

Infectious keratoconjunctivitis (IKC; pinkeye) of cattle, sheep, and goats is characterized by blepharospasm, conjunctivitis, lacrimation, and varying amounts of corneal opacity. The most common manifestation of IKC in cattle is infectious bovine keratoconjunctivitis (IBK; bovine pinkeye), for which the initial key clinical sign is central corneal ulceration. Microbiological, cytological, and/or molecular testing of samples collected from affected eyes can help identify specific organisms associated with IKC or IBK. Treatment generally consists of administering systemic and/or topical antimicrobials, along with providing other supportive care, depending on disease severity. Prevention relies on controlling risk factors. For IBK, commercial and autogenous vaccines exist, but their efficacy is vigorously debated.
Infectious keratoconjunctivitis (IKC; pinkeye) of cattle, sheep, and goats is a common ocular condition characterized by blepharospasm, conjunctivitis, lacrimation, and varying amounts of corneal opacity. In cattle, the most common manifestation is infectious bovine keratoconjunctivitis (IBK; bovine pinkeye). Corneal ulceration is the key defining clinical sign of IBK; however, it is not a required clinical sign for diagnosing IKC in small ruminants.
Animals with IKC can present at any age, but juveniles are the most commonly affected.
In cattle, IBK can occur at any time of year; however, outbreaks are typically associated with warmer periods, when exposure to risk factors is the greatest. In small ruminants, IKC commonly develops during the summer in association with animals attending fairs and livestock shows.
Risk factors for IKC and IBK, as well as associated infectious agents, are listed in the table .
Infectious Keratoconjunctivitis Risk Factors and Infectious Agents
Infectious Keratoconjunctivitis (IKC) | Infectious Bovine Keratoconjunctivitis (IBK) |
|---|---|
RISK FACTORS | |
Infectious agents (see below) Commingling during shipping or at shows, sales, and auctions | Ultraviolet solar irradiation Flies Dust Mechanical irritation (awns from plants such as foxtail grasses) Trace mineral deficiencies (copper, selenium) Infectious agents (see below) |
INFECTIOUS AGENTS | |
Chlamydophila pecorum Mycoplasma spp (notably Mycoplasma conjunctivae) Moraxella ovis Colesiota conjunctivae Listeria monocytogenes Acholeplasma oculi Thelazia spp | Primary etiological agent: Moraxella bovis Possible contributing agents:
|
aPublished experimental challenges of cattle with Moraxella bovoculi have not provided a direct link between Moraxella bovoculi infection and IBK. | |
Diagnostic testing of samples collected from affected eyes may help identify specific organisms associated with IKC. Treatment is to administer antimicrobials and provide supportive care, depending on the severity of disease and on other management and economic considerations.
For IBK, commercial and autogenous parenteral vaccines exist that currently use the bacteria Moraxella bovis or Moraxella bovoculi as vaccine antigens.
Clinical Findings of Infectious Keratoconjunctivitis in Ruminants
The earliest clinical signs of IKC are photophobia, blepharospasm, and epiphora; later, ocular discharge may become mucopurulent.
In small ruminants with IKC, conjunctivitis develops as the disease progresses; corneal ulceration may or may not be present.
In cattle with IBK, corneal ulceration typically starts near the center of the cornea. Initially, the area of cornea around an ulcer is clear; within a few hours, though, a faint haze appears that subsequently increases in opacity. One or both eyes can be affected.
In sheep and goats with IKC, concurrent polyarthritis can be associated with C pecorum infections. Appetite is often decreased because of ocular discomfort or visual disturbance. The usual clinical course varies from a few days to several weeks. Relapse may occur at any stage of recovery.
In cattle with IBK (see ), corneal lesions may regress in the early stages or continue to develop. After 48–72 hours in severe cases, the entire cornea may become opaque as a result of corneal edema (hazy white to blue corneas), thus blinding the animal in the affected eye. In more severe cases, leukocyte infiltration due to the inflammatory process can occur (milky white to yellow corneas; see ).


Steer with infectious bovine keratoconjunctivitis. Note the extensive tearing (epiphora) that extends below the left eye down the side of the face. The partial closure of the left eyelid indicates ocular pain as well.
Courtesy of Dr. John A. Angelos.

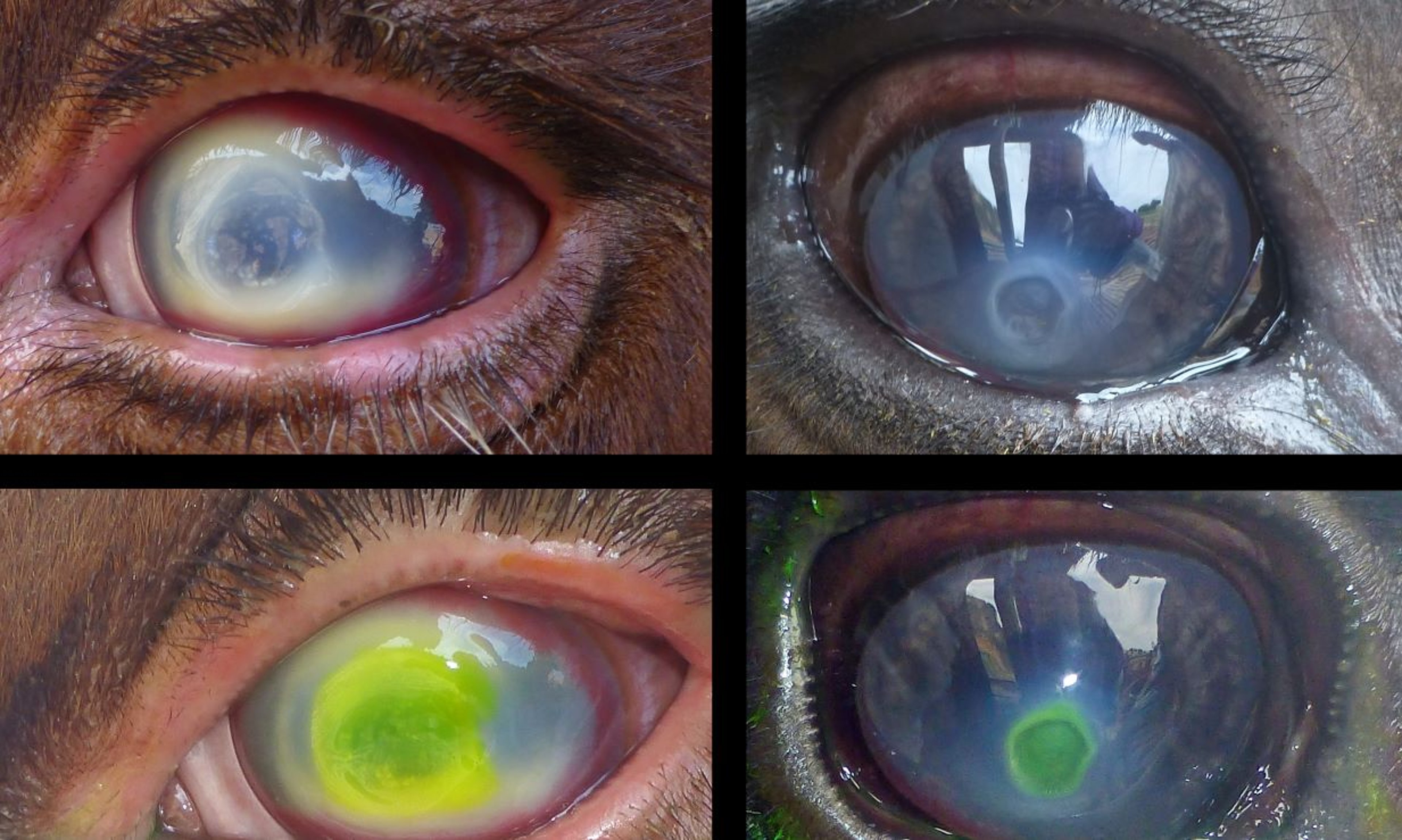
The eyes of two different steers with infectious bovine keratoconjunctivitis before (top) and after (bottom) staining with fluorescein to demonstrate areas of corneal ulceration (shown by yellow or green staining). Conjunctivitis, corneal neovascularization, and corneal edema (opacity) are present in both animals; however, the case on the left is more advanced, as demonstrated by the greater area of affected cornea and corneal neovascularization, as well as corneal stromal infiltration by white blood cells (whitish or yellow areas surrounding the ulcer).
Courtesy of Dr. John A. Angelos.
In cattle with severe IBK and small ruminants with more advanced IKC, deep corneal blood vessels begin to grow at a rate of ~1 mm/day into the cornea from the limbus. Deep corneal ulcers are at risk of perforation and globe rupture (see ). Complete globe rupture results in permanent blindness.

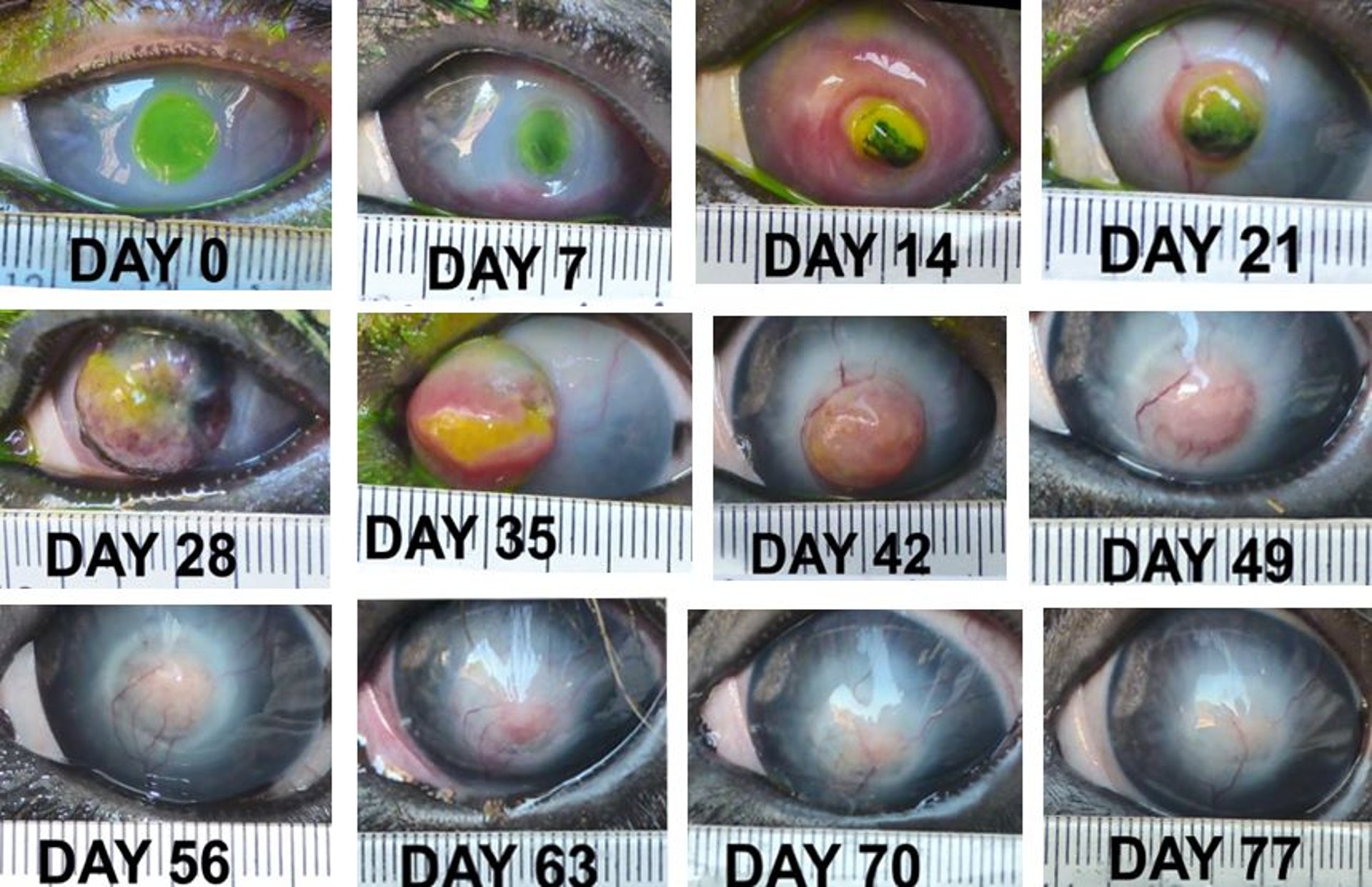
In this steer, an ulcer associated with infectious bovine keratoconjunctivitis was first noted on day 0, and the animal was treated with systemic antimicrobials. On day 7, the ulcer had a dark center suggestive of impending perforation. On day 14 the iris had prolapsed as a result of corneal perforation, and on day 28 the globe had ruptured. From day 35 to day 77, the corneal injury healed, with scar formation and superficial corneal neovascularization.
Courtesy of Dr. John A. Angelos.
In some instances of corneal perforation, the iris can become attached to the site of perforation, thus preventing complete globe rupture (see ). Subsequent healing results in the formation of anterior synechiae.


An ulcer associated with infectious bovine keratoconjunctivitis was first detected in this steer on day 0 (both unstained and fluorescein-stained day 0 images are shown). On day 7, the iris was visible at the site of corneal rupture; systemic antimicrobials and flunixin meglumine were administered. Subsequent stages of healing from days 14 through 28 are shown.
Courtesy of Dr. John A. Angelos.
Healed animals typically display varying amounts of corneal scarring that may or may not resolve with time. If severe enough, such scarring may impair vision.
Diagnosis of Infectious Keratoconjunctivitis in Ruminants
Clinical signs
Microbial culture
Molecular testing
Cytological evaluation
A presumptive diagnosis of IBK or IKC is usually based on clinical ocular signs in conjunction with general physical examination findings.
In patients with corneal ulceration, it is important to rule out the possibility that a foreign body such as a plant awn or parasite is present in the affected eye.
In infectious bovine rhinotracheitis, upper respiratory signs and conjunctivitis predominate, and keratitis accompanied by ulceration is rare.
In bovine malignant catarrhal fever, respiratory signs are prominent with primary uveitis and associated keratitis.
Bacterial agents such as Moraxella spp can be identified from ocular swabs of affected eyes via traditional culturing of samples on standard bacterial growth media, followed by biochemical testing. Molecular testing methods are also available for the detection and speciation of Moraxella spp and Mycoplasma spp.
Many diagnostic laboratories have adopted the use of newer technology, such as matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS), to identify bacteria.
Diagnostic testing on collected samples for Chlamydophila and Mycoplasma typically requires special media, and a diagnostic laboratory should be consulted before sample collection and transport when trying to identify these agents. In cases of suspected IKC in small ruminants, conjunctival scrapes or exfoliative cytology can also provide cytological information that may help identify chlamydial organisms.
Treatment and Prevention of Infectious Keratoconjunctivitis in Ruminants
Treatment
Conventional treatment of IKC and IBK is to administer antimicrobials. Although Moraxella spp are relatively susceptible to a variety of antimicrobials, relatively few have a label claim for the treatment of IBK. However, anecdotal reports suggest the following treatment recommendations:
In the US, parenterally administered oxytetracycline and tulathromycin have been approved for the treatment of IBK associated with Moraxella bovis in cattle.
Topical oxytetracycline (formulated as oxytetracycline hydrochloride and polymyxin B sulfate in an ophthalmic ointment) is approved for pinkeye treatment in cattle and sheep.
Dilute hypochlorous acid spray is also available in the US for treating pinkeye in cattle and goats.
Topical ointments or sprays should be applied at least every 8–12 hours to be effective; thus they may not be practical in typical herd settings.
Other antimicrobials that have been experimentally shown as effective in treating IBK in cattle, but that are not currently FDA approved for this indication, include ceftiofur crystalline free acid and florfenicol. Federal regulations in the US prohibit extra-label use of certain drugs in food-producing animals. Extra-label use of cephalosporins (excluding cephapirin) is prohibited in cattle, swine, chickens, or turkeys for disease prevention; at unapproved routes of administration, doses, frequencies, or durations; or if the drug is not approved for that species and production class.
Given the lack of drugs specifically labeled for IKC treatment, extra-label use of drugs such as oxytetracycline and tulathromycin that are approved for the treatment of IBK in cattle is a rational antimicrobial treatment choice for IKC in small ruminants.
Injection of penicillin under the bulbar conjunctiva, though not specifically approved for treating IBK, is a common practice among cattle producers and veterinarians. Specific milk withdrawals following such use in dairy cattle must be observed to avoid illegal drug residues in milk.
Nitrofurazone-containing puffers are still available in farm supply stores for treating a variety of conditions, including eye infections in small animals. They may seem an attractive option for the treatment of IKC or IBK; however, the use of any nitrofurazone-containing product in food-producing animals is illegal in the US.
A temporary eye patch glued to the hair surrounding the eye is an inexpensive and easily applied treatment used in cattle with IBK. The eye patch provides shade, prevents exposure to flies, and may help to decrease the transmission of bacteria from infected eyes. In addition, in one study, corneal ulcers associated with IBK healed faster in cattle that received an eye patch along with systemic oxytetracycline and flunixin meglumine (1).
Animals with substantial uveitis secondary to keratoconjunctivitis may benefit from the application of 1% atropine ointment to the eye every 8–24 hours. This treatment prevents painful ciliary body spasm. Because atropine causes mydriasis, treated animals should be provided with shade. Systemic NSAID treatment (eg, with flunixin meglumine) may also provide relief.
Other possible treatments for keratoconjunctivitis, especially in animals with deep corneal ulcers, include the application of conjunctival or third-eyelid flaps, and tarsorrhaphy. These treatments can decrease morbidity in severely affected animals by providing corneal protection from light, flies, and physical irritants. In hospital settings where frequent drug treatments are more feasible than they are in the field, the administration of autologous serum eye drops can support the healing of an injured cornea.
Prevention
The main focus of IBK prevention in cattle is to mitigate common risk factors known to be associated with IBK, as well as to vaccinate. Examples of risk factor control practices include the following:
controlling external parasites to minimize face fly (Musca autumnalis, an important vector for Moraxella bovis) burdens via topical or parenteral treatments, dust bags, and/or application of insecticide-impregnated ear tags to calves
mowing pastures that have mature or dry seed awns before turning animals out onto the pasture
maintaining trace mineral supplementation programs (for copper and selenium supplementation in cattle raised in copper- and selenium-deficient areas)
For prevention of both IBK and IKC, it is recommended that affected animals be isolated from herdmates whenever possible and feasible. In addition, use of gloves and protective clothing that can be disinfected between animals, as well as disinfection of any handling equipment, is recommended to prevent the iatrogenic transmission of microorganisms potentially associated with these diseases.
The following solutions are commonly used for disinfecting equipment:
~0.05% chlorhexidine, made by mixing ~100 mL of a 2% stock solution per gallon of water.
10% household bleach, prepared by mixing ~1–1.5 cups of regular-strength household bleach per gallon of water. If the bleach is concentrated, ~0.5 cups of bleach should be used per gallon of water to achieve an ~10% solution.
Given that bleach is inactivated by organic debris, disinfecting solutions should be prepared more frequently when they become soiled.
In the US, no vaccines are commercially available for controlling IKC in small ruminants. Therefore, control of the disease relies primarily on 1) minimizing exposure by identifying, treating, and isolating sick animals; and 2) preventing transmission within a herd by temporarily isolating new herd additions and animals returning from shows or livestock exhibits.
For IBK prevention, Moraxella bovis and Moraxella bovoculi commercial and autogenous bacterins are available; however, the efficacy of these vaccines against IBK is a matter of considerable debate.
In most published randomized, controlled field trials evaluating commercial or autogenous Moraxella bovis or Moraxella bovoculi bacterins that were parenterally administered, these vaccines were not found to be effective against IBK (2, 3, 4, 5).
This lack of efficacy could arise from antigenic variation between outbreak and vaccinal strains of Moraxella. This possibility seems plausible, especially because of a report that two different genotypes of Moraxella bovis exist in North America (6). Two different genotypes of Moraxella bovoculi have also been characterized; however, only one of these has been associated with clinical cases of IBK (7, 8).
In a study that evaluated three vaccines (an autogenous vaccine containing antigens from Moraxella bovis, Moraxella bovoculi, and Mycoplasma bovoculi; a commercially available Moraxella bovis vaccine; and a sham vaccine [adjuvant]), a numerically lower cumulative incidence of IBK was reported among animals that received the autogenous vaccine (9).
Although this difference was not statistically significant, it may be biologically important, given that the animals in the autogenous vaccine group also had fewer cases of IBK that required retreatment.
In contrast to the results observed in formal studies, anecdotal reports of successes for both commercial and autogenous vaccines against Moraxella spp suggest that in some herds, IBK prevention through vaccination can be effective.
To allow time for adequate immune responses to develop after vaccination against IBK, vaccines should be administered ≥ 4 weeks before expected seasonal increases in IBK. The use of modified live virus vaccines against infectious bovine rhinotracheitis (IBR) has been associated with IBK in cattle; therefore, the timing of IBR vaccination with regard to animal shipment, especially at higher-risk times of the year (summer and warmer months), may be important (10).
Given that IBK occurs on a mucosal surface, intranasal vaccination to boost local ocular immunity to Moraxella spp antigens may provide an alternative to currently available parenterally administered vaccines. An experimental intranasal vaccine that used a Moraxella bovis cytotoxin subunit administered to cattle in two doses 21 days apart resulted in increased cytotoxin-specific tear IgA, as well as less severe corneal ulcers in vaccinates compared to controls (11).
It is likely that vaccines against Moraxella spp will never be completely effective at controlling IBK in the face of important risk factors such as flies, dust, other infectious agents, and trace mineral deficiencies. IBK control programs should aim to mitigate such risks as much as possible to help maximize the chances for success at preventing this disease in cattle.
Key Points
Early identification and treatment of infectious keratoconjunctivitis (IKC; pinkeye) in cattle, sheep, and goats is important to minimize animal pain and suffering and to decrease transmission within a herd.
Addressing risk factors is an important aspect of disease control.
For infectious bovine keratoconjunctivitis (IBK) in cattle, vaccination is controversial; however, anecdotal reports suggest that there can be benefits from vaccination in some herds.
For More Information
O'Connor AM, Angelos JA, Dennis EJ, et al. Future directions for research in infectious bovine keratoconjunctivitis. Vet Clin North Am Food Anim Pract. 2021;37:371-379. doi:10.1016/j.cvfa.2021.03.011
Maier G, O'Connor AM, Sheedy D. The evidence base for prevention of infectious bovine keratoconjunctivitis through vaccination. Vet Clin North Am Food Anim Pract. 2021;37(2):341-353. doi:10.1016/j.cvfa.2021.03.009
Loy JD, Hille M, Maier G, Clawson ML. Component causes of infectious bovine keratoconjunctivitis - the role of Moraxella species in the epidemiology of infectious bovine keratoconjunctivitis. Vet Clin North Am Food Anim Pract. 2021;37(2):279-293. doi:10.1016/j.cvfa.2021.03.004
Loy JD, Clothier KA, Maier G. Component causes of infectious bovine keratoconjunctivitis—non-Moraxella organisms in the epidemiology of infectious bovine keratoconjunctivitis. Vet Clin North Am Food Anim Pract. 2021;37(2):295-308. doi:10.1016/j.cvfa.2021.03.005
Kneipp M. Defining and diagnosing infectious bovine keratoconjunctivitis. Vet Clin North Am Food Anim Pract. 2021;37(2):237-252. doi:10.1016/j.cvfa.2021.03.001
References
Maier GU, Davy JS, Forero LC, Bang H, Clothier K, Angelos JA. Effects of eye patches on corneal ulcer healing and weight gain in stocker steers on pasture: a randomized controlled trial. Transl Anim Sci. 2021;5:1-9. doi/10.1093/tas/txab162
O'Connor A, Cooper V, Censi L, Meyer E, Kneipp M, Dewell G. A 2-year randomized blinded controlled trial of a conditionally licensed Moraxella bovoculi vaccine to aid in prevention of infectious bovine keratoconjunctivitis in Angus beef calves. J Vet Intern Med. 2019;33(6):2786-2793. doi:10.1111/jvim.15633
Cullen JN, Engelken TJ, Cooper V, O'Connor AM. Randomized blinded controlled trial to assess the association between a commercial vaccine against Moraxella bovis and the cumulative incidence of infectious bovine keratoconjunctivitis in beef calves. J Am Vet Med Assoc. 2017;251:345-351. doi:10.2460/javma.251.3.345
O'Connor AM, Brace S, Gould S, Dewell R, Engelken T. A randomized clinical trial evaluating a farm-of-origin autogenous Moraxella bovis vaccine to control infectious bovine keratoconjunctivis (pinkeye) in beef cattle. J Vet Intern Med. 2011;25(6):1447-1453. doi:10.1111/j.1939-1676.2011.00803.x
Funk L, O'Connor AM, Maroney M, et al. A randomized and blinded field trial to assess the efficacy of an autogenous vaccine to prevent naturally occurring infectious bovine keratoconjunctivitis (IBK) in beef calves. Vaccine. 2009;27(34):4585-4590. doi:10.1016/j.vaccine.2009.05.082
Wynn EL, Hille MM, Loy JD, et al. Whole genome sequencing of Moraxella bovis strains from North America reveals two genotypes with different genetic determinants. BMC Microbiol. 2022;22:art. 258. doi:10.1186/s12866-022-02670-3
Dickey AM, Schuller G, Loy JD, Clawson ML. Whole genome sequencing of Moraxella bovoculi reveals high genetic diversity and evidence for interspecies recombination at multiple loci. PLoS One. 2018;13(12):e0209113. doi:10.1371/journal.pone.020911
Dickey AM, Loy JD, Bono JL, et al. Large genomic differences between Moraxella bovoculi isolates acquired from the eyes of cattle with infectious bovine keratoconjunctivitis versus the deep nasopharynx of asymptomatic cattle. Vet Res. 2016;47:art. 31. doi:10.1186/s13567-016-0316-2
Hille MM, Spangler ML, Clawson ML, et al. A five year randomized controlled trial to assess the efficacy and antibody responses to a commercial and autogenous vaccine for the prevention of infectious bovine keratoconjunctivitis. Vaccines (Basel). 2022;10(6):916. doi:10.3390/vaccines10060916
George LW, Ardans A, Mihalyi J, Guerra MR. Enhancement of infectious bovine keratoconjunctivitis by modified-live infectious bovine rhinotracheitis virus vaccine. Am J Vet Res. 1988;49(11):1800-1806.
Angelos JA, Agulto RL, Mandzyuk B, Chigerwe M. Randomized controlled field trial to assess the efficacy of an intranasal Moraxella bovis cytotoxin vaccine against naturally occurring infectious bovine keratoconjunctivitis. Vaccine X. 2023;15:100378. doi:10.1016/j.jvacx.2023.100378


