

Because of the liver's large functional reserve and ability to regenerate, hepatic injury must be considerable or chronic and recurrent to cause overt hepatic dysfunction or failure.
Active liver injury typically is associated with increased circulating liver enzyme activities.
Release of cytosolic transaminases (ALT, AST) acutely reflects altered cell membrane permeability. This may reflect a reversible phenomenon of membrane blebbing.
Increases in alkaline phosphatase (ALP) and gamma-glutamyl transferase (GGT) reflect gene-transcriptional responses (enzyme induction), direct injury to bile duct epithelium (cholangiocytes), or cholestasis associated with injury to biliary elements.
The liver is predisposed to secondary injury from systemic disorders because of its sentinel position between the systemic circulation and GI tract and because of an abundant population of macrophages (ie, Kupffer cells [resident hepatic macrophages]; liver sinusoidal endothelial cells [LSECs]).
Macrophage phagocytosis removes a multitude of substances (particulate debris and endotoxins). Such phagocytic activity has the potential to activate hepatic Kupffer cells and LSECs, initiating release of numerous inflammatory cytokines, leading to local tissue damage and recruitment of inflammatory infiltrates.
LSECs are vital for a spectrum of metabolic, secretory, storage, clearance, scavenging, and immunologic functions.

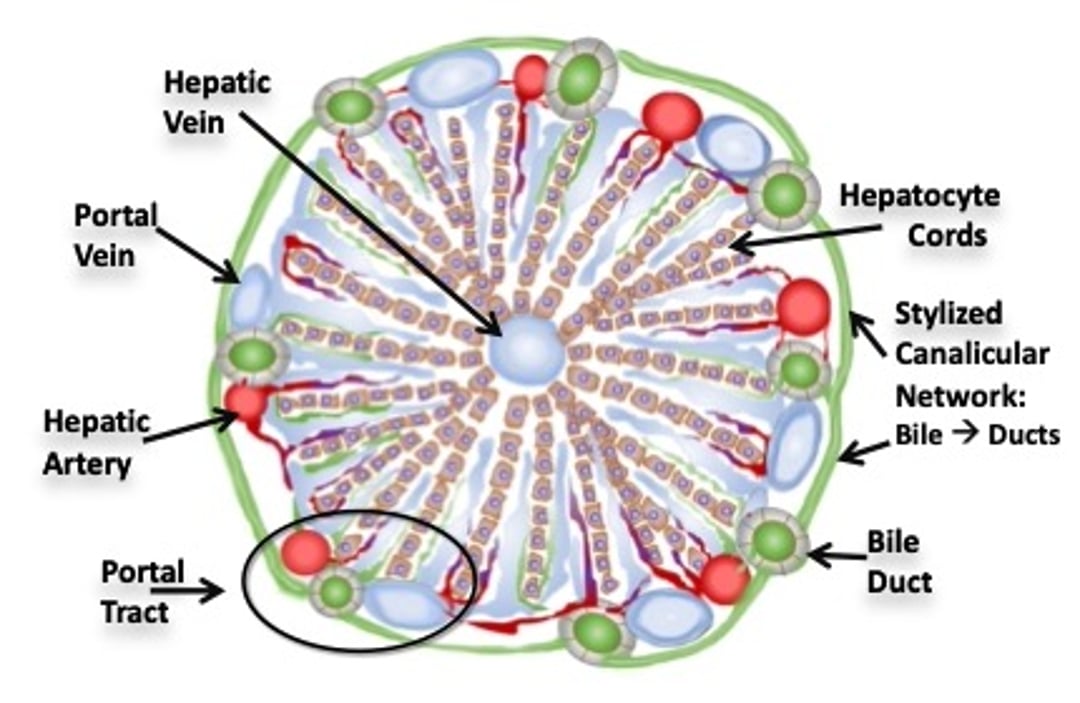
Schema of a classical hepatic lobule in cross-section. Linear cords of hepatocytes are oriented radially surround the hepatic vein and extend to portal tracts. Portal tracts display profiles of hepatic artery, portal vein, and bile duct. Most perfusion is venous (blue shading), with less arterial perfusion (red shading). These intermix in sinusoids. Tiny arterial branches extend to the bile ducts (peribiliary arterial plexus). The hepatic vein is most vulnerable to hypoxic or ischemic events receiving the last sinusoidal distribution of blood. Canalicular conduits (not shown) are located at the intercellular juxtaposition of hepatocytes (see Hepatic lobule, zones). Green shading in areas other than well-defined bile ducts reflects bile flow in canalicular and cholangiolar conduits.
Courtesy of Dr. Sharon Center.
Because of their broad repertoire of activities, these cells play a central role in the pathogenesis of acute and chronic liver injury and development of liver fibrosis. The considerable spectrum of hepatic metabolism and detoxification escalates risk of generating injurious products or toxic adducts.
In the presence of the primed hepatic surveillance system (ie, Kupffer and LSEC populations), such injuries can be escalated or exaggerated, especially those provoked by toxins. This is particularly notable in centrilobular regions expressing cytochrome P450 enzymes, because these orchestrate a myriad of bioactivating and detoxication reactions that generate noxious metabolites and oxidative radicals. Hepatocytes in this region also are more easily injured by systemic hypoxia, being the last recipients of sinusoidal blood flow.
Accumulation of transition metals (eg, copper or iron) in centrilobular regions can also foster oxidative injury, aggravating damage incurred from unrelated insults. The propensity of dogs to accumulate copper in centrilobular hepatocytes imposes high risk for a "two-hit" injury phenomenon (primary injury event augmented by copper-mediated oxidative damage).





