

Embryo transfer in the equine industry has been primarily used to obtain offspring from mares with restricted reproductive potential (mares with undiagnosed subfertility, uterine disease, or simply older mares) or from performance mares that must remain nonpregnant to continue to train and compete. Most breed associations allow the registration of foals born by embryo transfer, and an increasing number now allow the registration of multiple foals born in the same year. Because of this relatively recent increased acceptance by breed registries, many horse breeders have obtained several foals in one breeding season from a single donor mare.
Superovulating mares with a purified form of equine follicle-stimulating hormone extract preparation (eFSH) to increase ovulation and embryo recovery rates is no longer commonly done commercially. Difficulties with manufacturing suitable gonadotropins and the variable response of mares to FSH stimulation have precluded widespread commercial use of this approach to produce equine embryos. It was thought that the low embryo recovery rate in mares ovulating >4 follicles/ovary could be attributed to an inability of the ovarian fossa to accommodate multiple ovulations in that area, or alternatively, excessive response to the FSH stimulation could result in dysmatured oocytes.
The horse embryo is notoriously challenging to cryopreserve, probably owing to its relatively large diameter and the presence of an embryonic capsule that limits interaction between cryoprotectant agents and the embryo. Embryos of morula or early blastocyst stage (< 6.5 days after ovulation) are preferable for cryopreserving, because after thawing, older embryos have invariably low morphological quality that results in poor pregnancy rates. A vitrification media for horse embryos is commercially available, and acceptable pregnancy rates varying from 40%–60% have been reported. Successful cryopreservation of expanded equine blastocysts also has been reported for embryos that had their blastoceles collapsed after embryo biopsy procedures (see video of embryo collapsing procedure).


Because one or two embryos are typically recovered from donor mares, breeding soundness evaluations must be done for both donor and embryo recipient mares. Daily ultrasonographic evaluation of the uterus and ovaries of donor and potential recipient mares during estrus provide critical information about the time of ovulation, which is essential for determining the day of ovulation and day of embryo collection and to assist in the selection of qualified recipient candidates for embryo transfer.
Nonsurgical techniques are currently used to collect and transfer horse embryos. Embryo collection is usually performed on day 7 or 8 (day 0 = ovulation). The use of good standard techniques generally results in a recovery rate of ~75%; this rate can be as high as 90% for young maiden or fertile mares or as low as 10%–20% in subfertile mares. Before embryo collection, palpation per rectum and ultrasonography are performed mainly to document the presence of the corpus luteum, the extent of cervical tone, and absence of any fluid in the uterus. Mild soap or povidone-iodine scrub can be used to wash the perineal region, followed by a thorough rinsing with clean water.
Sedation is not used in most cases but may be needed when working with uncooperative mares. Acepromazine should be avoided because it may cause relaxation of the uterus and potentially impair fluid recovery or manipulation of the reproductive tract during flushing of the uterus; sedation with an alpha2-adrenergic receptor agonist (eg, xylazine or detomidine) is preferred.
Embryo collection is performed via a routine transcervical uterine lavage procedure, using a silicone catheter with an inflatable cuff. Using sterile technique, the silicone catheter (measuring 28 to 34 in. long and 28F to 37F, depending on the size of the reproductive tract of the mare) is introduced through the cervix into the uterus, and then the balloon is inflated (typically 60–80 mL) with air or collection medium; the catheter is then gently pulled back so the cuff seals the internal cervical os. Complete flush media with antimicrobials, surfactant, and bovine serum albumin is available commercially and ready to use. Alternatively, as with cattle, flush media can be prepared with Dulbecco PBS solution and 1%–5% FBS; 1–2 L are infused into the uterus and then allowed to flow back into a graduated cylinder or plastic bucket to measure the recovered volume.
Once the uterus is filled, it can be gently manipulated per rectum to aid the recovery of fluid. An embryo filter equipped with a 75-mcm mesh is usually connected to the end of the outflow tubing to produce ~40–60 mL of fluid. In some cases, an injection of oxytocin (10 U, IM or SC) may be administered to minimize the retention of a large amount of flush media in the uterus. The recovered fluid should be clear and free of a noteworthy amount of debris and blood. Nearly 100% of the fluid used to lavage the uterus should be recovered. A total of 4–8 L of flush media is used to complete the embryo collection procedure (flush). If retention of fluid is suspected or if the outflow of media is interrupted, transrectal ultrasonography may be used to assess the presence of intraluminal fluid. A common cause of interrupted outflow drainage of flush media results from placing the tip of the catheter intracervically and not in the body of the uterus: the media easily flow into the uterus but not outward.
Once the flush is completed, the remaining fluid in the filter is searched in a sterile dish with grid under a magnification of 15× using a stereomicroscope. Once the embryo is found, it is transferred to a well in a sterile tissue culture dish containing holding media (commercial, ready-to-use with 0.4% albumin or made with Dulbecco PBS solution plus 10%–20% FBS). The embryo should be washed at least 3 times by transferring into two other wells previously filled with holding media. Embryo manipulation is done with a 0.25-mL straw connected to a tuberculin syringe with a 16-gauge needle, a 0.5-mL straw directly connected to a tuberculin syringe, or a capillary pipette (20 mcL) attached to a tuberculin syringe. After being washed, the embryo should be transferred to a recipient mare (within 1 hour) or prepared for short storage and transportation. The stage of the embryo (morula, early, or expanded blastocyst) and quality (1, best; 5, dead) should be recorded.
Although surgical transfer of equine embryos was once thought to produce higher pregnancy rates than nonsurgical transfer techniques, the latter are now the preferred method to transfer horse embryos. Recipient mares should be reproductively sound and in good body condition and health. Synchronization of ovulation should be maximized by hormonal manipulation of the estrous cycle and daily transrectal ultrasonographic evaluation. Good pregnancy rates result from using recipients that have ovulated from 1 day before to 3 days after the donor. In addition, progestagens such as altrenogest may be used until the day of pregnancy examination 4–5 days after the transfer (~12–13 days of gestation).
The nonsurgical embryo transfer is performed using transcervical catheterization. Plastic straws (0.25 or 0.5 mL) are used to load the embryo; the column of medium containing the embryo should be surrounded by two small columns of air, which are in turn surrounded by two columns of medium. The straw loaded with the embryo is fitted into an embryo transfer gun. Embryo transfer sheaths with side delivery can minimize embryo damage during the transfer procedure.

Courtesy of Dr. Carlos Pinto and LSU Comparative IVF Laboratory.
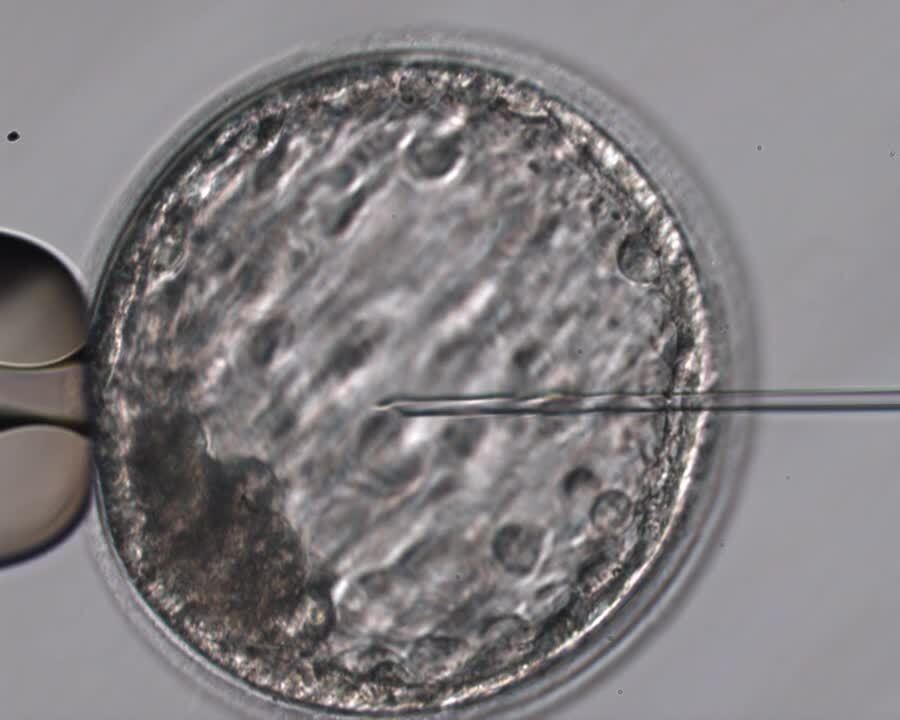
A recent advance in embryo transfer technologies in commercial settings has been the possibility of producing in vitro equine embryos using intracytoplasmic sperm injection (ICSI) using immature oocytes collected via ovum pick-up (OPU). Frozen semen from deceased stallions can be efficiently used to produce in vitro embryos by using only a portion of a frozen semen straw to provide sperm for the ICSI procedure. The number of foals born after transfer of OPU-ICSI equine embryos has been increasing substantially over the past 10 years.
Developed in the 1990s, OPU-ICSI has been increasingly used to produce embryos in vitro, now in routine use by several laboratories in the US, Europe, and South America. Acceptance of this assisted reproductive technology mirrors the time most breed registries took to accept the use of artificial insemination and embryo transfer to produce foals.
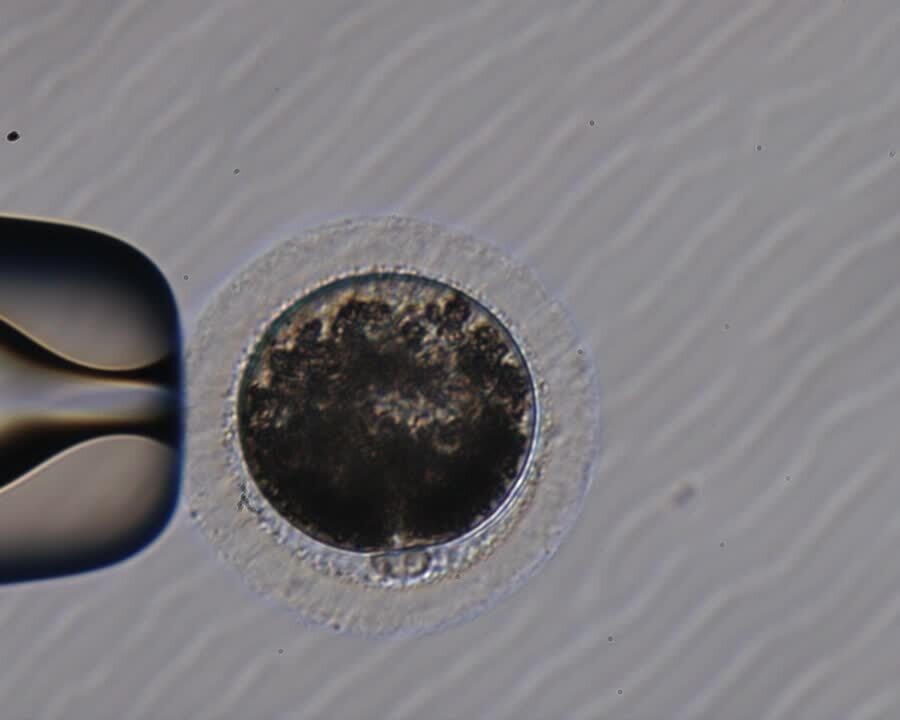
Briefly, immature oocytes are collected from nonstimulated donor mares and subjected to in vitro maturation either immediately after retrieval or after being held for < 24 hours in regular embryo holding media; holding oocytes before placing them on in vitro maturation media helps with the scheduling of the in vitro insemination procedure (ICSI) at a convenient time for the laboratory staff, typically 24–28 hours after being incubated on in vitro maturation media. Holding oocytes does not seem to be detrimental to embryo production, based on cleavage and blastocyst production rates.
Embryos are cultured for at least 7 days and invariably transferred only at the blastocyst stage. The use of recipient mares that are on day 4–6 of diestrus seem to result in optimal pregnancy rates. Although the success of OPU-ICSI can be greatly vary, ~1 transferable blastocyst embryo is being produced on average per OPU-ICSI session, with 60%–70% recipient mares becoming pregnant after transfer of one embryo. Most recently, the pregnancy success of transfer of frozen-thawed OPU-ICSI embryos has been ~50%.
Preparation for Short Storage and Transport for Embryo Transfer in Horses
Horse breeders without an adequate number of recipients and veterinarians with modest investment in equipment can collect embryos and prepare them for short storage and transport to a centralized embryo transfer facility.
Pregnancy rates do not appear to differ from those obtained with fresh embryos, especially if embryos are shipped counter-to-counter on the same day they are collected. Embryos are routinely shipped in commercially available holding media that are ready-to-use preparations containing 0.4% bovine serum albumin and antimicrobials. The embryo is placed into a 2-mL polypropylene cryotube vial or a 5-mL snap-cap tube that contains the holding media. The tube with the embryo is then placed into a semen shipping container designed to cool and transport horse semen. The container is preferably shipped to an embryo transfer facility on the same day the collection is performed using an airline carrier (counter-to-counter) or processed for overnight delivery using a commercial carrier.





