




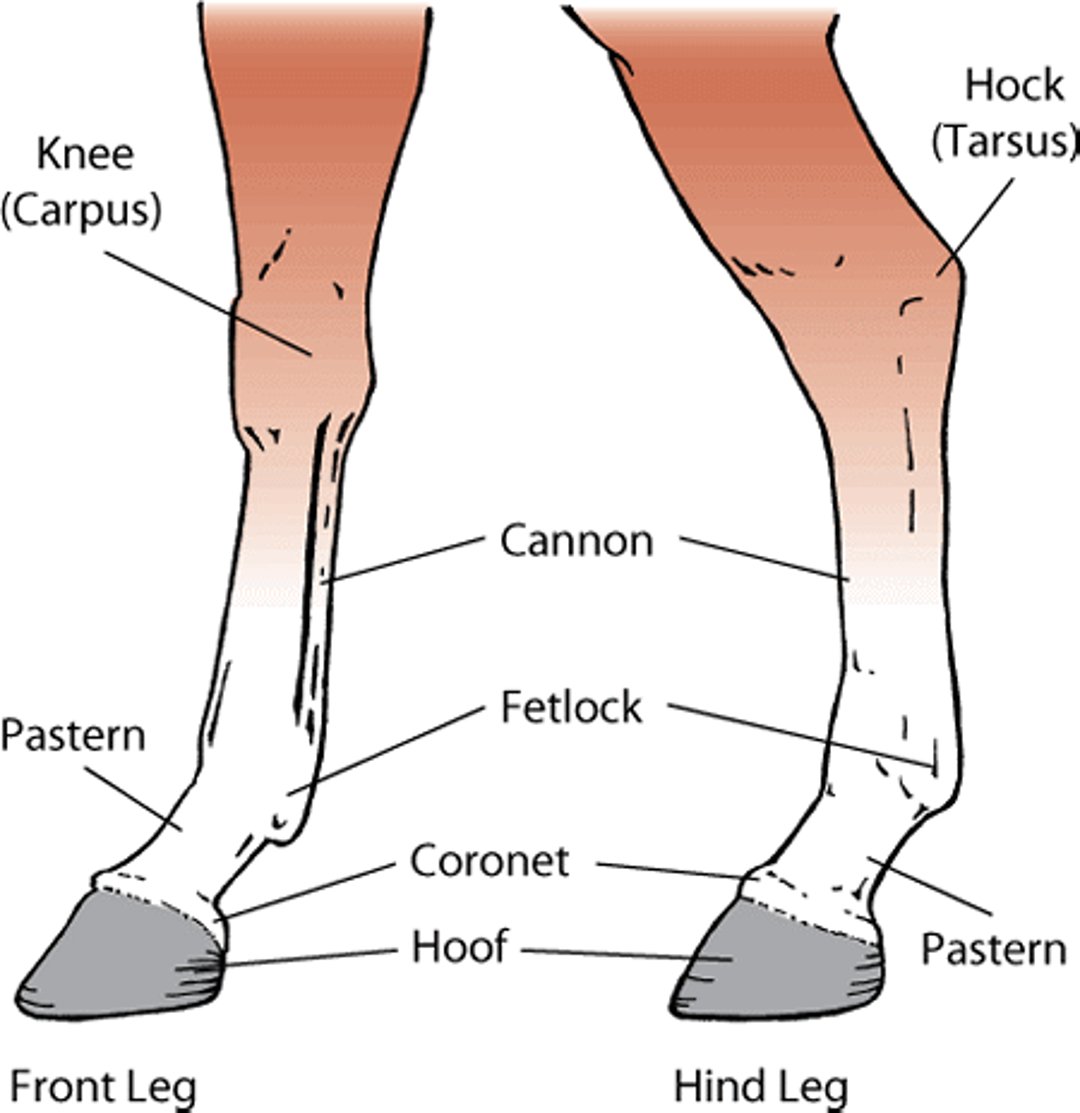
Fetlock is a term used for the joint where the cannon bone, the proximal sesamoid bones, and the first phalanx (long pastern bone) meet. The pastern is the area between the hoof and the fetlock joint. Disorders of the fetlock and pastern include conditions such as fractures, osteoarthritis, osselets, ringbone, sesamoiditis, synovitis, and windgalls.
Legs, horse

Fractures of Phalanges and Proximal Sesamoids
Fractures of the long pastern bone (first phalanx) are not uncommon in racehorses or other performance horses. They may be small “chip” fractures, fractures along the length of the bone (split pastern), or comminuted fractures in which the bone is broken into multiple fragments.
Chip fractures often occur on the top, upper portion of the long pastern bone. They usually occur when the horse is exercising at a high speed due to overextension (hyperextension) of the fetlock joint. An affected horse will suddenly become lame and have swelling of the fetlock joint.
Another type of fracture involves chips or loose fragments on the back of the long pastern bone. They may be due to trauma or osteochondrosis. These fractures are more common in the hindlimb and may involve the joint.
Signs of longitudinal or comminuted fractures involve sudden, severe weightbearing lameness after work or a race. There may be significant swelling and intense pain on feeling or bending the fetlock joint.
Diagnosis involves physical and lameness examinations and, sometimes, nerve blocks. X-rays confirm the diagnosis, although it can be difficult to see the fine line of the fracture. In some circumstances, computed tomography (CT scan) may aid in diagnosis and repair of the fracture.
Chip and fragmented fractures can be surgically removed using an endoscope. The outlook is excellent for these fractures as long as no other abnormalities are present. Long, split fractures can be repaired using 2 or more bone screws. Conservative treatment of severely fragmented fractures involves using a cast for up to 12 weeks. Complications of long pastern bone fractures include poor alignment at the fracture site, failure of implants (such as screws), laminitis in the opposite limb, and secondary arthritis.
Fractures of the short pastern bone (second phalanx) are most common in Quarter horses and typically affect the hindlimbs. The chip fractures that occur in the long pastern bone are uncommon in the short pastern bone. Fractures of the upper portion of the bone (called palmar or plantar eminence fractures) or multiple fragments of the bone (comminuted fractures) are more likely. Most fractures of the short pastern bone require surgical repair. Some residual lameness usually remains after healing and depends on the degree of arthritis present in surrounding joints. The outlook depends on how comfortable the horse is after fracture repair. If uncomfortable, the horse has an increased risk of laminitis in the opposite limb.
Fractures of the proximal sesamoid bones are relatively common and often extend into the fetlock. The most common sesamoid fractures of Thoroughbreds and Standardbreds are caused by overextension and often are associated with damage to the suspensory ligament. Shoeing with a trailer-type shoe may cause fractures of the proximal sesamoid bones in the hindlimb of Standardbreds. Signs of fracture include heat, pain, and sudden onset of lameness; these tend to worsen when the fetlock joint is bent. There is bleeding and fluid buildup in the fetlock joint. X‑rays confirm the diagnosis.
The outlook for recovery is fairly good if small fragments are surgically removed as soon as possible. Many of these horses can return to racing. Horses with a fracture in a hindlimb respond more favorably than those with a fracture in the forelimb. The outlook for recovery in large fractures at the base of the fetlock bone is poor, regardless of the treatment. Very severe damage to the suspensory ligaments, including fracture of both sesamoid bones, is a catastrophic injury and can cause a compromise of blood flow to the foot. Some horses can still be used for breeding by surgical fusion of the fetlock joint.
Ringbone
Ringbone is inflammation of the connective tissue surrounding the pastern bone or osteoarthritis in the digits. It leads to the development of spurs or outgrowths of bone. Causes include poor conformation, improper shoeing, or repeated jarring injury from working on hard ground. Trauma and infection, especially wire-cut wounds, are other causes. In light horses, the condition may result from strains on ligaments and tendons in the pastern region.
The pastern may become bell-shaped when affected by ringbone. Inflammation of the connective tissue will initially cause lameness. The lameness may subside once the bony outgrowths appear, particularly if the surfaces of the joint are unaffected. If joint surfaces are involved, lameness tends to persist, sometimes leading to the fusion of the bones to the joint. Your veterinarian will diagnose the condition by physical examination of your horse, use of regional analgesia to identify the location of pain, and x-rays to confirm the findings.
Complete rest is the most important requirement for treatment. Cold and astringent applications as well as radiation therapy in the early stages may be beneficial. Anti-inflammatory medication may relieve the signs of lameness. Surgically fusing the pastern joint can improve the lameness in many cases.
Sesamoiditis
The sesamoid bones in the fetlock are kept in position by ligaments. Due to the great stress placed on the fetlock during racing, the sesamoid bones are susceptible to injuries. Inflammation of the sesamoid bones, or sesamoiditis, can result in bony changes (including the excessive production or loss of bone). Horses with sesamoiditis may have a significantly greater risk of developing a suspensory ligament injury after starting training.
The signs of sesamoiditis are similar to—but less severe than—those resulting from sesamoid fracture (see above). The amount of lameness or swelling will depend on the extent of the damage. Reduced speed may be the only sign of lameness. A veterinarian will look for pain and heat while bending the fetlock joint, but x-rays are necessary for accurate diagnosis and evaluation.
The recommended treatment is enforced rest and symptomatic treatment to combat inflammation and soreness.
Villonodular Synovitis (Chronic Proliferative Synovitis)
Villonodular synovitis is inflammation of a fibrous cartilage pad found in the upper, front portion of the membrane (joint capsule) surrounding the forelimb fetlock joint. It is thought to be caused by repetitive trauma from exercise. Typically, this condition is found most frequently in racing Thoroughbreds, but it may also develop in Standardbreds and nonracing breeds. Signs include a firm swelling on the upper, front aspect of the fetlock joint, swelling and decreased movement of the fetlock joint, and lameness. Changes to the surrounding bone and cartilage may occur.
To diagnose villonodular synovitis, your veterinarian will examine your horse for the presence of a nodule or small lump around the joint. X-rays confirm the diagnosis. Arthroscopic surgery is performed to remove the nodule.
Digital Sheath Tenosynovitis (Windgalls, Windpuffs)
The digital sheath surrounds the digital flexor tendons, extending from the lower third of the cannon bone to the navicular bursa within the hoof. Inflammation of the digital sheath (tenosynovitis) is common in all types of working horses. Puffy, fluid-filled swellings along the backside of the hind limbs (called "windpuffs") does not usually cause a problem. They generally are not accompanied by heat, pain, or lameness. However, swelling of the tendon sheath in only one leg typically indicates a problem and can lead to lameness. Trauma and hard exercise are believed to contribute to the condition. The condition can occur due to a problem involving the tendon sheath or one of the structures within it.
The diagnosis is made with a physical examination and ultrasonography. In the absence of lameness, treatment is not warranted. Treatment of the sheath with corticosteroids or hyaluronic acid may be sufficient. In other cases, surgery with an endoscope may be necessary.







