




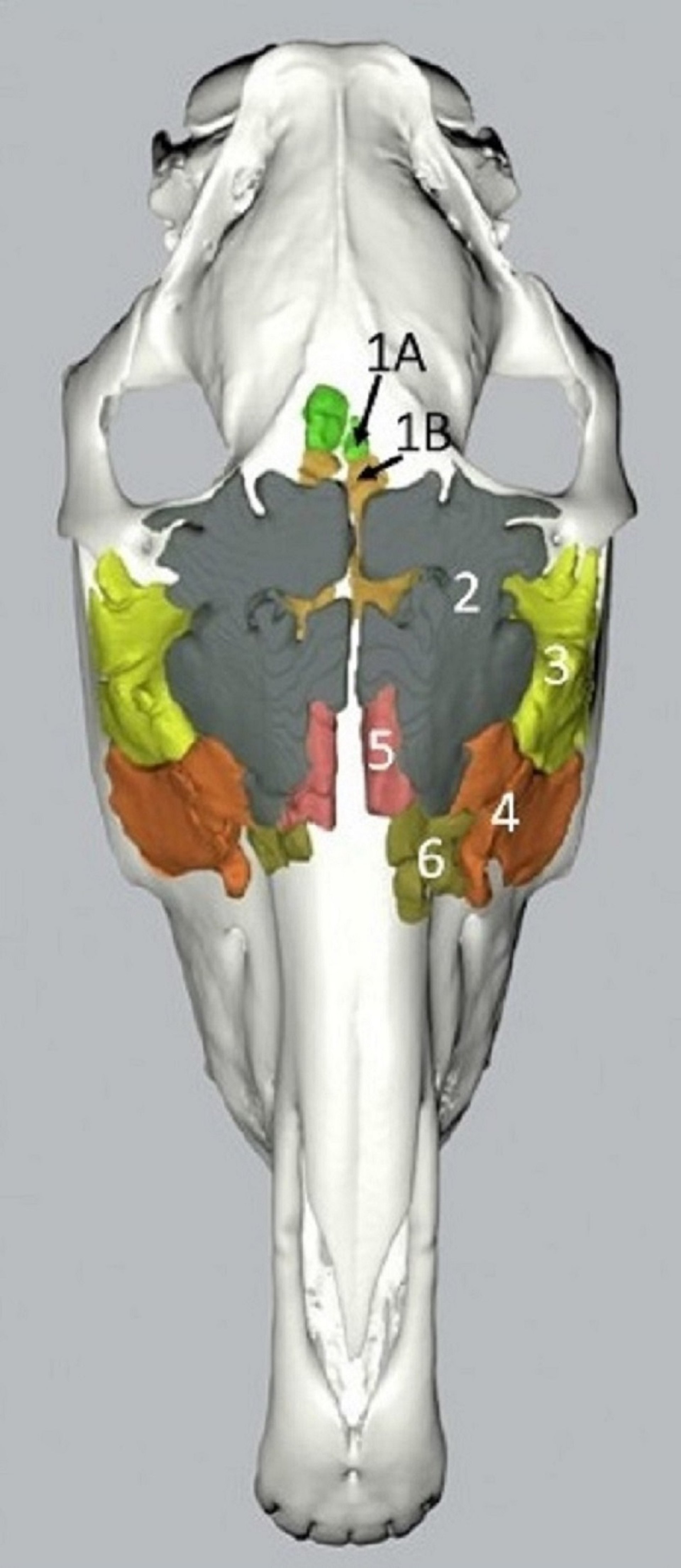
The paranasal sinus system of the horse consists of paired frontal, conchal (dorsal and ventral compartments), sphenopalatine, and maxillary (rostral and caudal compartments) sinus compartments.
Paranasal sinuses in the horse
Paranasal sinuses in the horse. Illustration by Dr. Georghe Constantinescu. |

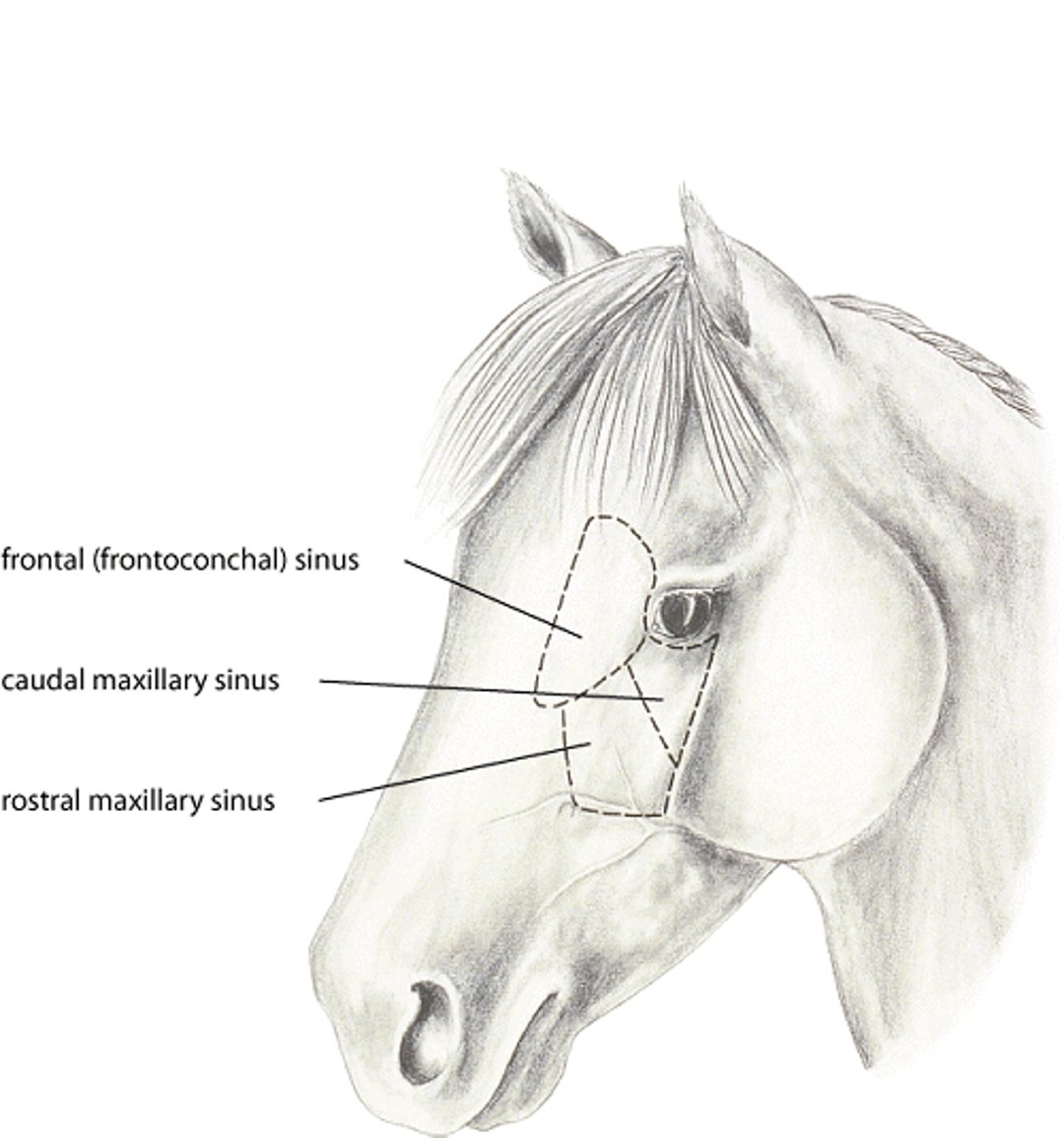

Courtesy of Dr. Dewey Wilhite, Auburn University.
The maxillary sinus is the largest paranasal sinus and is divided by a thin septum into caudal and rostral parts. The rostral maxillary sinus contains the root of the first maxillary molar (109/209) and the caudal maxillary sinus contains the root of the second (110/210) and third molar (111/211). The frontal sinus has a large communication with the dorsal conchal sinus rostrally, forming the conchofrontal sinus. The dorsal and ventral conchae are divided into rostral and caudal compartments. The rostral compartment is an air-filled turbinate or bulla within the nasal passage. The caudal compartment of the dorsal and ventral concha form the dorsal conchal and ventral conchal sinus compartments. The caudal and rostral maxillary sinuses have separate openings into the middle nasal meatus, and the caudal maxillary sinus communicates with the frontal sinus through the large frontomaxillary opening. Diseases that originate in one sinus cavity may extend to and involve other compartments. The sphenopalatine sinus communicates with the caudal maxillary sinus, and the ventral conchal sinus can be accessed from the rostral maxillary sinus.
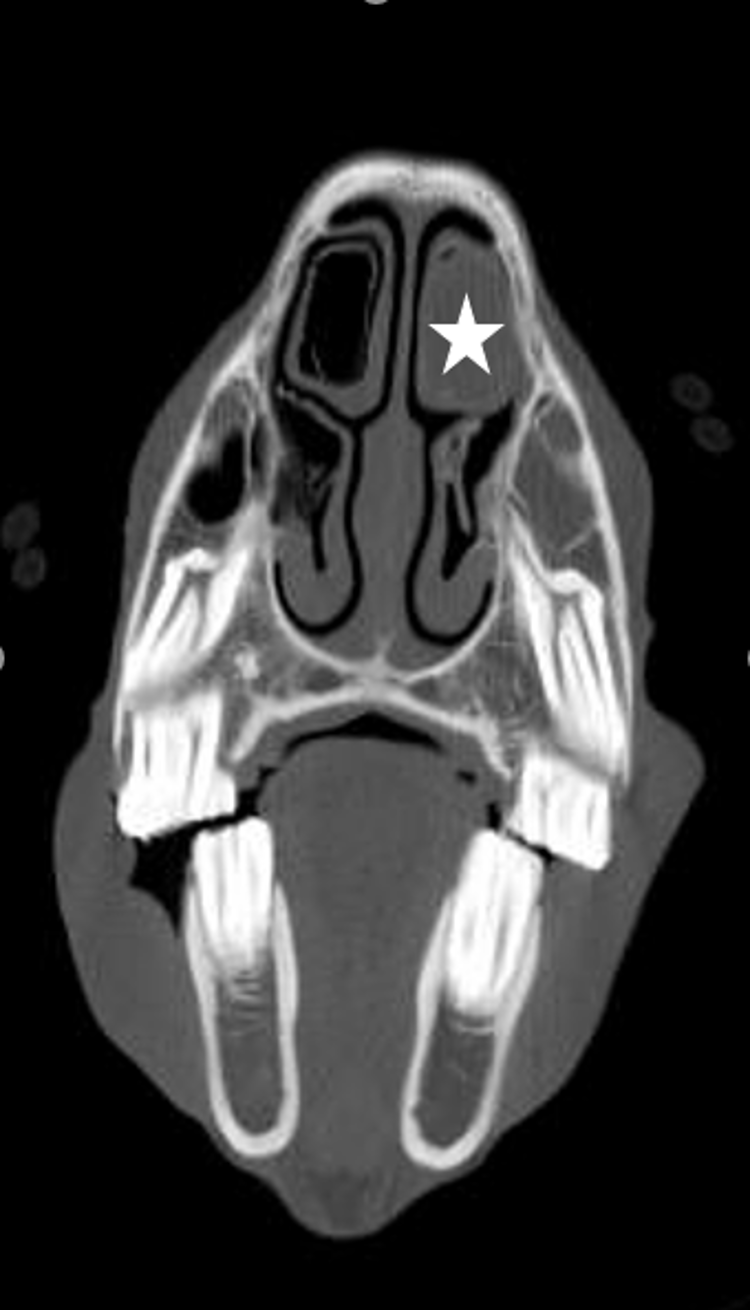
Diseases of the paranasal sinuses usually cause mucopurulent or bloody nasal discharge. Drainage is unilateral, in contrast to bilateral discharge in respiratory diseases originating distal to the nasal passages. Unilateral facial swelling, epiphora, and inspiratory noise are other common manifestations of sinus disease. On endoscopy, purulent material, a mass, or blood can sometimes be seen within the nasal passage and originating from the nasomaxillary opening. Radiographs of the skull may reveal fluid or a discrete mass within the sinus, changes to the roots of the maxillary molars, or lytic/proliferative bony changes associated with neoplasia. CT scan is useful in deciphering affected sinus compartments, particularly the involvement of the ventral conchal and sphenopalatine sinuses, and for detecting subtle changes to the periapical region of the teeth.
Centesis of the maxillary or frontal sinuses is performed to obtain fluid for cytologic analysis and bacterial culture and sensitivity. Sinoscopy can be performed in the standing horse with sedation and local anesthesia; after a trephine hole is created, the endoscope is inserted to allow direct inspection of the frontal or maxillary sinuses. This procedure can aid diagnosis, debridement/removal of purulent debris, and assist with anatomic placement of an indwelling lavage system. Flap sinusotomy is often needed to treat sinus disease. For complete evaluation of the paranasal sinuses, fenestration of the maxillary septal bulla is needed and is generally performed during sinusotomy. This provides access to the rostral and ventral conchal sinus compartments from the frontal and/or caudal maxillary sinus. This procedure is usually performed in the standing, sedated patient using appropriate local anesthetic techniques. General anesthesia is required in severe disease or in patients refractory to standing sinusotomy.
Sinusitis
Primary Sinusitis

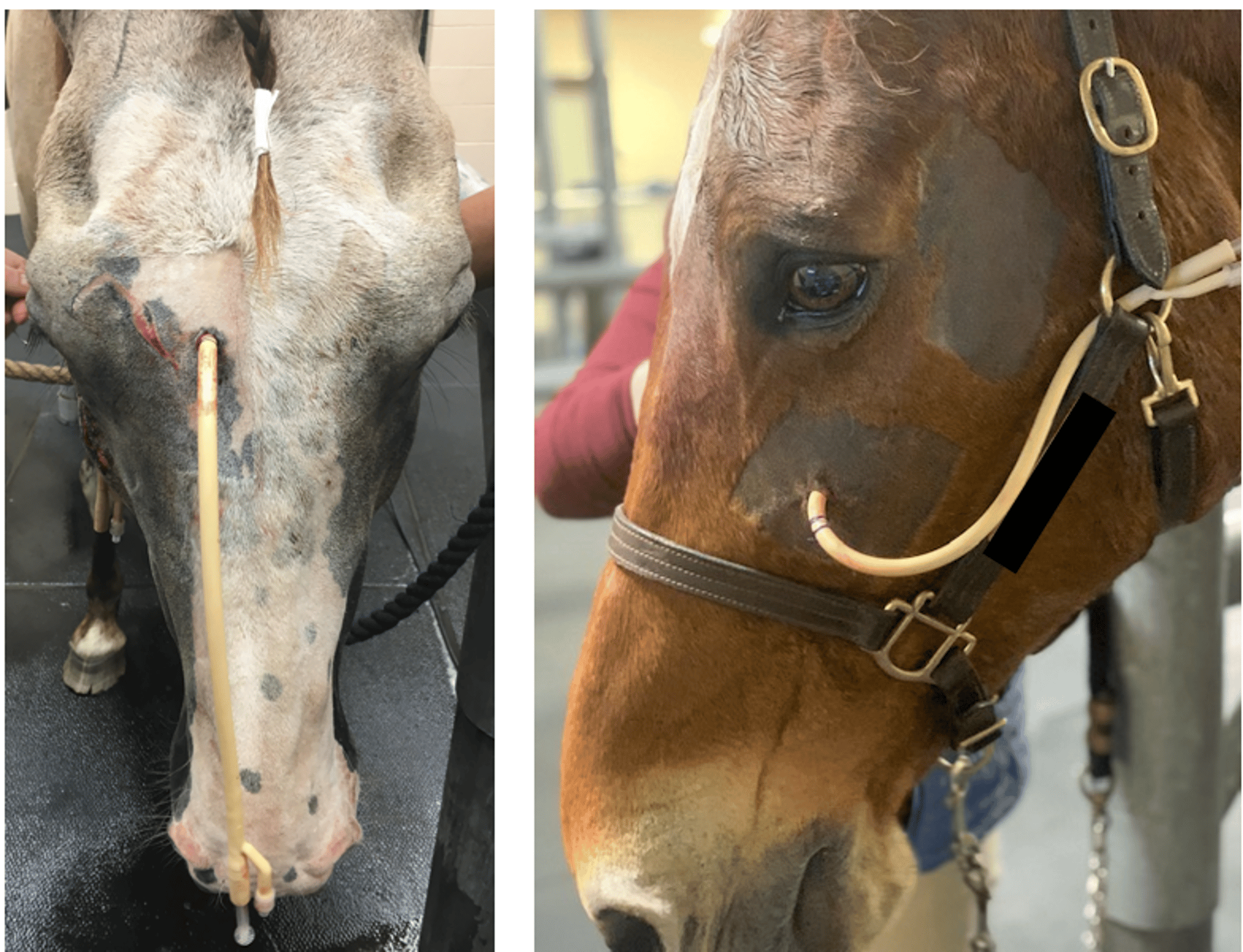
Courtesy of Dr. Lindsey Boone, Auburn University.
Primary sinusitis occurs subsequent to previous upper respiratory tract infection. Disease typically involves all sinus compartments. Diagnosis is made based on radiographic evidence of fluid accumulation within one or all sinus compartments and ruling out other primary causes of sinusitis. Treatment includes ensuring adequate sinus drainage, sinus lavage, and appropriate antimicrobial treatment. NSAID administration may help facilitate drainage by reducing swelling of the mucosa. Sinus lavage can be performed via trephination of the conchofrontal or maxiallary sinuses. If sinusitis does not resolve with antimicrobials and lavage alone, the presence of exudate within the ventral conchal sinus or the nasal conchal bulla should be suspected. For persistent disease of the ventral conchal sinus, surgical removal of the exudate from the ventral conchal sinus is performed via sinoscopy and maxillary septal fenestration or a maxillary bone flap. If empyema of the nasal conchal bulla is identified, endoscopic fenestration can also be performed with a surgical laser to provide drainage.

Courtesy of Dr. Lindsey Boone, Auburn University.
Secondary Sinusitis
Secondary sinusitis is more common than primary sinusitis in horses, and of the causes of secondary sinusitis (dental, cysts, neoplasia, ethmoid hematoma), dental-associated sinusitis is the most common. Dental-associated sinusitis results from a breach of the alveoli of the maxillary ’08–11 teeth, due to severe inflammation and infection of the periapical or periodontal space. Clinical signs include mucopurulent, malodorous unilateral nasal discharge. Oral examination is usually normal in horses with periapical abscessation. Identification of fistulae, fracture, or deep infundibular or peripheral caries during oral examination warrant further investigation due to possible ascending infection causing sinusitis. CT scan of the skull is indicated, or skull radiographs and dental radiographs when CT is not available or for confirmation of the initial diagnosis and planning with the client. Widening of the periapical space along the tooth root and blunting of the tooth roots are the most common radiographic findings in horses with periapical abscessation. Secondary sinus infection may be contained to the sinus compartment communicating with the compromised alveolus, or may spread to other compartments. Once the affected tooth is identified, it is removed by oral extraction or sinus surgery when necessary, followed by treatment with NSAIDs, antimicrobials, and sinus lavage. Sinusitis in horses is commonly associated with recurrence or incomplete resolution of the nasal discharge. If clinical signs do not resolve, repeat CT and sinusotomy are indicated.
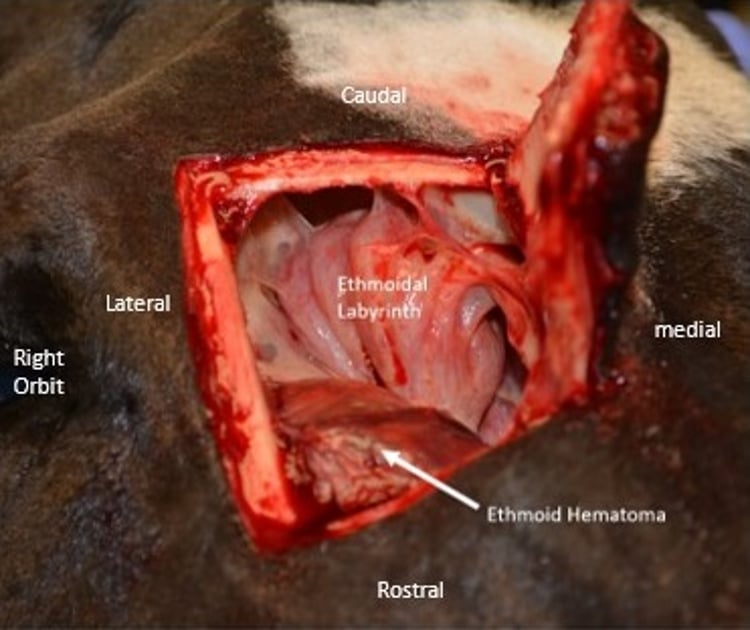
Ethmoid Hematoma
Progressive ethmoid hematoma is a locally destructive, well-encapsulated mass of the nasal passages and/or paranasal sinuses of uncertain etiology. Formation may occur due to hemorrhage of the respiratory submucosa. The mass resembles a tumor in appearance but is not neoplastic in origin. Hematomas typically arise from the ethmoid labyrinth. As they expand, ethmoid hematomas can either extend dorsally into the frontal sinus or ventrally into either the maxillary or sphenopalatine sinus, or they can arise in the sinuses independent of the ethmoturbinates. Most commonly, however, they arise from the ethmoturbinates and extend ventrally into the nasal passage, where they can be viewed endoscopically.

Courtesy of Dr. Claudia Reyner.


Courtesy of Dr. Sameeh M. Abutarbush.
The most common clinical sign is intermittent, unilateral epistaxis. A respiratory noise, reduced air flow from the affected nasal passage, facial deformity, and malodorous breath are possible with large ethmoid hematomas. Middle-aged horses are more commonly affected.
Diagnosis is usually made endoscopically by observing enlargement and/or discoloration (greenish yellow to purple) of the ethmoturbinates or a trickle of blood from the ethmoturbinate region. Radiographs are also performed to investigate potential sinus involvement.
Treatment should be based on size and location of the ethmoid hematoma. Small ethmoid hematomas, originating from the greater ethmoid turbinate and contained within the nasal passage, can may be treated with endoscopically guided intralesional injection of 4% formaldehyde. This will cause regression of the ethmoid hematoma; however, complete resolution will typically require repeat treatment. Neurologic signs have been reported after intralesional formalin injection, associated with communication of the hematoma into the calvarium, so advanced imaging (CT or MRI) of all cases is most ideal, to determine the extent of the lesion prior to treatment. Endoscopic laser ablation with a Nd: YAG has also been reported. Large ethmoid hematomas that extend into the sinus or rostrally within the nasal passage obstructing endoscopic access to the ethmoid turbinates should be treated with sinusotomy. It is important that the origin of the mass be destroyed via radical debridement. Surgical removal can cause appreciable hemorrhage, and the possibility of transfusion should be considered in surgical planning. Horses are treated postoperatively with NSAIDs, antimicrobials, removal of sinus packing at 2-3 days post-op and, sometimes, sinus lavage. Recurrence of the hematoma is common (reported in up to ~40% of cases) and frequent re-evaluation is recommended to detect recurrence early.
Paranasal Sinus Cyst


Courtesy of Dr. Lindsey Boone and Dr. Claudia Reyner.
Sinus cysts are single or loculated fluid-filled cavities with an epithelial lining that can become secondarily infected. They typically develop in the maxillary sinuses and ventral concha and can extend into the frontal sinus. Sinus cysts are typically found in young adult horses but can also occur in older horses. The primary clinical signs are facial deformity, nasal discharge, and partial airway obstruction. Radiographs are more likely to identify a sinus cyst than is endoscopic examination, because they do not extend into nasal passages. Spherical, uniform soft tissue densities and fluid lines within the sinuses are observed radiographically; occasionally, dental distortion, flattening of tooth roots, soft tissue mineralization, and deviation of the nasal septum, frontal bone, or maxilla are seen. Treatment involves surgical removal of the cyst lining via a bone flap (sinusotomy). Care is taken with removal of the cyst lining when adhered to the infraorbital canal or alveoli. Prognosis for complete recovery is good, and recurrence is low. In young horses, facial deformity may regress. Some horses may have a permanent, mild mucoid nasal discharge after surgery.
Neoplasia of the Paranasal Sinuses
In cases of sinus neoplasia, nasal discharge is not always present; when present, it can be either sanguinous or purulent in nature. A foul odor of the breath may be detected due to tissue destruction by the tumor. Diagnosis is made on radiographic evidence of soft tissue opacity within the sinus causing a mass effect and widespread bony lysis. The most commonly diagnosed neoplasm of the paranasal sinuses is squamous cell carcinoma. Fibrosarcoma is another relatively common tumor, and is generally diagnosed in young horses. Neoplasia of the sinuses typically carries a poor prognosis, due to its invasive nature and the extent of disease that is present at the time of diagnosis. Non-invasive neoplasms of the sinuses have been reported (fibroma, osteoma, etc) and carry a more favorable prognosis.
Key Points
Sinus diseases usually cause unilateral nasal discharge (purulent, bloody, or malodorous).
Facial deformity and/or dyspnea can also be associated with sinus cysts or neoplasms.
Treatment is directed toward the primary cause, but secondary sinusitis also usually requires specific therapy with drainage, antimicrobials and lavage.
Surgical treatment of the sinuses can either be performed with sinoscopy or sinusotomy (bone flap) of the frontal or maxillary sinuses.
For More Information
Dixon P & O’Leary. A review of equine paranasal sinusitis: Medical and surgical treatments. Equine veterinary education. 2012. 24 (3): 143–158
O’Leary J & Dixon P. A review of equine paranasal sinusitis. Aetiopathogenesis, clinical signs, and ancillary diagnostic techniques. Equine Veterinary Education. 2011. 23 (3): 148–159
Also see pet health content regarding diseases of the paranasal sinuses in horses.







