

Urticaria, in its most common form, is an acute immune response resulting in multifocal dermal edema. Diagnosis is generally achieved via history, physical examination, and response to treatment. Urticaria may resolve spontaneously 12–48 hours after occurrence. It is generally treated with administration of an antihistamine and a glucocorticoid. Urticaria may be a precursor to anaphylaxis. In some cases, urticaria may be chronic or require a skin biopsy.
Urticaria (hives) is a common cutaneous reaction pattern characterized by variably pruritic, edematous lesions (wheals). Urticaria may occur in any mammal but is most often recognized in dogs and horses.
Etiology and Pathogenesis of Urticaria in Animals
Urticaria is the result of degranulation of mast cells and the subsequent release of histamine and other constituents into the dermis. Histamine release causes vasodilation and dermal edema.
Urticaria is generally an acute immune response (usually mediated by a type I hypersensitivity), often occurring within minutes of the stimulus. Urticaria may resolve without treatment, generally within 12–48 hours. It may recur frequently, depending on the underlying cause, and it may be chronic in rare cases.
Most commonly, urticaria occurs as a result of an insect bite (eg, from bees, wasps, hornets, mosquitoes, black flies, ants, spiders, or certain caterpillars), drug reaction, vaccine reaction, adverse food reaction, or seasonal environmental allergens (in horses in particular). The specific cause is often not identified.
Additional causes of urticaria include the following:
inhaled or contact allergen
mast cell neoplasia
plants (such as stinging nettle)
transfusion reactions
viruses
bacteria
fungi
parasites
In addition, exposure to topical medications or chemicals, such as carbolic acid, turpentine, carbon disulfide, or crude oil may induce urticaria. Foods, food additives, systemically administered drugs (such as penicillin, ampicillin, tetracycline, vitamin K, propylthiouracil, amitraz, ivermectin, moxidectin, and doxorubicin), and estrus may cause urticaria.
A unique form of urticaria in cattle has been described chiefly in the Channel Island cattle breeds (Jersey, Guernsey), which become sensitized to the casein in their own milk (“milk allergy”); it occurs in cases of milk retention or unusual engorgement of the udder with milk.
Not all causes of urticaria are immunologic. Nonimmunologic causes include the following:
heat or cold
exercise
pressure
dermatographism
psychological stress
Clinical Findings of Urticaria in Animals
Common lesions in urticaria include acute-onset, haired, dome-shaped wheals. Occasionally, urticarial lesions will become very large, linear, or even serpiginous.
Dermal edema is often multifocal, leading to 0.5- to 3-cm-diameter wheals; however, it may be diffuse, affecting large areas of dermis or subcutis. In severe cases, diffuse edema (angioedema) causes gross swelling of entire body regions such as the limb, face, or ventrum.
Urticaria can affect any area of the skin; however, some areas are more commonly affected than others.
In dogs, the head, limbs, trunk, and ventrum are commonly affected (see ).
In horses, wheals are observed mainly on the back, flanks, neck, eyelids, and legs (see ).
In sheep, lesions are usually evident only on the udder and hairless parts of the abdomen.
In pigs, eruptions occur around the eyes, between the hind legs, and on the snout, abdomen, and back.

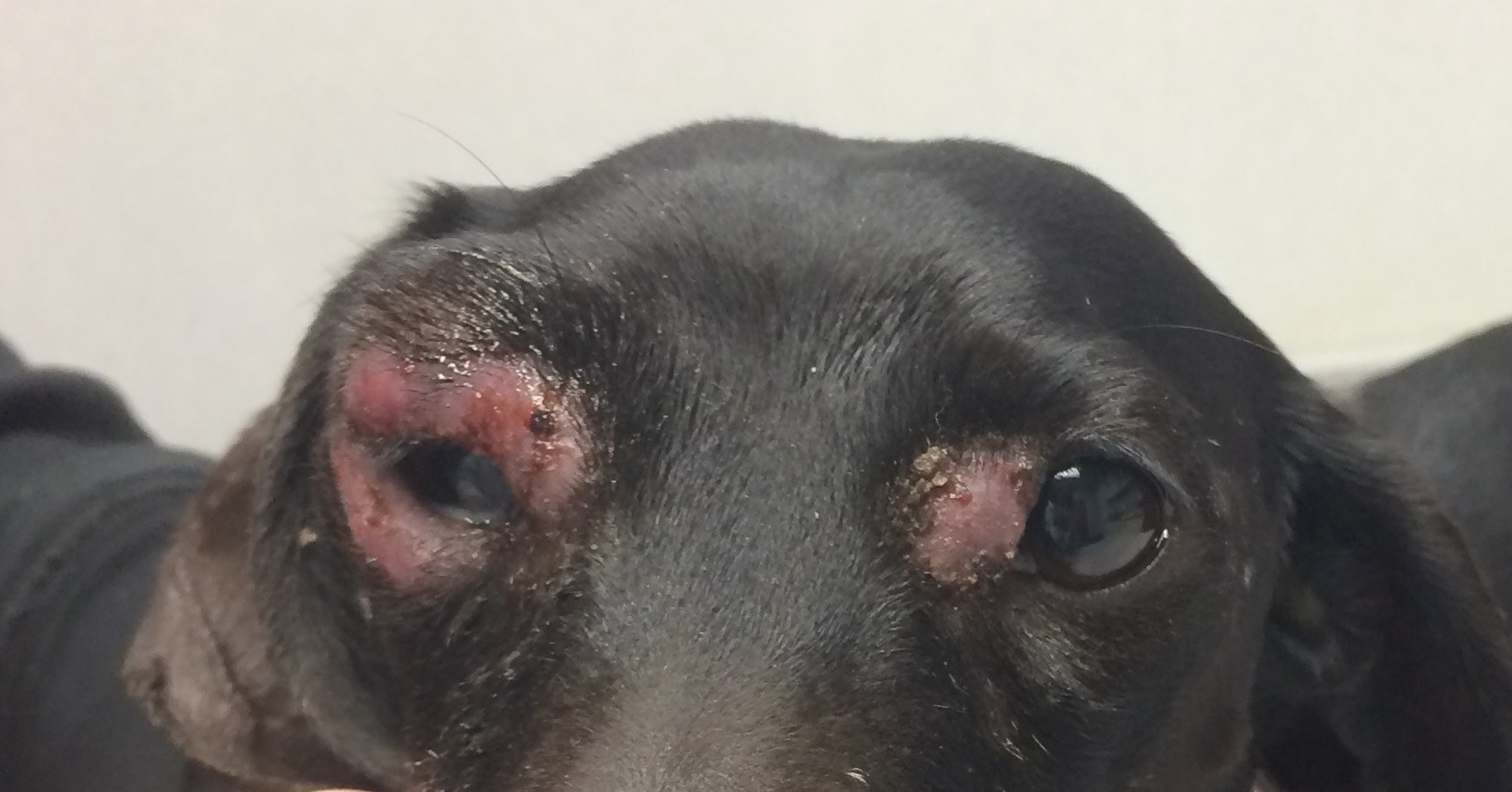
Courtesy of Dr. Nicole Heinrich.


Courtesy of Dr. Nicole Heinrich.
Urticaria may or may not be associated with pruritus. Large urticarial lesions and angioedema will pit when digital pressure is applied.
Diagnosis of Urticaria in Animals
History
Physical examination
Response to treatment
Skin biopsy in chronic or unusual cases
Diagnosis of urticaria can usually be made clinically, based on history, physical examination findings, and response to treatment:
The history of a patient with urticaria typically includes an acute onset of lesions that may or may not be pruritic.
Physical examination reveals wheals and/or angioedema that pits when digital pressure is applied. Wheals are haired, multifocal, and variably crusting; exudate and ulceration are generally not concurrent clinical signs.
Lesions subside quickly when a glucocorticoid is administered.
Extensive diagnostic procedures are not usually necessary. However, wheals that are chronic or accompanied by other clinical signs should be biopsied.
Potential differential diagnoses for urticaria include folliculitis and neoplasia. Differential diagnoses for angioedema include bacterial cellulitis, sterile granulomatous dermatitis and lymphadenitis (juvenile cellulitis), snakebite, neoplasia, and edema due to other causes.
Treatment of Urticaria in Animals
Antihistamines
Glucocorticoids
Mild cases of urticaria may spontaneously resolve within 12–48 hours. Treatment is generally initiated, however, because it is difficult to predict whether untreated urticaria will resolve or worsen over time. Generally, urticaria and angioedema respond quickly to treatment with glucocorticoids and antihistamines.
For dogs with urticaria, an antihistamine may be administered. Examples of antihistamines that may be effective include the following:
diphenhydramine (2–4 mg/kg, PO, every 8–12 hours for 3–5 days)
diphenhydramine (0.5–2 mg/kg, IM, once)
cetirizine (1–4 mg/kg, PO, every 24 hours for 3–5 days)
hydroxyzine pamoate (2 mg/kg, PO, every 12 hours for 3–5 days)
Loratadine and clemastine are not effective antihistamines for dogs. Responses to antihistamines in all species can vary considerably between individual animals.
Anecdotal experience suggests that additional treatment with a glucocorticoid will result in quicker resolution of urticaria compared with antihistamine alone, although research findings do not necessarily support this practice (1). Dexamethasone sodium phosphate may be administered (0.1 mg/kg, IV, once) in cases where swelling is severe or progressing rapidly. Administration of prednisone (0.5–1.0 mg/kg, PO, once) is generally sufficient for mild to moderate cases.
Although urticaria generally responds quickly to treatment, it may recur as the antihistamine and glucocorticoid are metabolized. Administration of an oral antihistamine for 3–5 days after initial treatment helps to prevent acute recurrence. In cats, prednisolone should be used in place of prednisone, and diphenhydramine should be avoided because it may cause paradoxical excitation.
For horses with urticaria, an antihistamine may be administered. Examples of antihistamines that may be effective include hydroxyzine pamoate (500 mg per horse, PO, every 12 hours for 3–5 days), pyrilamine (0.5–1.2 mg/kg, PO, every 12 hours for 3–5 days), and cetirizine (0.2–0.4 mg/kg, PO, every 12 hours for 3–5 days). For severe urticaria, dexamethasone may be administered (0.02–0.1 mg/kg; IV, PO, or IM; once) (2).
Glucocorticoids should be administered with caution in horses that are predisposed to laminitis. As in dogs, urticaria in horses may recur as the antihistamine and glucocorticoid are metabolized. Administration of an oral antihistamine for 3–5 days after initial treatment helps to prevent acute recurrence.
Urticaria can be a precursor to anaphylaxis. Anaphylaxis is a life-threatening condition characterized by systemic clinical signs and inadequate response to glucocorticoids. Epinephrine (0.01 mg/kg, IM, once, potentially repeated every 5–15 minutes; maximum dose of 0.3 mg total dose in dogs and cats < 40 kg and 0.5 mg total dose in dogs > 40 kg) is recommended for the initial treatment of anaphylaxis. Horses may receive epinephrine (0.01–0.02 mg/kg, IM or SC, once). Fluid therapy and other supportive care are essential for patients experiencing anaphylactic shock. Fatalities are rare.
Prevention of Urticaria in Animals
Prevention of urticaria is dependent upon avoidance of or desensitization to its underlying cause.
For insect bite–induced urticaria, several actions can be taken. An insect repellent should be applied to the affected animal daily. Permethrin products offer reasonable insect repellency and are available for dogs and horses. Permethrin products can be fatal to cats.
Protective clothing such as fly masks for horses can be helpful. Horses and other animals spending time outside should be kept away from environments that favor biting insects, such as low-lying areas with standing water and poor air circulation.
Daily administration of an antihistamine may be necessary for those animals that cannot avoid allergens or insects that induce urticaria. Mast cell stabilizers (eg, palmitoylethanolamide), allergen-specific immunotherapy, and omega-3 fatty acid supplementation can be helpful in preventing urticaria. In cases of recurrent or chronic severe allergic disease in dogs, immunosuppressive treatment such as oclacitinib or cyclosporine may be required.
Key Points
Mild cases of urticaria may resolve spontaneously and require little to no treatment, while severe cases can be a precursor of anaphylaxis.
Prevention of recurrent urticaria relies upon identification and avoidance of the underlying cause, or continuous treatment with antihistamine or other therapy.
References
Fosset FTJ, Lucas BEG, Wolsic CL, Billhymer AC, Lavergne SN. Retrospective evaluation of hypersensitivity reactions and anaphylaxis in dogs (2003-2014): 86 cases. J Vet Emerg Crit Care, 2023;33(5):577-586. doi:10.1111/vec.13319
Rashmir‐Raven AM. A review of physical urticarias in the horse. Equine Vet Educ. 2019;31(4):195-197. doi:10.1111/eve.12851
For More Information
Rostaher A, Hofer‐Inteeworn N, Kümmerle‐Fraune C, Fischer NM, Favrot C. Triggers, risk factors and clinico‐pathological features of urticaria in dogs: a prospective observational study of 24 cases. Vet Derm. 2017;8:39-46. doi:10.1111/vde.12342
Hill P. Canine urticaria and angioedema. In: Noli C, Foster A, Rosenkrantz W, eds. Veterinary Allergy, 2013; 195-200. doi:10.1002/9781118738818.ch30
Sauvé F. Can equine urticaria be cured?Can Vet J. 2020;61(9):1001.
Also see pet health content regarding hives in dogs, hives in cats, and hives in horses.


