




Empyema
Guttural pouch empyema is defined as unilateral or bilateral accumulation of purulent exudate in the guttural pouch. The infection usually develops subsequent to a bacterial (primarily Streptococcus spp) infection of the upper respiratory tract. Rarely, it may develop secondary to trauma involving the guttural pouch or with congenital or acquired stenosis of the guttural pouch opening.

Courtesy of Dr. Bonnie R. Rush.


Courtesy of Dr. Ronald Green.

Courtesy of Auburn University, College of Veterinary Medicine.
Clinical Signs of Guttural Pouch Empyema in Horses
Clinical signs of guttural pouch empyema in horses include intermittent purulent nasal discharge, painful swelling in the parotid area, lymphadenopathy, fever, depression, and anorexia (variably seen). In severe cases, clinical signs can include stiff head carriage and stertorous breathing, dysphagia, or neuropathy.
Diagnosis of Guttural Pouch Empyema in Horses
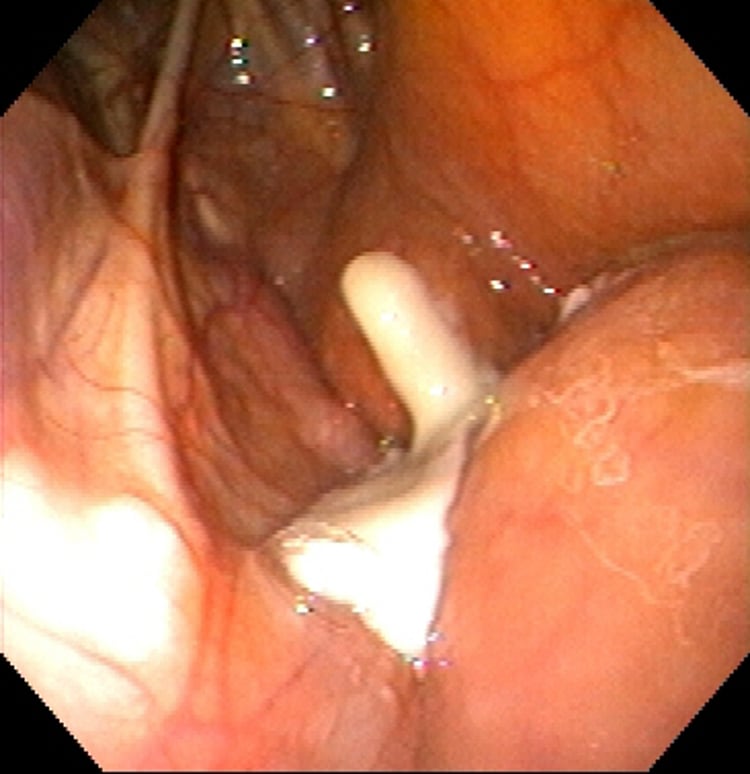
Endoscopic examination of both guttural pouches
Radiographs of the pharynx
Culture or PCR of purulent material to identify Streptococcus equi or other bacterial infection

Courtesy of Dr. Bonnie R. Rush.

Radiographs of the pharynx demonstrate a fluid line in the guttural pouch and may allow identification of an associated retropharyngeal mass. Culture or PCR of purulent material can identify Streptococcus equi or other bacterial infection. Endoscopic examination of both guttural pouches determines whether the condition is unilateral or bilateral. Chondroids (inspissated purulent material) may be identified in chronic cases.
Systemic antimicrobial treatment alone rarely resolves the infection; repeated guttural pouch lavage is necessary. Penicillin gel (prepared using sodium penicillin) can be administered directly into the guttural pouch and may enhance bacterial clearance. Retropharyngeal abscesses can sometimes be resolved by rupturing the abscess into the guttural pouch using an endoscopic blade. If endoscopic rupture into the guttural pouch is unsuccessful, surgical drainage is necessary for retropharyngeal abscessation. Guttural pouch empyema may compress the dorsal pharynx and produce upper airway obstruction. Tracheotomy may be necessary to provide a temporary alternative airway in these cases. Chondroid material in the guttural pouch serves as a source of chronic infection. A small number of chondroids can be removed using an endoscopic snare; however, larger accumulations of exudate, chondroid material, or unresolved retropharyngeal abscesses require surgical drainage.
Guttural Pouch Mycosis
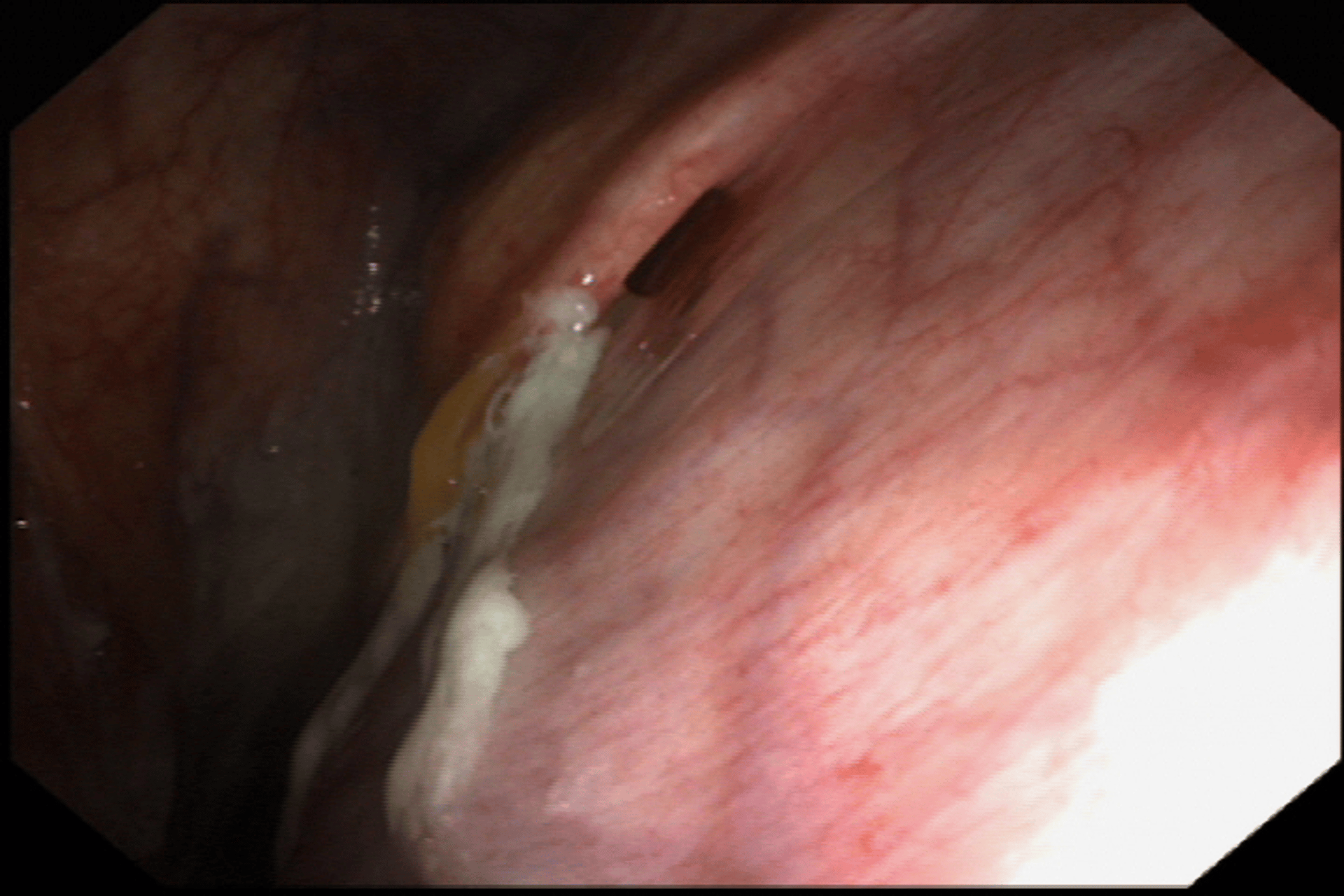
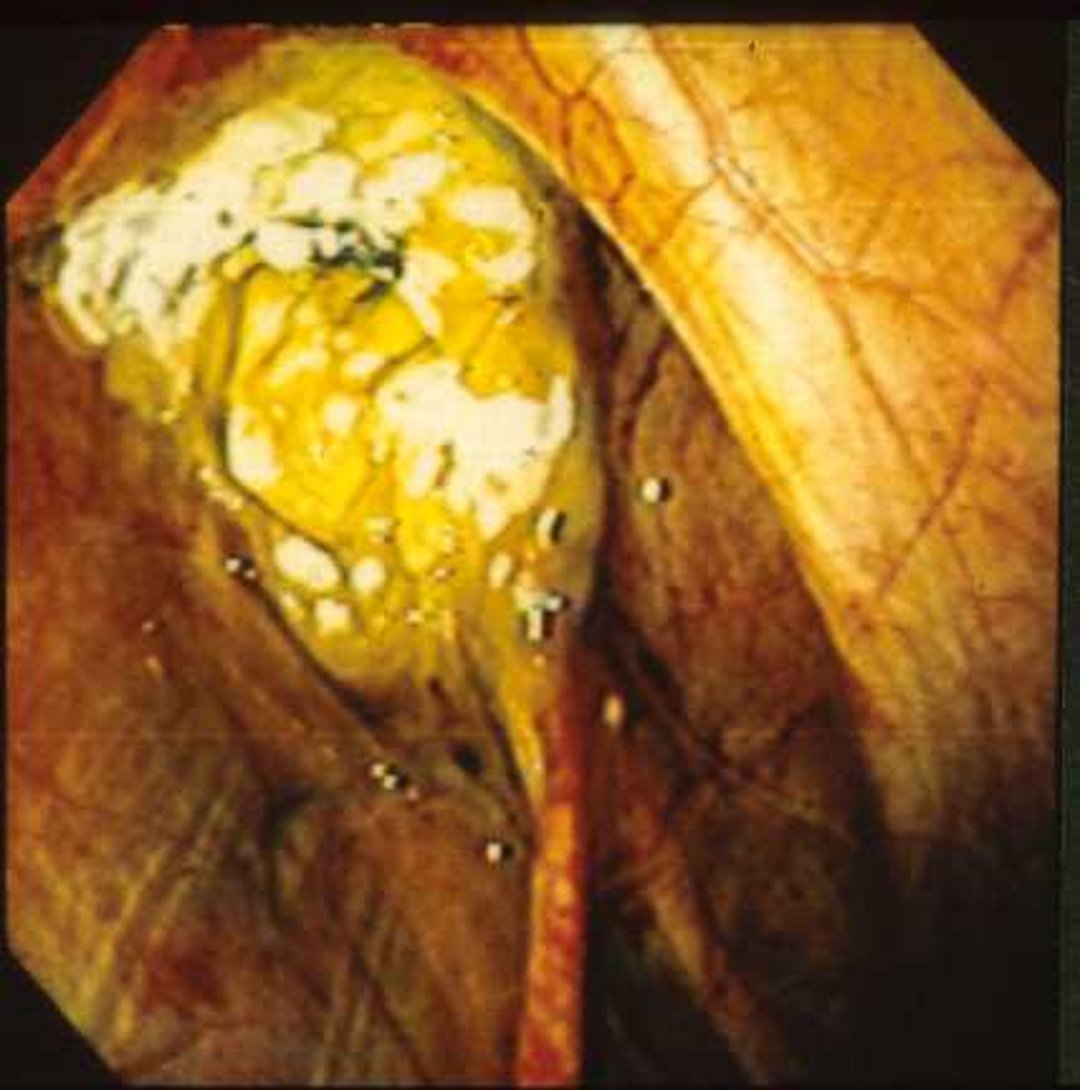
Guttural pouch mycosis is a life-threatening condition, primarily affecting adult horses and resulting in fatal hemorrhage in almost 50% of cases. Mycotic plaques form within the guttural pouch and are typically located on the caudodorsal aspect of the medial guttural pouch, over the internal carotid artery. In some instances, fungal plaques may be multiple or diffuse. Plaques can also be identified in the lateral guttural pouch over the external maxillary artery (~30% of cases) and, more rarely, over the external carotid artery. The most common fungal organism associated with guttural pouch mycosis is Aspergillus spp.


Courtesy of Dr. Sameeh M. Abutarbush.

Courtesy of Dr. Bonnie R. Rush.
The condition is clinically occult until the fungal plaques damage the cranial nerves and arteries within the guttural pouch. The most common sign is epistaxis, due to fungal erosion of the wall of either the internal carotid artery (most cases) or branches of the external carotid artery. Hemorrhage is spontaneous and severe, and repeated bouts may precede a fatal hemorrhagic episode. Dysphagia, Horner syndrome, dorsal displacement of the soft palate, and facial paralysis may also develop in response to fungal damage to cranial nerves and the sympathetic nerve that superficially traverse the guttural pouch. Dysphagia is a poor prognostic indicator and is highly correlated with non-survival.
Medical treatment can be expensive and prolonged (weeks), consisting of topical and systemic antifungal treatment. Variable success is reported. Additional supportive or medical treatment may be needed depending on the severity of disease or blood loss, and associated neurologic abnormalities. Surgical occlusion of the affected arteries both proximal and distal to the lesion can be attempted in combination with medical treatment. Options for occlusion include ligation of affected vessels, placement of a balloon-tipped catheter or fluoroscopic-guided transarterial coil embolism. Vessel occlusion is primarily performed to decrease the risk of fatal hemorrhage but may also arrest fungal plaque growth.
Guttural Pouch Tympany
Guttural pouch tympany involves distension of one or both guttural pouches with air. The condition is seen in horses ranging from birth to 1.5 years of age and is more common in fillies than in colts. A breed predilection has been proposed for Arabian and Paint horses and a genetic basis of disease has been identified in Arabians and German Warmblood breeds, including a gender-specific quantitative trait locus in Warmbloods. The exact cause for guttural pouch tympany is unknown, but the most common explanation is that malformation or dysfunction in the mucosal flap (plica salpingopharyngea) which forms the pharyngeal orifice to the guttural pouch, creating a one-way valve and trapping air within the affected guttural pouch. In some cases, it is thought that the condition may occur secondary to upper airway respiratory disease and associated inflammation affecting the mucosal flap.


Courtesy of Auburn University College of Veterinary Medicine.
Characteristic clinical signs of tympany include a nonpainful, fluctuant swelling of the parotid region overlying the affected pouch. Tympany is usually unilateral; however, bilateral cases have been reported. Bilateral swelling may also result from severe unilateral tympany. Breathing may become stertorous in severely affected animals. Dysphagia, dyspnea, secondary empyema, and aspiration pneumonia may occur in more complicated cases. Diagnosis is based on clinical signs and radiographic examination of the skull. Endoscopy may also be useful to confirm diagnosis, rule out other upper airway or guttural pouch disorders, and facilitate distinction between unilateral and bilateral disease.
In cases where upper respiratory tract inflammation is identified, conservative medical management with NSAIDs and broad-spectrum antimicrobial treatment may be successful. Temporary relief can be obtained via decompression of air using a percutaneous needle or catheter placed through the pharyngeal opening to the guttural pouch. Surgical fenestration of the septum between the affected guttural pouch and the normal one can be performed, to allow air in the abnormal guttural pouch to pass to the normal side and be expelled into the pharynx. Repeated surgery may be needed in some cases. Fenestration is generally unsuccessful with bilateral tympany. The postoperative prognosis is good in cases without secondary complications. Alternatively, long-term (2-6 weeks) placement of Foley catheters into the opening of each guttural pouch, exiting the nares, can result in remodeling at the plica fold, with permanent resolution of tympany once the catheters are removed.







