

Corynebacterium pseudotuberculosis is a common cause of infection in horses and cattle that leads to chronic abscesses along lymphatic chains (lymphangitis) on the limbs of horses and cattle, occasionally on the abdomen, and most commonly in the pectoral region of the horse. Diagnosis is confirmed by isolation of the bacteria from lesions. Longterm antimicrobial treatment and drainage of abscesses are required; however, the disease is often chronic, and internal infections have a 30%–40% mortality rate.
In horses, Corynebacterium pseudotuberculosis causes ulcerative lymphangitis (an infection of the lower limbs; see ) and chronic abscesses in the pectoral region, ventral abdomen, and preputial or mammary regions. It is a common and economically important infectious disease of horses and cattle worldwide.


Equine ulcerative lymphangitis. Note that the lesions follow a trail distally coinciding with the lymphatic chains of the distal limbs.
Courtesy of Dr. Sharon Spier.
In cattle, C pseudotuberculosis most commonly causes cutaneous excoriated granulomas. Large, ulcerative skin lesions resembling infected granulation tissue and lymphangitis may occur in 2%–5% of cows (see ). Location on the animal varies but is often associated with skin trauma. Healing often occurs without treatment or with limited topical treatment in 2–4 weeks. Abortion and mastitis may also occur.


Bovine ulcerative lymphangitis. A chain of abscesses in the hind limb that follow the lymphatics is one form of external infection.
Courtesy of Dr. J. Glenn Songer.
In cattle, visceral involvement has been reported with C pseudotuberculosis infection, but it occurs much less commonly than in horses. Disease has also been reported in camels, alpacas, llamas, and buffalo.
Pathogenesis and Clinical Findings of Lymphangitis of Horses and Cattle
The onset of ulcerative lymphangitis in horses is variable and usually manifests as painful inflammation, nodules, and ulcers, especially in the region of the lower limb, or lameness and edematous swelling can extend up the entire limb. The exudate is odorless, thick, tan, and blood tinged. Usually, only one leg is involved. If the animal is not treated aggressively with antimicrobials, lesions and swelling usually progress and become chronic with relapses.
C pseudotuberculosis infection in horses occurs at any time of the year. However, peak incidence of disease is during the summer and fall, when flying insects are present. Infection results in abscessation of the pectoral region (see ) or ventral abdominal region, with secondary dissemination to internal organs (see ).


Typical pectoral abscess due to lymphangitis in a horse, with flies present. Flies act as vectors of the disease.
Courtesy of Dr. Sharon Spier.

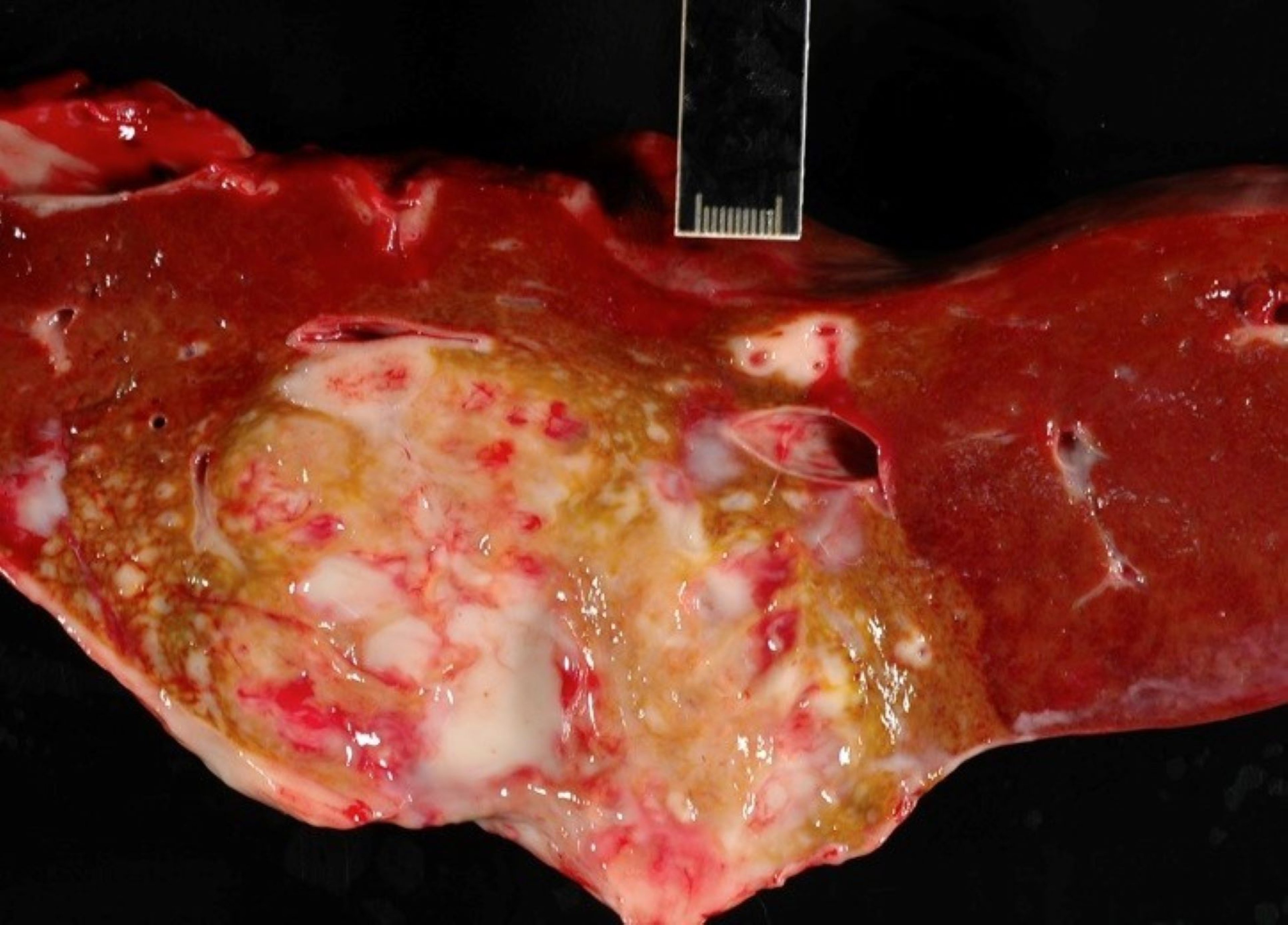
Liver abscess from a necropsy specimen of a horse with lymphangitis.
Courtesy of Dr. Sharon Spier.
Clinical signs of C pseudotuberculosis infection in horses and cattle include the following:
diffuse or localized swellings
ventral pitting edema
ventral midline dermatitis
lameness
draining abscesses or tracts
fever
weight loss
depression
In addition, anemia, leukocytosis, neutrophilia, hyperfibrinogenemia, and increased concentrations of serum amyloid A (SAA) and hyperglobulinemia (indicative of inflammation) are usually present. A marked or prolonged fever, anorexia, or weight loss suggests deep or recurring abscesses, internal abscessation, or systemic infection with abortion.
Abscesses can be large, up to 20 cm in diameter before rupturing, and take weeks to months to resolve. Weight loss, colic, splinted abdomen, or lethargy may be clinical signs of internal abscesses.
Dermatitis lesions are painful and mildly pruritic with alopecia, exudation, crusting, and ulceration. Nonhealing abscesses or wounds may be concurrently affected with cutaneous habronemiasis (“summer sores”).
C pseudotuberculosis bacteria enter via skin wounds by arthropod vectors such as stable flies, horn flies, and house flies, or by contact with contaminated fomites or soil.
Diagnosis of Lymphangitis of Horses and Cattle
Bacterial culture of pus from external abscesses
Abdominal ultrasonographic examination to detect internal infection or abscesses, clinicopathologic evidence of inflammation, and serologic testing for internal infection
PCR testing of abdominal fluid for C pseudotuberculosis
Isolation of C pseudotuberculosis from lesions is necessary to confirm a diagnosis of infection. In all forms of lymphangitis in horses, samples for culture include aspirates of abscesses, swabs of purulent exudate beneath crusts associated with folliculitis, and punch biopsies.
Differential diagnoses of C pseudotuberculosis infection include the following:
pyoderma, abscesses, or lymphangitis due to other bacteria (eg, Staphylococcus aureus, Rhodococcus equi, Streptococcus spp, or Dermatophilus spp)
equine cryptococcosis
North American blastomycosis
Ultrasonography of the abdomen and thorax is useful for detecting internal C pseudotuberculosis infection of the liver, spleen, kidneys, or lungs. Ultrasonography is also useful for detecting and draining deep abscesses that result in lameness, particularly in the triceps musculature of horses.
Transtracheal aspirates are required to confirm pneumonia due to C pseudotuberculosis. In horses, serologic testing with the synergistic hemolysis inhibition (SHI) test, which detects IgG to the phospholipase D exotoxin, is a useful adjunct for diagnosis of internal infection in the absence of external infection. By itself, serologic testing is not sufficient to diagnose infection.
Treatment of Lymphangitis of Horses and Cattle
Lancing and drainage of external abscesses
Longterm antimicrobials for ulcerative lymphangitis, limb infection, and internal infection
Fly control
Lymphangitis and internal infection should be treated with longterm antimicrobials (a minimum of 1 month duration or as directed by follow-up ultrasonography). The organism is susceptible to many commonly administered antimicrobials (1); however, antimicrobial treatment of uncomplicated external abscesses may prolong the disease by delaying abscess maturation.
External abscess swellings are treated with hot packs, poultices, or hydrotherapy until they rupture or are drained surgically. Abscesses are lanced and flushed with dilute antiseptic solutions. Deep abscesses in the triceps or quadriceps region require ultrasonography to guide placement of an indwelling drain.
Systemic administration of phenylbutazone or flunixin meglumine relieves pain and swelling. General supportive and nursing care is indicated.
If treatment for lymphangitis is successful, the swelling gradually recedes over days or weeks. Internal infection with C pseudotuberculosis has a 30%–40% mortality rate in horses, even with appropriate treatment.
Severe or untreated lymphangitis cases often become chronic, leading to fibrosis and induration of the leg.
Isolation of infected animals, comprehensive fly control including insect growth regulators, and good sanitation are recommended for prevention of lymphangitis. A conditionally licensed bacterin or toxoid is currently available for horses.
Key Points
Corynebacterium pseudotuberculosis is a gram-positive, soil-dwelling bacterium.
C pseudotuberculosis infection occurs worldwide and is increasing in frequency in North America.
In horses, external abscesses involving the ventral abdomen and pectoral region are the most common signs of C pseudotuberculosis infection.
In horses, internal infection and ulcerative lymphangitis require longterm antimicrobial treatment.
Measures to control flies and isolate animals are recommended for preventing new cases.
For More Information
Also see Pet Health content regarding lymphangitis in horses.
References
Rhodes DM, Magdesian KG, Byrne BA, Kass PH, Edman J, Spier SJ. Minimum inhibitory concentrations of equine Corynebacterium pseudotuberculosis isolates (1996–2012). J Vet Intern Med. 2015;29(1):327-332. doi:10.1111/jvim.12534





