

Anthrax is a noncontagious zoonotic disease caused by the spore-forming bacterium Bacillus anthracis. Anthrax primarily affects domestic and wild herbivores. Clinical features, characterized by sudden death, with leakage of uncoagulated blood from natural openings, overlap those of the hemorrhagic fevers, with hyperacute or acute onset of clinical signs. Common diagnostic tests include microscopic examination, culture, and PCR assay. The most effective control strategy for animals in endemic areas is vaccination. Antimicrobial therapy is effective if administered at an early stage. Control measures include proper disposal of carcasses, disinfection and decontamination of contaminated materials, and environmental decontamination.
Anthrax is a noncontagious zoonotic disease caused by the spore-forming bacterium Bacillus anthracis. Anthrax is most common in wild and domestic herbivores (eg, cattle, sheep, goats, camels, and antelopes) but can also be seen in humans exposed to tissue from infected animals, to contaminated animal products, or under certain conditions, directly to B anthracis spores. Depending on the route of infection, host factors, and potentially strain-specific factors, anthrax can have different clinical manifestations. In herbivores, anthrax commonly causes acute septicemia with a high fatality rate, often accompanied by hemorrhagic lymphadenitis. In dogs, humans, horses, and pigs, disease is usually less acute but still potentially fatal.
Spores of B anthracis can remain viable in soil for many years. During this time, they are a potential source of infection for grazing animals; however, they generally do not represent a direct risk of infection for people. Grazing animals may become infected when they ingest sufficient quantities of spores from the soil. In addition to direct transmission, biting flies may mechanically transmit B anthracis spores from one animal to another. The latter follows when there have been rains encouraging a high fly hatch and there are 4–6 moribund or dead cattle for the flies to feed on (eg, if reporting has been delayed on the index ranch during an epizootic). Feed contaminated with bone or other meal from infected animals can serve as a source of infection for production animals, as can hay muddy with contaminated soil. Raw or poorly cooked contaminated meat is a source of infection; anthrax resulting from contaminated meat consumption has been reported in pigs, dogs, cats, mink, wild carnivores, and humans.
Etiology and Pathogenesis of Anthrax in Animals
Bacillus anthracis, the causative agent of anthrax, is a large, gram-positive, aerobic, spore-forming bacillus.
After wound inoculation, ingestion, or inhalation, anthrax spores infect macrophages, germinate, and proliferate. In cutaneous and GI infection, proliferation can occur at the site of infection and in the lymph nodes draining the site of infection. Lethal toxin and edema toxin are produced by B anthracis and respectively cause local necrosis and extensive edema, which are frequent characteristics of the disease. As the bacteria multiply in the lymph nodes, toxemia progresses and bacteremia may ensue. With the increase in toxin production, the potential for disseminated tissue destruction and organ failure increases.
After vegetative bacilli are discharged from an animal after death (by carcass bloating, scavengers, or postmortem examination), the oxygen content of air induces sporulation. Spores are relatively resistant to extremes of temperature, chemical disinfection, and dessication. Necropsy is discouraged because of the potential for blood spillage and vegetative cells to be exposed to air, resulting in large numbers of spores being produced. Because of the rapid pH change after death and decomposition, vegetative cells in an unopened carcass quickly die without sporulating.
Epidemiology of Anthrax in Animals
Anthrax has been reported on nearly every continent and is most common in agricultural regions with neutral or alkaline, calcareous soils. In these regions, anthrax epizootics periodically emerge among susceptible domesticated and wild animals. These epizootics are usually associated with drought, flooding, or soil disturbance, and many years may pass between outbreaks. During interepidemic periods, sporadic cases may keep soil contaminated. Anthrax is now absent from some countries in western Europe, north Africa, and east of the Mississippi river in the US.
Underdiagnosis and unreliable reporting make it difficult to estimate the true incidence of anthrax worldwide. The precise incidence of anthrax among animals in the US is unknown. Animal infections have been seen in nearly all states, with highest frequency in the Midwest and West. Anthrax is enzootic in west Texas and northwest Minnesota; sporadic in south Texas, Montana, eastern North and South Dakota; and only occasionally seen elsewhere. Since 1900, the annual incidence of human anthrax in the US has declined from ~130 cases annually to no reported cases in 2004–2005.
Human cases may occur after contact with contaminated carcasses or animal products. In areas where home slaughter and sanitation issues exist, each affected cow is estimated to result in up to 10 human cases. The risk of human disease in these settings is comparatively small in more developed economies, partly because people are relatively resistant to infection.
Four clinical forms of anthrax are seen in humans:
In cases of natural transmission (>95% of all cases), people exhibit primarily cutaneous anthrax.
Gastrointestinal anthrax (including pharyngeal anthrax) may be seen among human populations after consumption of contaminated raw or undercooked meat.
Under certain artificial conditions (eg, laboratories, animal hair processing facilities, and exposure to weaponized spore products), humans may develop a highly fatal form of disease known as inhalational anthrax or wool sorter’s disease. This form manifests as acute hemorrhagic lymphadenitis of the mediastinal lymph nodes, often accompanied by hemorrhagic pleural effusions, severe septicemia, and meningitis. Inhalational anthrax is associated with a high mortality rate.
An uncommon fourth form of the disease, injection anthrax results from the subcutaneous inoculation of B anthracis spores. Cases have mostly been associated with contaminated heroin.
The CDC High-Priority Biological Agents and Toxins list includes B anthracis in Category A (highest priority), and it has been manufactured as a biological warfare agent. In 2001, B anthracis was used successfully as a weapon of terrorism, killing 5 people and causing disease in 22. Probably because of the method of delivery (via mail), no known animal disease resulted from this attack. Weaponized spores represent a threat to both human and animal populations. The World Health Organization has estimated that 50 kg of B anthracis released upwind of a population center of 500,000 could result in 95,000 deaths and 125,000 hospitalizations. The effect on animal populations has not been estimated, but because production animals are more susceptible to B anthracis infection than primates, the outcome of an aerosol attack with B anthracis spores against production animals would result in higher and earlier mortality and morbidity rates than among a human population. Subsequent to the 1979 Severdlovsk anthrax leak, in which B anthracis spores were accidentally released from a Soviet military research facility, human cases were seen up to 4 km from the source, but dead sheep were noted 64 km downwind and in villages between.
The typical incubation period for anthrax is 3–7 days (range, 1−14 days).
Clinical Findings of Anthrax in Animals


Photograph of an anthrax-infected bovine carcass. Note the marked bloating. Bacteria in body fluids exuded from orifices after death form spores that contaminate nearby soil and vegetation.
Courtesy of Dr. Domenico Galante.
The clinical course ranges from peracute to chronic. The peracute form (common in cattle and sheep) is characterized by sudden onset and a rapidly fatal course. In cattle, sheep, and goats, staggering, dyspnea, trembling, collapse, a few convulsive movements, and death after only a brief period of illness may occur.
In acute anthrax of cattle and sheep, there is an abrupt onset of fever and a period of excitement followed by lethargy, stupor, respiratory or cardiac distress, staggering, seizures, and death. Often, the course of disease is so rapid that illness is not observed, and animals are found dead. Body temperature may reach 41.5°C (107°F), rumination ceases, milk production is materially reduced, and pregnant animals may abort. There may be bloody discharges from the natural body openings. Some infections are characterized by localized, subcutaneous edema, and swelling can be quite extensive. Areas most frequently involved are the ventral aspect of the neck, thorax, and shoulders.
Anthrax in horses may be acute. Clinical signs may include fever, chills, severe colic, anorexia, depression, weakness, bloody diarrhea, and swellings of the neck, sternum, lower abdomen, and external genitalia. Death usually occurs within 2–3 days following onset of signs of disease.
Although they are relatively resistant to anthrax, pigs may develop acute septicemia after ingestion of B anthracis, characterized by sudden death, oropharyngitis, or more usually a mild, chronic form. Oropharyngeal anthrax is characterized by rapidly progressive swelling of the throat, which may cause death by suffocation. In the chronic form, pigs have systemic clinical signs of illness and gradually recover with treatment. Some later have evidence of anthrax infection in the cervical lymph nodes and tonsils when slaughtered (as apparently healthy animals). Intestinal involvement is seldom recognized and has nonspecific clinical characteristics of anorexia, vomiting, diarrhea (sometimes bloody), or constipation.
In dogs, cats, and wild carnivores, anthrax resembles that seen in pigs. In wild herbivorous animals, the expected course of illness and lesions varies by species but resembles, for the most part, anthrax in cattle.
Postmortem Lesions
Rigor mortis is frequently absent or incomplete. Dark blood may ooze from the mouth, nostrils, and anus, with marked bloating and rapid body decomposition. If the carcass is inadvertently opened, septicemic lesions are evident. The blood is dark and thickened and fails to clot readily. Hemorrhages of various sizes are common on the serosal surfaces of the abdomen and thorax as well as on the epicardium and endocardium. Edematous, red-tinged effusions commonly are present under the serosa of various organs, between skeletal muscle groups, and in the subcutis. Hemorrhages frequently occur along the GI tract mucosa, and ulcers, particularly over Peyer’s patches, may be present. An enlarged, dark red or black, soft, semifluid spleen is common. The liver, kidneys, and lymph nodes usually are congested and enlarged. If the skull is opened, meningitis may be noted.
In pigs with chronic anthrax, lesions usually are restricted to the tonsils, cervical lymph nodes, and surrounding tissues. The lymphatic tissues of the area are enlarged and are a mottled salmon to brick-red color on cut surface. Diphtheritic membranes or ulcers may be present over the surface of the tonsils. The area around involved lymphatic tissues generally is gelatinous and edematous. A chronic intestinal form involving the mesenteric lymph nodes is also recognized.
Diagnosis of Anthrax in Animals
Clinical evaluation
Laboratory examinations
Diagnosis of anthrax based only on clinical signs is difficult. Confirmatory laboratory testing should be attempted if anthrax is suspected. Because the vegetative cell is not robust and will not survive 3 days in transit, the optimal sample is a cotton swab dipped in the blood and allowed to dry. This results in sporulation and the death of other bacteria and contaminants. For carcasses dead >3 days, either the nasal turbinates should be swabbed or turbinate samples removed. Pigs with localized disease are rarely bacteremic, so a small piece of affected lymphatic tissue that has been collected aseptically should be submitted. Before submission, the receiving reference laboratory should be contacted regarding appropriate specimen labelling, handling, and shipping procedures.

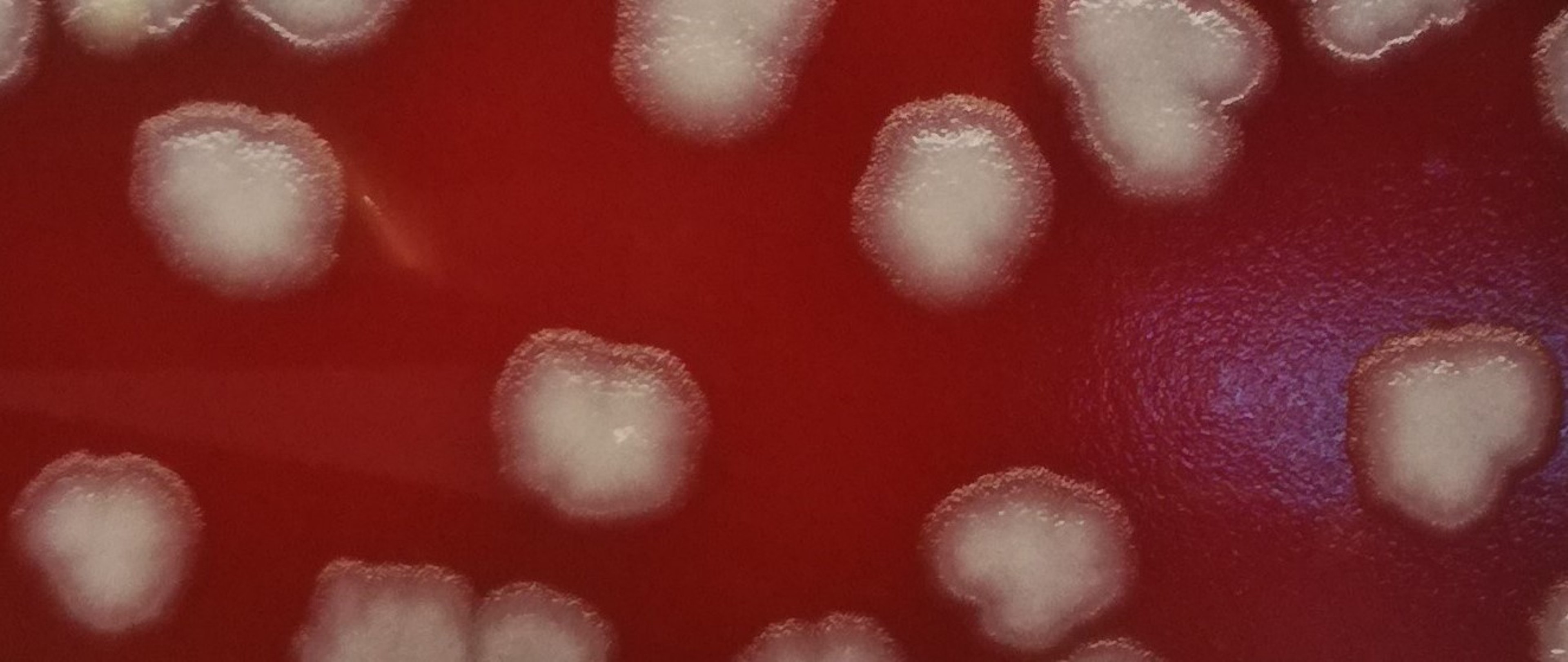
Subgross photograph of Bacillus anthracis colonies on blood agar. Colonies appear nonhemolytic and nonpigmented, with a dry, ground glass surface and irregular edges.
Courtesy of Dr. Domenico Galante.
Specific diagnostic tests include bacterial culture, PCR assay, and fluorescent antibody stains to demonstrate the agent in blood films or tissues. Western blot and ELISA for antibody detection are available at some reference laboratories. Lacking other tests, fixed blood smears stained with Loeffler’s or MacFadean stains can be used and the capsule visualized; however, this can result in a false-positive rate of ~20%.

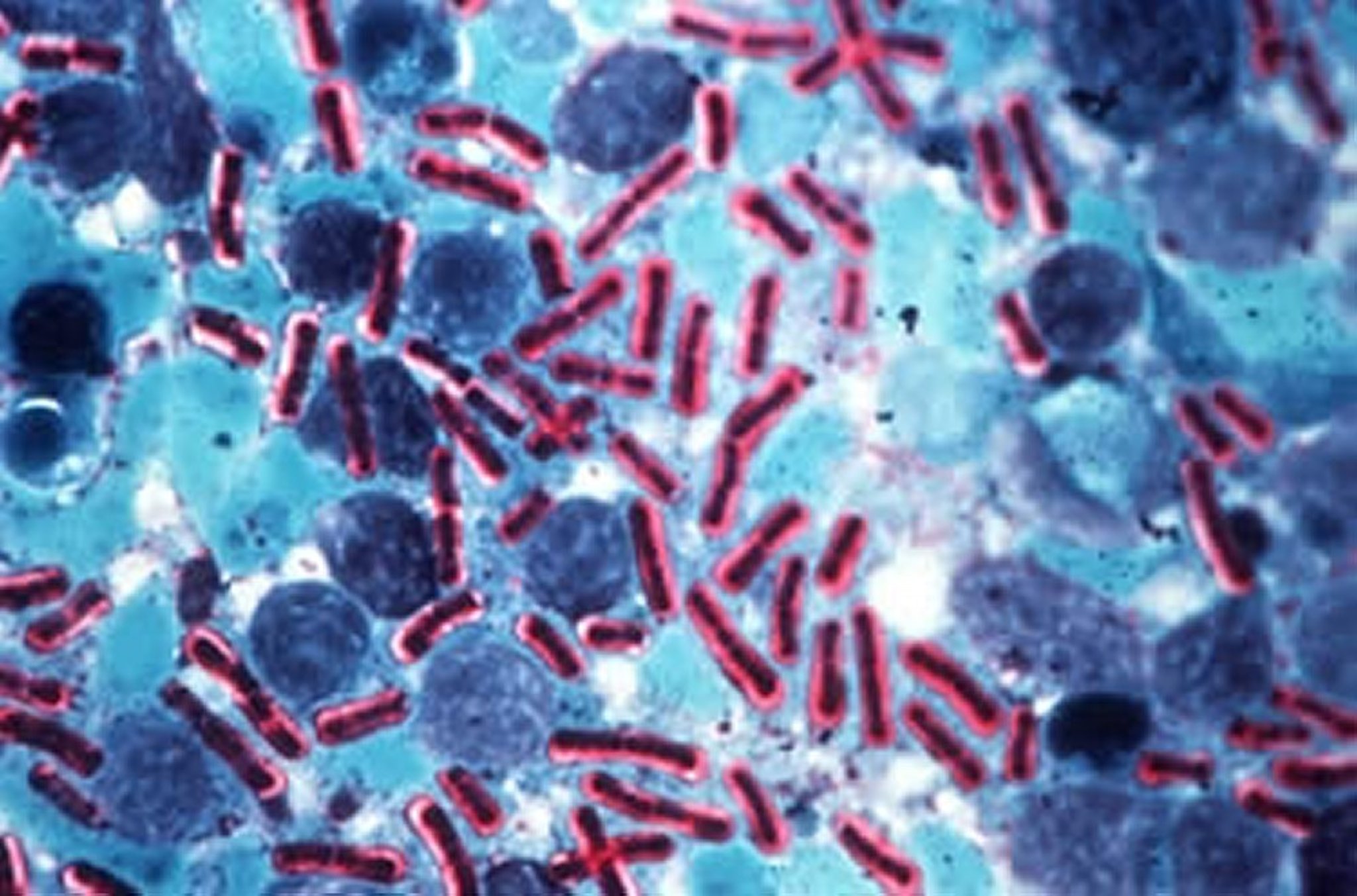
Photomicrograph of a tissue smear demonstrating Bacillus anthracis. Note the intense red stain of the large capsule of this organism. Methylene blue stain; original magnification, 400×.
Courtesy of the Department of Pathobiology, Ontario Veterinary College, University of Guelph.

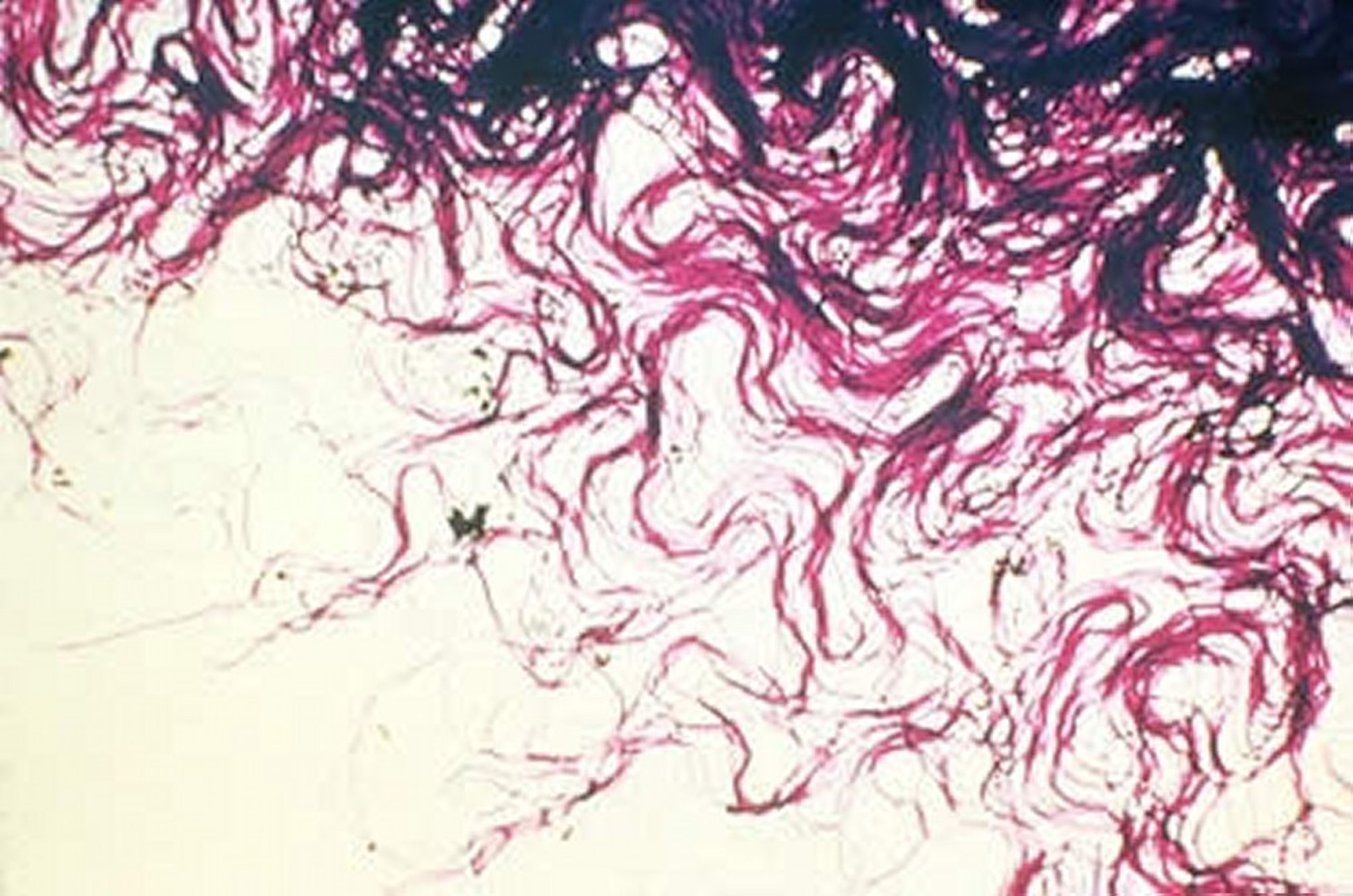
Bacillus anthracis colonies at small magnification, present at the edge of the colony and composed of long, interlacing chains of bacilli, resembling locks of matted hair and referred to as the "Medusa head appearance."
Courtesy of Dr. J. Glenn Songer.
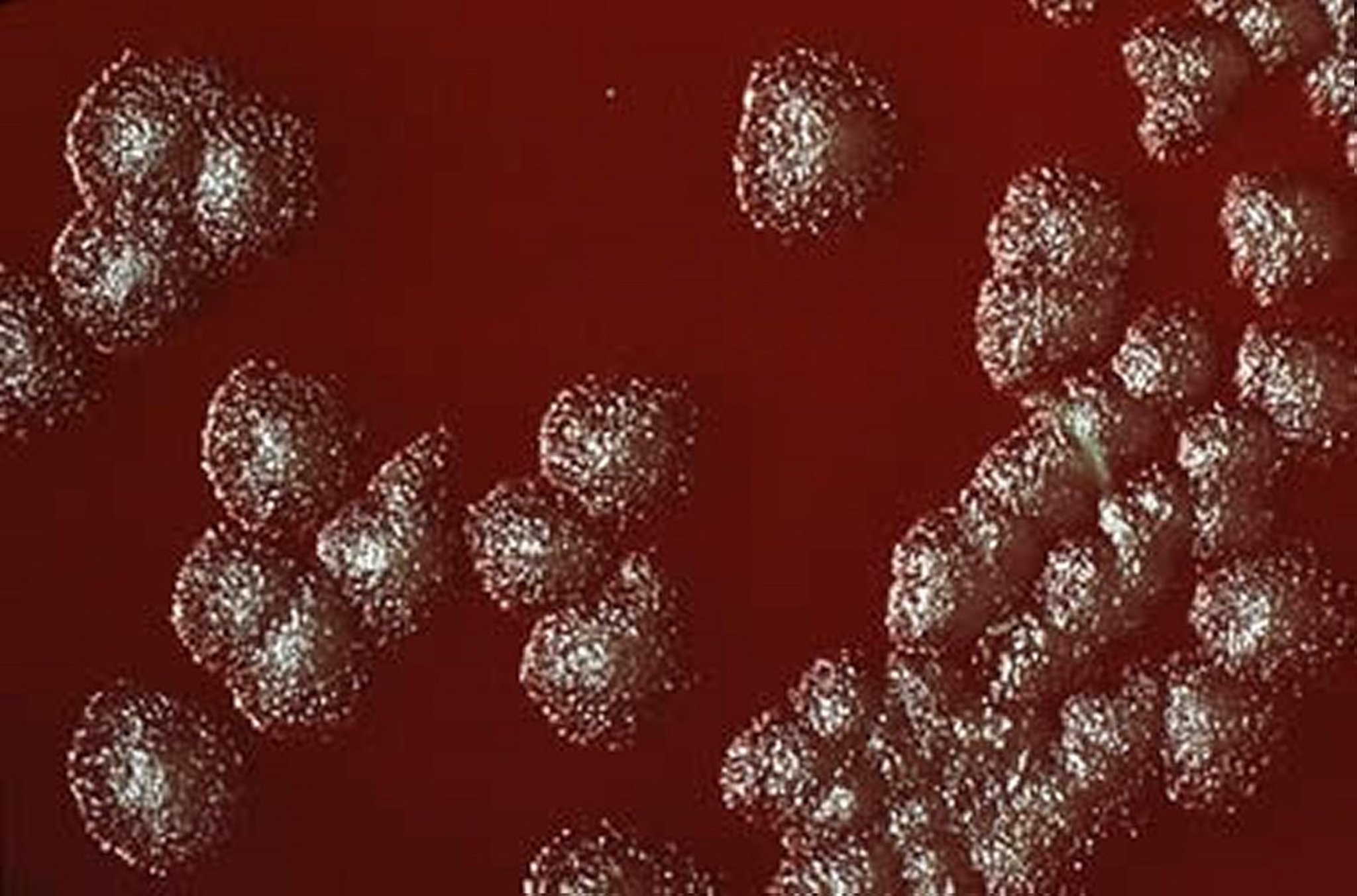
On agar plates, Bacillus anthracis forms opaque, grayish-white colonies 3–4 mm in diameter, with a rough surface and irregular, round margins called glass beads.
Courtesy of Dr. J. Glenn Songer.
In production animals, anthrax must be differentiated from other conditions that cause sudden death. In cattle and sheep, clostridial infections, bloat, and lightning strike (or any cause of sudden death) may be confused with anthrax. Also, acute leptospirosis, bacillary hemoglobinuria, anaplasmosis, and acute poisonings by bracken fern, sweet clover, and lead must be considered in cattle. In horses, acute infectious anemia, purpura, colic, lead poisoning, lightning strike, and sunstroke may resemble anthrax. In pigs, acute classical swine fever, African swine fever, and pharyngeal malignant edema are diagnostic considerations. In dogs, acute systemic infections and pharyngeal swellings due to other causes must be considered.
Treatment, Control, and Prevention of Anthrax in Animals
Vaccination
Management of anthrax-infected carcasses
Antimicrobial therapy
Anthrax is controlled through vaccination programs, rapid detection and reporting, quarantine, treatment of subclincally affected animals (postexposure prophylaxis), and burning or burial of suspect and confirmed cases. In production animals, anthrax can be controlled largely by annual vaccination of all grazing animals in the endemic area and by implementation of control measures during epizootics. The nonencapsulated Sterne-strain vaccine is used almost universally for production animal vaccination. Vaccination should be done at least 2–4 weeks before the season when outbreaks may be expected. Because this is a live attenuated spore vaccine, antimicrobials should not be administered within 1 week of vaccination. Before vaccination of dairy cattle during an outbreak, all of the procedures required by local laws should be reviewed and followed. Human anthrax vaccines currently licensed and used in the US and Europe are based on filtrates of artificially cultivated B anthracis.


An anthrax-infected bovine carcass. The head is covered by a plastic bag and the body by a plastic sheet to minimize bleeding on the soil and the dissemination of anthrax spores in the environment.
Courtesy of Dr. Domenico Galante.
Early treatment and vigorous implementation of a preventive program are essential to reduce losses among production animals. Animals at risk should be immediately treated with a long-acting antimicrobial to stop all potential incubating infections, followed by vaccination ~7–10 days after treatment. Any animals becoming sick after initial treatment or vaccination should be retreated immediately and revaccinated a month later. Simultaneous use of antimicrobials and vaccine is inappropriate, because available commercial vaccines for animals in the US are live vaccines. Animals should be moved to another pasture away from where the bodies had lain and any possible soil contamination. Suspected contaminated feed should be immediately removed. Domestic production animals respond well to penicillin if treated in the early stages of the disease. Oxytetracycline administered daily in divided doses also is effective. Other antimicrobials, including amoxicillin, chloramphenicol, ciprofloxacin, doxycycline, erythromycin, gentamicin, streptomycin, and sulfonamides, also can be used, but their effectiveness in comparison with penicillin and the tetracyclines has not been evaluated under field conditions.
In addition to treatment and vaccination, specific control procedures are necessary to contain the disease and prevent its spread. These include the following:
notification of the appropriate regulatory officials
rigid enforcement of quarantine (after vaccination, 2 weeks before movement off the farm, 6 weeks if going to slaughter)
prompt disposal of dead animals, feces, bedding, or other contaminated material by cremation (preferable) or deep burial
isolation of sick animals and removal of well animals from the contaminated areas
cleaning and disinfection of stables, pens, milking barns, and equipment used on production animals
use of insect repellents
control of scavengers that feed on animals dead from the disease
observation of general sanitary procedures by people who handle diseased animals, both for their own safety and to prevent spread of disease
Contaminated soils are difficult to completely decontaminate, but formaldehyde will be successful if the level is not excessive. The process generally requires removal of soil.
Human infection is controlled by reduction of infection in production animals, veterinary supervision of animal production and slaughter to reduce human contact with potentially infected production animals or animal products, and, in some settings, either pre- or postexposure prophylaxis. In countries where anthrax is common and vaccination coverage in production animals is low, humans should avoid contact with production animals and animal products that were not inspected before and after slaughter. In general, consumption of meat from animals that died suddenly, meat obtained via emergency slaughter, and meat of uncertain origin should be avoided.
Routine vaccination against anthrax is indicated for individuals engaged in work involving large quantities or concentrations of B anthracis cultures or activities with a high potential for aerosol production. Laboratory workers using standard Biosafety Level 2 practices in the routine processing of clinical samples are not at increased risk of exposure to B anthracis spores.
The risk for workers who come into contact with imported animal hides, furs, bone meal, wool, animal hair, or bristles has been reduced by improvements in industry standards and import restrictions. Routine preexposure vaccination is recommended for people in this group only when these standards and restrictions are insufficient to prevent exposure to anthrax spores.
Routine vaccination of veterinarians in the US is not recommended because of the low incidence of animal cases. However, vaccination may be indicated for veterinarians and other high-risk individuals handling potentially infected animals in areas where there is a high incidence of anthrax cases.
The CDC recommends that those at risk of repeated exposure to B anthracis spores in response to a bioterrorism attack be vaccinated. Those groups include some emergency first responders, federal responders, and laboratory workers. Vaccination in anticipation of a terrorist attack is not recommended for other populations.
For humans, postexposure prophylaxis is recommended after an aerosol exposure to B anthracis spores. Prophylaxis may consist of antimicrobial therapy, a combination of antimicrobial therapy and vaccination, and sometimes monoclonal antibodies.
Key Points
Bacillus anthracis forms highly resistant spores that can persist in the environment for decades and infect grazing animals.
Anthrax develops without apparent clinical signs, with sudden death due to acute or hyperacute septicemia and leakage of uncoagulated blood from natural openings.
Humans usually acquire infection after exposure to infected animals, carcasses, or animal products.
Treatment with antimicrobials is effective if administered at an early stage of the infection.
Control measures include the correct disposal of carcasses, disinfection and decontamination of contaminated materials, and decontamination of the environment.
Vaccination of exposed animals and humans is the best practice to contain and prevent the disease.
Bacillus anthracis presents concern for animal and human disease from potential use as a bioterrorism agent.
For More Information
Anthrax. World Organisation for Animal Health
Anthrax. Centers for Disease Control and Prevention
Anthrax in humans and animals. World Health Organization


