineral ration balancer supplement for up to a few days. For horses with sporadic forms of exertional rhabdomyolysis, rest with regular access to a paddock should continue until serum muscle enzyme activities are normal. Because the inciting cause is usually temporary, most horses respond to rest, a gradual increase in training, and dietary adjustment. Endurance horses should be encouraged to drink electrolyte-supplemented water during an endurance ride and monitored particularly closely during hot, humid conditions.
Chronic Exertional Rhabdomyolysis
Some horses have recurrent episodes of rhabdomyolysis, even with light exercise. Four forms of chronic tying-up have been identified on the basis of muscle biopsies or genetic testing: type 1 polysaccharide storage myopathy (PSSM), type 2 PSSM, malignant hyperthermia, and recurrent exertional rhabdomyolysis. Horses with chronic exertional rhabdomyolysis do not respond well to prolonged rest and, unlike horses with sporadic exertional rhabdomyolysis, are often put back into exercise before serum CK activity is within normal limits.
Type 1 polysaccharide storage myopathy occurs frequently in Quarter Horse–related breeds (especially halter and Western pleasure horses), Morgans, and draft horses; however, it is also present in at least 20 other horse breeds. It is caused by a dominantly inherited mutation in the glycogen synthase 1 (GYS1) gene. A diagnosis can be made by genetic testing of blood or hair samples.
Quarter Horse–related breeds and other crossbred or light breeds of horses with type 1 PSSM often develop episodes of rhabdomyolysis at a young age with little exercise. Rest for a few days before exercise is a common triggering factor. Episodes are characterized by a tucked-up abdomen, a camped-out stance, muscle fasciculations, sweating, gait asymmetry, hind limb stiffness, and reluctance to move. Some horses paw or roll, with signs resembling colic. Serum CK and AST activities are increased during an episode (usually >1,000 U/L) and, unlike in other forms of rhabdomyolysis, subclinical episodes characterized by persistently abnormal CK activity are common. Serum CK activity remains elevated for longer periods of time than with sporadic or other forms of chronic rhabdomyolysis. Chronic clinical signs in draft horses may include loss of muscle mass, progressive weakness, and recumbency with normal serum CK and AST activities. When draft horses develop rhabdomyolysis, CK and AST activities may be markedly increased, and horses can become myoglobinuric, weak, and reluctant to rise.
Type 2 polysaccharide storage myopathy occurs in light breeds such as Arabians, Morgans, Thoroughbreds, a variety of Warmblood breeds, and some Quarter Horses. A diagnosis is made by identifying an abnormal pattern of glycogen storage in muscle biopsies in a horse with a negative GYS1 genetic test. Chronic episodes of muscle stiffness, soreness, and muscle atrophy with normal to modest increases in serum CK activity are common in horses with type 2 PSSM. Many cases of type 2 PSSM in Arabian and Warmblood horses have been reclassified as myofibrillar myopathy.


Courtesy of Dr. Stephanie Valberg.


Courtesy of Dr. Stephanie Valberg.

Myofibrillar myopathy is a newly recognized disorder in Arabian and Warmblood horses. In Arabian horses, it occurs most commonly in endurance horses and is characterized by muscle pain, stiffness, and elevated serum CK and AST activities. This occurs at the end of endurance rides or about 5 miles into rides that are preceded by 1– 2 weeks of rest. The most common signs of myofibrillar myopathy in Warmbloods are mild shifting lameness, exercise intolerance, and loss of muscle mass that is not accompanied by a concomitant rise in serum CK activity. Myofibrillar myopathy is linked to aberrations in the Z-disk of the sarcomere and alterations in cysteine-based antioxidants such as glutathione and peroxiredoxins.
Malignant hyperthermia is caused by an autosomal dominant mutation in the skeletal muscle ryanodine receptor gene (RYR1). The mutation is responsible for both anesthesia-related and non–anesthesia-related causes of rhabdomyolysis in Quarter Horses. A diagnosis can be made by genetic testing of blood or hair roots. Clinical signs related to inhalation anesthesia include tachycardia, tachypnea, hyperthermia, and muscle rigidity accompanied by severe lactic acidosis, increased serum CK activity, and electrolyte derangements. Exertional rhabdomyolysis in Quarter Horses with malignant hyperthermia can result in sudden death or clinical signs of excessive sweating, tachycardia, tachypnea, hyperthermia, and muscle rigidity. Some Quarter Horses have both malignant hyperthermia and PSSM, which results in more severe clinical signs of exertional rhabdomyolysis than those that occur in horses with PSSM alone.
Recurrent exertional rhabdomyolysis occurs frequently in Thoroughbreds, Standardbreds, and Arabian horses that are in high-stress environments. It is likely due to abnormal regulation of intracellular calcium in skeletal muscles with acute episodes of rhabdomyolysis triggered by stress. Horses are most susceptible to the condition if they are fit, fed high nonstructural carbohydrate diets, and have a nervous temperament.
Diagnostic tests to determine the cause of chronic tying-up include a CBC, serum biochemical analysis, measurement of serum vitamin E and selenium concentrations, dietary analysis, exercise testing, genetic testing, and muscle biopsy. An exercise challenge test is useful to detect subclinical cases; serum CK activity is measured before and 4 hours after light exercise. In addition, quantifying the extent of exertional rhabdomyolysis during mild exercise is helpful in deciding how rapidly to reinstate training.
A diagnosis of type 1 PSSM is based on identification of the GYS1 mutation. If muscle biopsies are examined, muscle fibers with subsarcolemmal vacuoles, dark periodic acid-Schiff (PAS) staining for glycogen, and, most notably, amylase-resistant abnormal complex polysaccharide are usually present. A diagnosis of type 2 PSSM is based on the absence of the GYS1 mutation and the presence of muscle fibers with aggregates of amylase-sensitive PAS-positive staining glycogen and occasionally small amounts of amylase-resistant PAS-positive material. A diagnosis of myofibrillar myopathy is made by identifying aggregates of the cytoskeletal protein desmin in muscle biopsy samples. A diagnosis of recurrent exertional rhabdomyolysis is based on history, clinical signs, increases in serum CK and AST activities, and muscle biopsy. Muscle biopsy is useful for the evaluation of horses during periods when they have clinical signs of muscle disease and during which a diagnosis can lead to beneficial changes in management. Muscle biopsy is not recommended for use in prepurchase examinations or breeding decisions.
Horses with type 1 PSSM have constitutively active glycogen synthase that is further stimulated by increased blood insulin concentrations, resulting in high muscle glycogen concentrations. When fed a starch meal, these horses take up a higher proportion of the absorbed glucose in their muscles than do healthy horses. Quarter Horse-related breeds with type 2 PSSM also have abnormal glycogen storage, and, although the cause of this myopathy is unknown, they are fed similarly. The ideal diet for PSSM is based on feeding forage at a rate of 1.5%–2% body wt, providing >15% of digestible energy as fat and limiting starch to < 10% of daily digestible energy by limiting grain or replacing it with a fat supplement. Caloric needs should be assessed first to prevent horses becoming obese on a high-fat diet. Improvement in clinical signs of exertional rhabdomyolysis for horses with PSSM requires both dietary changes and gradual increases in the amount of daily exercise and turn-out.
The approach to feeding Arabian and Warmblood horses with type 2 PSSM and myofibrillar myopathy has changed. If horses with type 2 PSSM do not respond satisfactorily to a diet low in nonstructural carbohydrates and high in fat, a trial period of 6–8 weeks on a myofibrillar myopathy diet is warranted. The myofibrillar myopathy diet consists of moderate nonstructural carbohydrates (20–39%, as indicated on feed bag) and moderate fat (4–8%, as indicated on feed bag) with higher levels of protein (12–14%, as indicated on feed bag). Whey-based amino acid supplements rich in cysteine, additional antioxidants such as coenzyme Q10, and adequate vitamin E are also recommended.
Horses with malignant hyperthermia may benefit from premedication with dantrolene (4 mg/kg, PO) 60–90 minutes before exercise, particularly under hot conditions.
Management of recurrent exertional rhabdomyolysis is aimed at decreasing the triggering factors for excitement and pharmacological alteration of intracellular calcium flux with contraction. Management changes that may decrease excitement include minimizing stall confinement by using turn-out or a hot walker, exercising and feeding horses with recurrent exertional rhabdomyolysis before other horses, providing compatible equine company, and the judicious use of low-dose tranquilizers during training. A high-fat, low-starch diet is beneficial, possibly by decreasing excitement.
In contrast to horses with PSSM, those with recurrent exertional rhabdomyolysis often require higher caloric intakes (>24 Mcal/day). At these high caloric intakes, specialized feeds designed for exertional rhabdomyolysis are necessary, because additional vegetable oil or rice bran cannot supply enough calories for equine athletes in intense training. Hay should be fed at 1.5%–2% body wt, and high-fat, low-starch concentrates should be selected that provide ≤20% of daily digestible energy as nonstructural carbohydrate and 20%–25% of digestible energy as fat.
Dantrolene (4 mg/kg, PO) administered 1 hour before exercise may decrease the release of calcium from the calcium release channel. Phenytoin (1.4–2.7 mg/kg, PO, every 12 hours) has also been advocated as a treatment for horses with recurrent exertional rhabdomyolysis. Therapeutic ranges vary, so oral dosages are adjusted by monitoring serum concentrations to achieve 8–12 mcg/mL. However, long-term treatment with dantrolene or phenytoin is expensive.
For More Information
Also see pet health content regarding muscle disorders in horses.







