

Tsetse-transmitted Trypanosomiasis
Tsetse-transmitted trypanosomiasis refers to a group of diseases caused by protozoa of the genus Trypanosoma and affects all domesticated animals. The major veterinary species are T congolense, T vivax, T brucei brucei, and T simiae. T brucei rhodesiense and T brucei gambiense are zoonotic, with people as the predominant host. For the animals mainly affected by these tsetse-transmitted trypanosomes and the geographic areas where tsetse-transmitted trypanosomiasis occurs, see Table: Tsetse-transmitted Trypanosomes.
Tsetse-transmitted Trypanosomes
Trypanosoma spp | Animals Mainly Affected | Major Geographic Distribution |
|---|---|---|
T congolense | Cattle, sheep, goats, dogs, pigs, camels, horses, most wild animals | South and eastern Africa |
T vivax | Cattle, sheep, goats, camels, horses, various wild animals | Africa, Central and South America, West Indiesa |
T brucei brucei | All domestic and various wild animals; most severe in dogs, horses, cats | South and eastern Africa |
T brucei rhodesiense | Cattle, wild hooved stock, people | South and eastern Africa |
T brucei gambiense | Cattle, sheep, goats, people | West and central Africa, including Uganda |
T simiae | Domestic and wild pigs, horses, camels | South and eastern Africa |
a In non-tsetse areas, transmission is by biting flies. | ||
Cattle, sheep, and goats are infected, in order of importance, by T congolense, T vivax, and T brucei brucei. In pigs, T simiae is the most important. In dogs and cats, T brucei is probably the most important. It is difficult to assign an order of importance for horses and camels. T vivax is found outside tsetse-infested areas of sub-Saharan Africa, carried mechanically by biting flies.
The trypanosomes that cause tsetse-transmitted trypanosomiasis (sleeping sickness) in people, T brucei rhodesiense and T brucei gambiense, closely resemble T brucei brucei, and suitable precautions should be taken when working with such isolates. Domestic animals act as reservoirs of human infections.
Transmission and Epidemiology of Trypanosomiasis in Animals
Most tsetse transmission is cyclic and begins when blood from a trypanosome-infected animal is ingested by the fly. The trypanosome alters its surface coat, multiplies in the fly, then alters its surface coat again, and becomes infective. T brucei spp migrate within the tsetse from the gut and eventually to the salivary glands; the cycle for T congolense stops at the hypopharynx, and the salivary glands are not invaded; the entire cycle for T vivax occurs in the proboscis. Therefore, the location within the tsetse can be useful in identifying the parasite species. The animal-infective form in the tsetse salivary gland is referred to as the metacyclic form. The life cycle in the tsetse may be as short as 1 week with T vivax or extend to a few weeks for T brucei spp.
Tsetse flies (genus Glossina) are restricted to Africa from about latitude 15°N to 29°S. The 3 main species inhabit relatively distinct environments: G morsitans usually is found in savanna country, G palpalis prefers areas around rivers and lakes, and G fusca lives in high forest areas. All 3 species transmit trypanosomes, and all feed on various mammals.
Mechanical transmission can occur through tsetse or other biting flies. In the case of T vivax, Tabanus spp and other biting flies seem to be the primary mechanical vectors outside tsetse-endemic areas, as in Central and South America. Mechanical transmission requires only that blood containing infectious trypanosomes be transferred by bite from one animal to another.
Pathogenesis of Trypanosomiasis in Animals
Infected tsetse inoculate metacyclic trypanosomes into the skin of animals, where the trypanosomes reside for a few days and cause localized inflammation (chancres). They enter the lymph and lymph nodes, then the bloodstream, where they divide rapidly by binary fission. In T congolense infection, the organisms attach to endothelial cells and localize in capillaries and small blood vessels. T brucei species and T vivax invade tissues and cause tissue damage in several organs.
The immune response is vigorous, and immune complexes cause inflammation, which contributes to fever and other signs and lesions of the disease. Antibodies against the surface-coat glycoproteins kill the trypanosomes. However, trypanosomes have a large family of genes that code for variable surface-coat glycoproteins that are switched in response to the antibody response, evading immunity. This antigenic variation results in persistence of the organism. Antigenic variation has prevented development of a protective vaccine and permits reinfections when animals are exposed to a new antigenic type.
Clinical Findings and Lesions of Trypanosomiasis in Animals
The severity of trypanosomiasis varies with species and age of the animal infected and species of trypanosome involved. The incubation period is usually 1–4 weeks. The primary clinical signs are intermittent fever, anemia, and weight loss. Cattle usually have a chronic course with high mortality, especially if there is poor nutrition or other stress factors. Ruminants may gradually recover if the number of infected tsetse flies is low; however, stress results in relapse.
Necropsy findings vary and are nonspecific. In acute, fatal cases, extensive petechiation of the serosal membranes, especially in the peritoneal cavity, may occur. Also, the lymph nodes and spleen are usually swollen. In chronic cases, swollen lymph nodes, serous atrophy of fat, and anemia are seen.
Diagnosis of Trypanosomiasis in Animals
Clinical evaluation
Serologic testing

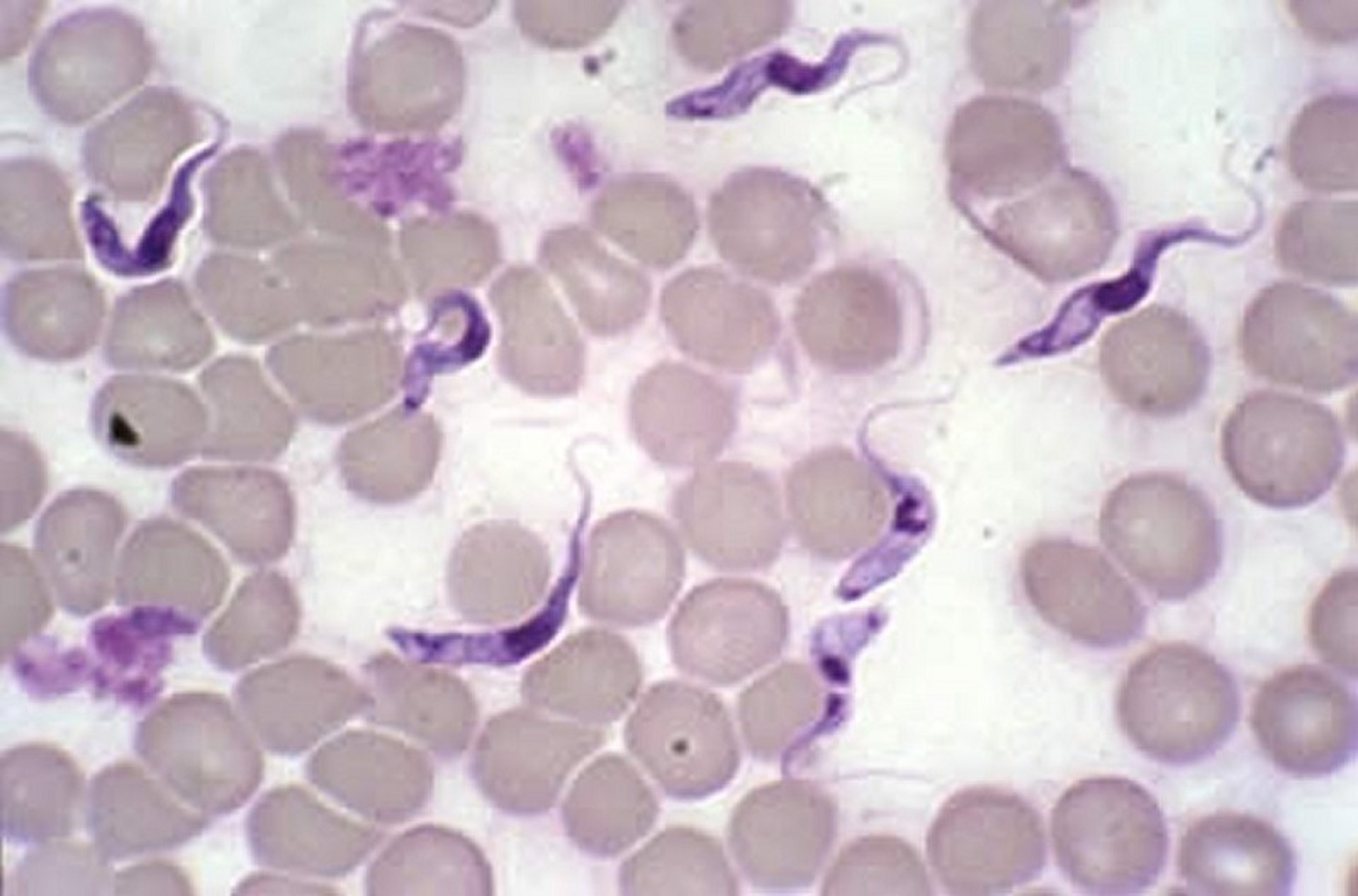
Trypanosoma vivax, Giemsa-stained blood smear of an infected cow.
Courtesy of Dr. Corrie Brown.
A presumptive diagnosis of trypanosomiasis is based on finding an anemic animal in poor condition in an endemic area. Confirmation depends on demonstrating trypanosomes in stained blood smears or wet mounts. The most sensitive rapid method is to examine a wet mount of the buffy coat area of a PCV tube after centrifugation, looking for motile parasites. Other infections that cause anemia and weight loss, such as babesiosis, anaplasmosis, theileriosis, and haemonchosis, should be excluded by examining a stained blood smear.
Various serologic tests measure antibody to trypanosomes, but their use is more suitable for herd and area screening than for individual diagnosis. Rapid agglutination tests to detect circulating trypanosome species-specific antigens in peripheral blood are available for both individual and herd diagnosis, although their reliability remains varied. Molecular techniques for trypanosome detection and differentiation have been developed, but they are not generally available for routine field use.
Treatment and Control of Trypanosomiasis in Animals
Chemotherapeutics
Reduction of tsetse fly populations
Several drugs can be used for treatment ( see Table: Drugs Commonly Used for Trypanosomiasis in Domestic Animals) of trypanosomiasis. Most have a narrow therapeutic index, which makes administration of the correct dose essential. Drug resistance occurs and should be considered in refractory cases.
Drugs Commonly Used for Trypanosomiasis in Domestic Animals
Drug | Animal | Trypanosoma | Main Action | Administration Route(s) | Dosage (mg/kg) |
|---|---|---|---|---|---|
Diminazene aceturate | Cattle | vivax, congolense, brucei | Curative | IM, SC | 3.5–7 |
Homidium bromide | Cattle | vivax, congolense, brucei | Curative, some prophylactic activity | IM (deep), IV (sheep, goats, pigs) | 1 |
Homidium bromide | Equids | vivax | Curative, some prophylactic activity | IV | 1 |
Homidium chloride | Equids | vivax | Curative, some prophylactic activity | IV | 1 |
Isometamidium chloride | Cattle | vivax, congolense | Curative and prophylactic | IM (deep) | 0.25–1 |
Quinapyramine sulfate | Horses, camels, pigs, dogs | vivax, congolense, brucei, evansi, equiperdum, simiae | Curative | SC | 3–5 |
Quinapyramine dimethylsulfate | Horses, camels, pigs, dogs | vivax, congolense, brucei, evansi, equiperdum, simiae | Prophylactic | SC | 3–5 |
Suramin | Horses, camels, dogs | brucei, evansi | Curative, some prophylactic activity | IV | 10 |
Melarsomine dichlorhydrate | Camels | evansi | Curative | SC, IM | 0.25–0.5 |
Control of trypanosomiasis can be exercised at several levels, including eradication of tsetse flies and use of prophylactic drugs. Tsetse flies can be partially controlled by frequent spraying and dipping of animals, aerial and ground spraying of insecticides on fly-breeding areas, use of insecticide-impregnated screens and targets, bush clearing, and other habitat removal methods. The Sterile Insect Technique (SIT) has been used with success in Zanzibar and may be used in other area-wide control operations after suppression of tsetse populations by insecticides. There is renewed international interest in large-scale tsetse eradication through the Pan African Tsetse and Trypanosomiasis Eradication Campaign (PATTEC) supported by the African Union. Animals can be given drugs prophylactically in areas with a high population of trypanosome-infected tsetse. Drug resistance must be carefully monitored by frequent blood examinations for trypanosomes in treated animals.
Several breeds of cattle and water buffalo have been identified that have innate resistance to trypanosomiasis and could play a valuable role in reducing the impact of the disease in these areas. However, resistance may be lost because of poor nutrition or heavy tsetse challenge.
Control is ideally achieved by combining methods to reduce the tsetse challenge and by enhancing host resistance with prophylactic drugs.
Surra
(Trypanosoma evansi Infection)
Surra is usually transmitted by other biting flies that are found within and outside tsetse fly areas. It is found in North Africa, the Middle East, Asia, the Far East, and Central and South America. The distribution of T evansi in Africa extends into the tsetse areas, where differentiation from T brucei is difficult. It is essentially a disease of camels and horses, but all domestic animals are susceptible. The disease can be fatal, particularly in camels, horses, and dogs. T evansi in other animals appears to be nonpathogenic, and these animals serve as reservoirs of infection.
Transmission is primarily by biting flies, probably resulting from interrupted feedings. A few wild animals are susceptible to infection and may serve as reservoirs.
Pathogenesis, clinical findings, lesions, diagnosis, and treatment for surra are similar to those of the tsetse-transmitted trypanosomes.
Dourine
Dourine is a chronic venereal disease of horses that is transmitted during coitus and caused by T equiperdum. The disease is recognized on the Mediterranean coast of Africa and in the Middle East, southern Africa, and South America; distribution is probably wider.
Signs of dourine may develop over weeks or months. Early signs include mucopurulent discharge from the urethra in stallions and from the vagina in mares, followed by gross edema of the genitalia. Later, characteristic plaques 2–10 cm in diameter appear on the skin, and the horse becomes progressively emaciated. Mortality in untreated cases is 50%–70%.
Demonstration of trypanosomes from urethral or vaginal discharges, skin plaques, or peripheral blood is difficult unless the material is centrifuged. Infected horses can be detected with the complement fixation test but only in areas where T evansi or T brucei are not found because they have common antigens. An ELISA test may become available for diagnosis.
In endemic areas, horses may be treated ( see Table: Drugs Commonly Used for Trypanosomiasis in Domestic Animals). When eradication is required, strict control of breeding and elimination of stray horses has been successful. Alternatively, infected horses may be identified using the complement fixation test; euthanasia is mandatory.
Chagas Disease
(Trypanosoma cruzi Infection)
Chagas disease, or American trypanosomiasis, is a zoonotic, vector-borne disease transmitted by triatomine bugs and caused by T cruzi. All mammals are considered susceptible to infection, with infection demonstrated in >100 mammalian species. Avian species are not susceptible. The disease is best recognized in dogs and people, with dogs serving as a major domestic reservoir. Domestic pigs and cats can also be infected, but their role as reservoirs for human infection is limited. Wildlife reservoirs include opossums, armadillos, raccoons, woodrats, and nonhuman primates.
Transmission and Epidemiology of Chagas Disease in Animals
Chagas disease is endemic in 21 countries of South America, Central America, and Mexico, and is increasingly reported in the southern USA. Chagas was once confined to the Americas, but human and animal migration has resulted in distribution to Europe, where it is an emerging disease of Spain, Switzerland, France, Italy, Germany, and England. Seropositivity in dogs in endemic regions can vary from 5%–92%. In some areas such as Venezuela, the seropositivity of dogs is similar to that of people, whereas in other areas, such as Campeche, Mexico, seropositivity can be higher in dogs than in people.
The nocturnal and hematophagous triatomine insects of the Triatoma, Rhodnius, and Panstrongylus genera serve as vectors for T cruzi. Common names include the “kissing bug,” “assassin bug,” “cone-nosed bug,” “vinchuca,” “chinche,” and “barbeiro." There are >130 species of triatomines in the Americas, and most are considered competent vectors. Insects take an infected blood meal ingesting extracellular T cruzi trypomastigotes. These differentiate in the midgut to epimastigotes and divide. Epimastigotes travel to the hindgut, where they differentiate back into metacyclic trypomastigotes. Infective metacyclic trypomastigotes are shed in insect feces.
In insectivorous animals, including dogs, consumption of infected bugs or materials contaminated with infected triatomine feces is a major mode of transmission. Remarkably, the opossum (Didelphis species) is a unique host for T cruzi, because the parasite can complete its entire life cycle without the need for a vector. T cruzi maturation occurs in the anal odoriferous glands, and infective trypomastigotes can be shed in feces or urine and ingested. Additional methods of transmission include transplacentally or via blood transfusions and organ transplant.
Pathogenesis of Chagas Disease in Animals
Once metacyclic trypomastigotes enter the bloodstream, they actively invade many cell types, exiting the parasitophorous vacuole and becoming nonflagellated amastigotes. Intracellular amastigotes divide every 15–18 hours for 5–6 days. T cruzi transforms back into trypomastigotes and lyses the cell. Released trypomastigotes invade new cells. T cruzi has a tropism for cardiac and smooth muscle but can be found in numerous other tissues.
Clinical Findings and Lesions of Chagas Disease in Animals
Chagas disease is divided into acute and chronic phases, with the chronic phase further subdivided into latent and symptomatic chronic disease. Incubation ranges from 5–42 days before acute disease. Acute infections may be asymptomatic or consist of nonspecific febrile illness with a chancre at the site of parasitic entry. Dogs may also present with regional or generalized lymphadenopathy, anorexia, lethargy, vomiting, diarrhea, and hepatomegaly or splenomegaly. Rarely, acute clinical myocarditis is seen. Parasitemia peaks 2–3 weeks after infection and dissipates after the first month as the organism moves to predominantly tissue-borne disease.
The latent phase can last for months to years. Chronic disease symptoms can include generalized weakness or sudden death. Symptomatic dogs commonly present with right-side congestive heart failure. This can progress to myocarditis, with arrhythmias and bilateral cardiac dilation. Histologic examination of cardiac muscle may contain unruptured pseudocysts without inflammation or contain ruptured pseudocysts with lymphocytic, monocytic, and/or neutrophilic inflammation. Death secondary to heart failure is common.
Diagnosis of Chagas Disease in Animals
Direct examination of blood smear
Antibody testing
Diagnosis of Chagas disease can be made by visualization of the organism, detection of DNA, or antibody detection. Parasitemia during the acute phase allows for detection on a microscopy of a routine peripheral blood smear. Although samples can be tested for T cruzi DNA by PCR or cultured, these diagnostic tests are uncommon in the field. On Giemsa stain, T cruzi is an extracellular, C-shaped protozoan with a single flagellum.
Antibody testing is of primary importance during the chronic phase. Whole blood, plasma, or serum can be submitted. Testing methodologies include immunochromographic “dipstick,” immunofluorescent antibody, or ELISA. Notably, cross-reaction with antibodies to Leishmania species, another trypanosomatid, can occur. Because of cross-reactivity of serologic tests, testing with at least two different methodologies or antigens is recommended. Additionally, cardiac tissue in the chronic phase can be analyzed by PCR for T cruzi DNA or by immunohistochemical analysis for amastigotes.
Treatment and Control of Chagas Disease in Animals
Chemotherapeutics
Vector control
Benznidazole is the drug of choice for treatment for Chagas disease, but nifurtimox can also be used. In dogs, benznidazole is administered at 5–10 mg/kg/day, PO, for 2 months. In the USA, both of these drugs lack FDA approval, and their use requires permission from the CDC as investigational protocols. Symptomatic treatment for heart failure and arrhythmias is also recommended.
No vaccine for Chagas disease is available; thus, control focuses on preventing disease transmission. Vector control methods include applying pesticides to eliminate triatomine vectors and decreasing vector attraction to dwellings at night by turning off outdoor lighting. Breeding of positive bitches is discouraged. Screening of blood donors is recommended. To avoid iatrogenic transmission, disinfection with 10% bleach or 70% ethanol is suggested for contaminated surfaces. Dead infected insects can remain a source of infective T cruzi for up to 6 days at 10°C or up to 2 months at 26°–30°C.
Nonpathogenic Trypanosomes
Trypanosoma theileri or markedly similar trypanosomes have been detected in peripheral blood from cattle on every continent. Infection with similar trypanosomes also has been detected in domestic and wild buffalo and various other wild ungulates. In the few areas studied, transmission is by contamination after a cycle of development in species of tabanid flies. Although most parasitemias are subpatent, the trypanosomes may be seen in a blood smear being examined for pathogenic protozoa or in a hemocytometer chamber. Pathogenicity has never been proved experimentally.
T melophagium of sheep also has a worldwide distribution and is transmitted by the sheep ked. T theodori, reported in goats, may be a synonym for the same trypanosome.
For More Information





