

Ascarids
The larvae of some ascarid roundworms, including Toxocara spp of dogs and cats and Baylisascaris spp of mustelids, can cause CNS disease.
Nervous system disorders frequently associated with ascarid infection in young dogs include focal CNS lesions caused by the death of aberrant arrested larvae of T canis. Toxocara larvae may also invade the eye and cause ocular larva migrans in animals and humans.
Baylisascaris procyonis is the ascarid found in the small intestine of raccoons. It causes larva migrans in both wild and domestic animals in North America and is usually associated with clinical signs of CNS disease. More than 90 species of wild and domesticated animals have been identified as being capable of serving as paratenic (transport) hosts harboring B procyonis larvae. Some species, including opossums, skunks, cats, pigs, sheep, and goats, appear to be marginally susceptible or resistant to neurologic migration. This parasite has also been associated with cerebrospinal nematodiasis in humans, particularly children; including as a cause of ocular larva migrans.
Filarids
Dirofilaria immitis is often referred to as the canine heartworm but can also infect cats and ferrets. As adults, these parasites usually infect the right ventricle and the pulmonary artery and its fine branches. In its definitive hosts, D immitis has also been recovered from a variety of aberrant sites, including the CNS and the anterior chamber of the eye.
Elaeophora schneideri, a filarid affecting the carotid arteries and its branches, is common in mule deer, primarily in western North America. Microfilariae accumulate in the skin of the head and face; intermediate hosts are tabanid horseflies. Larvae develop in arteries of the leptomeninges before migrating to the carotid arteries. Infection is usually asymptomatic in healthy definitive hosts. In wapiti, moose, white-tailed deer, sheep, and goats, worms in the arteries cause degeneration and loss of the endothelium and accumulation of plasma proteins and platelets on and within the intima. Thrombosis, infiltration of the intima, and fibroblastic proliferation may eventually result in occlusion and ischemic necrosis in associated tissues. Necrotic lesions associated with occlusion of leptomeningeal arteries are commonly found in the brain. Neurologic signs include blindness, head deviation, circling, ataxia, and paralysis (also see Elaeophorosis in Animals).
Setaria digitata is found in Asia and is a common parasite of the peritoneal cavity. Microfilariae are found in the blood; mosquitoes are intermediate hosts. Details of development in the normal host are unknown. In cattle, clinical signs do not appear to occur. In horses, goats, and sheep, the developing worms invade the CNS and cause motor weakness, ataxia, lameness, drooping eyelids or ears, and lumbar paralysis. Histologic lesions include focal malacia and degeneration of axis cylinders and myelin sheath in all regions of the CNS.
Setaria cervi has been reported in the leptomeninges of deer in Europe and in Russia and the former Soviet states, often in association with Elaphostrongylus cervi. Setaria spp have also been found in the CNS of horses. The clinical importance of these findings is unclear.
Filarids may also parasitize avian species. Splendidofilaria quiscula is found in the cerebral hemispheres of grackles (Quiscalus quiscula) and other birds in North America. Paronchocerca helicina may be found in the cranial leptomeninges of the snake bird (Anhinga anhinga) in the US.
Metastrongyles
Angiostrongylus cantonensis (rat lungworm) is a common parasite of rats (Rattus species) in southeast Asia and Australia and has spread across the Pacific to both North and South America. It continues to spread to new regions and countries. Terrestrial, aquatic, and amphibious snails and slugs are intermediate hosts. Paratenic hosts are freshwater prawns, land crabs, coconut crabs, and planarians. Larvae invade the cerebrum and develop in the neural parenchyma for ~2 weeks, then enter the subarachnoid space and migrate, ~1 month after infection, to the pulmonary arteries via the venous circulation. Neurologic signs are rare in rats. In endemic areas, humans frequently acquire infections by consuming raw or undercooked intermediate or paratenic hosts often disguised on vegetables. In humans, this parasite may produce fatal eosinophilic meningoencephalitis. In Australia and Hawaii, A cantonensis is known to produce an ascending paralysis in dogs, canine neuroangiostrongylosis.
Gurltia paralysans is found in the spinal veins of cats and has reportedly produced a high incidence of paralysis. It may also be an incidental parasite in cats.
Elaphostrongylus cervi is a common parasite of the skeletal musculature of Rangifer and Cervus spp (reindeer and elk) in the holarctic region, especially Eurasia. It is transmitted via terrestrial snails and slugs and apparently develops for a time in the CNS before migrating to the muscles. Infection is associated with lumbar weakness, paresis, and paralysis in cervids in Sweden and in Russia and the former Soviet states.
Skrjabingylus nasicola and S chitwoodorum are found in the frontal sinuses of mustelids, especially mink, weasels, and skunks. Larvae acquired from terrestrial snails and slugs develop for a time in the gut wall, then migrate to the spinal cord. They move on to the leptomeninges to the brain and along the olfactory tracts to the cribriform plate, which they penetrate to reach the frontal sinuses. Their presence on the leptomeninges elicits hemorrhage and leptomeningitis. In heavy infections, some subadult worms may invade the brain and cause neurologic signs, including paralysis.
References
Rat lungworm. Entomology and Nematology Department, University of Florida. Accessed April 21, 2022. https://entnemdept.ufl.edu/creatures/nematode/rat_lungworm.htm
Meningeal worm (Parelaphostrongylus tenuis)

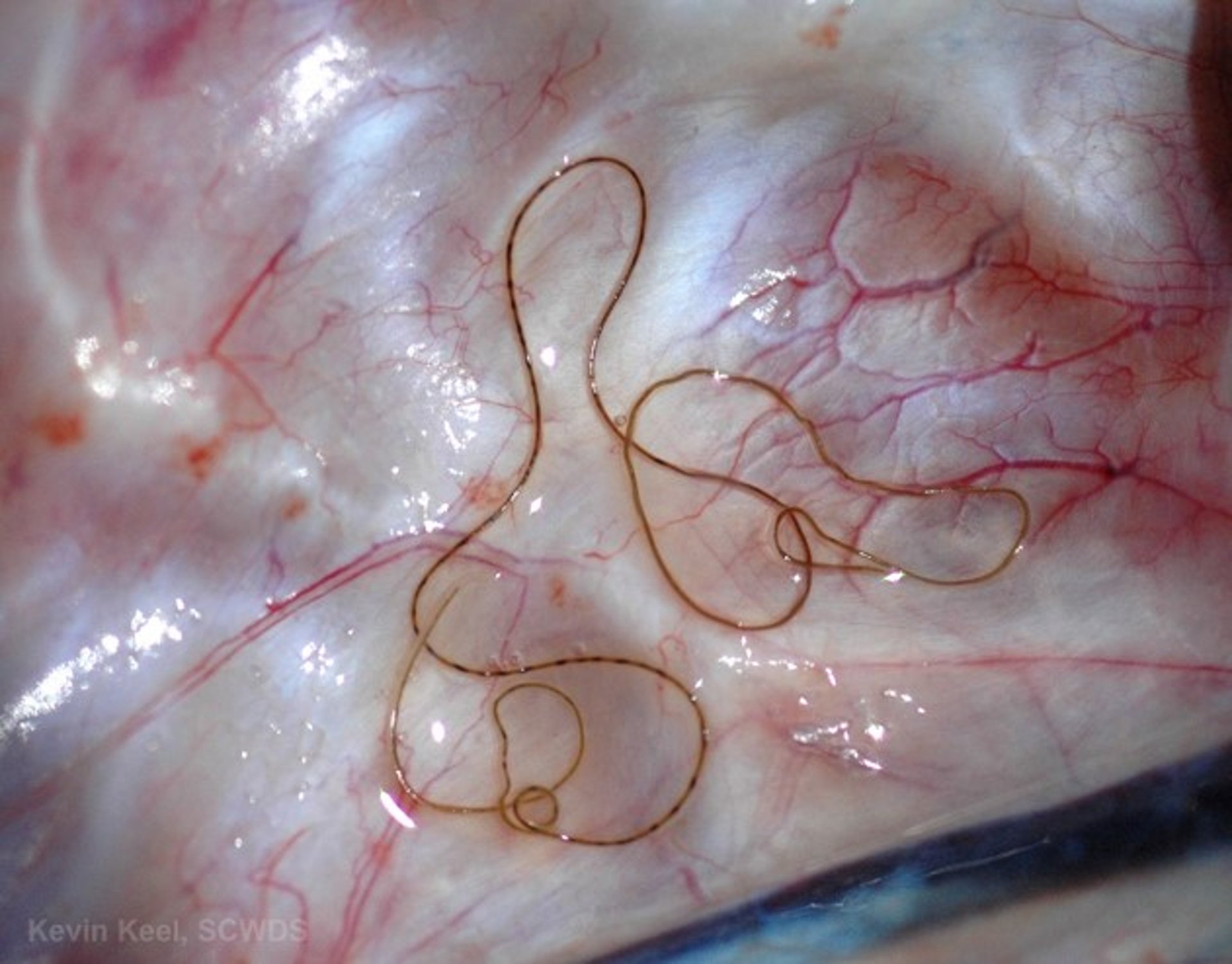
Adult meningeal worm on the meninges of a white-tailed deer.
Courtesy of Dr. Kevin Keel.

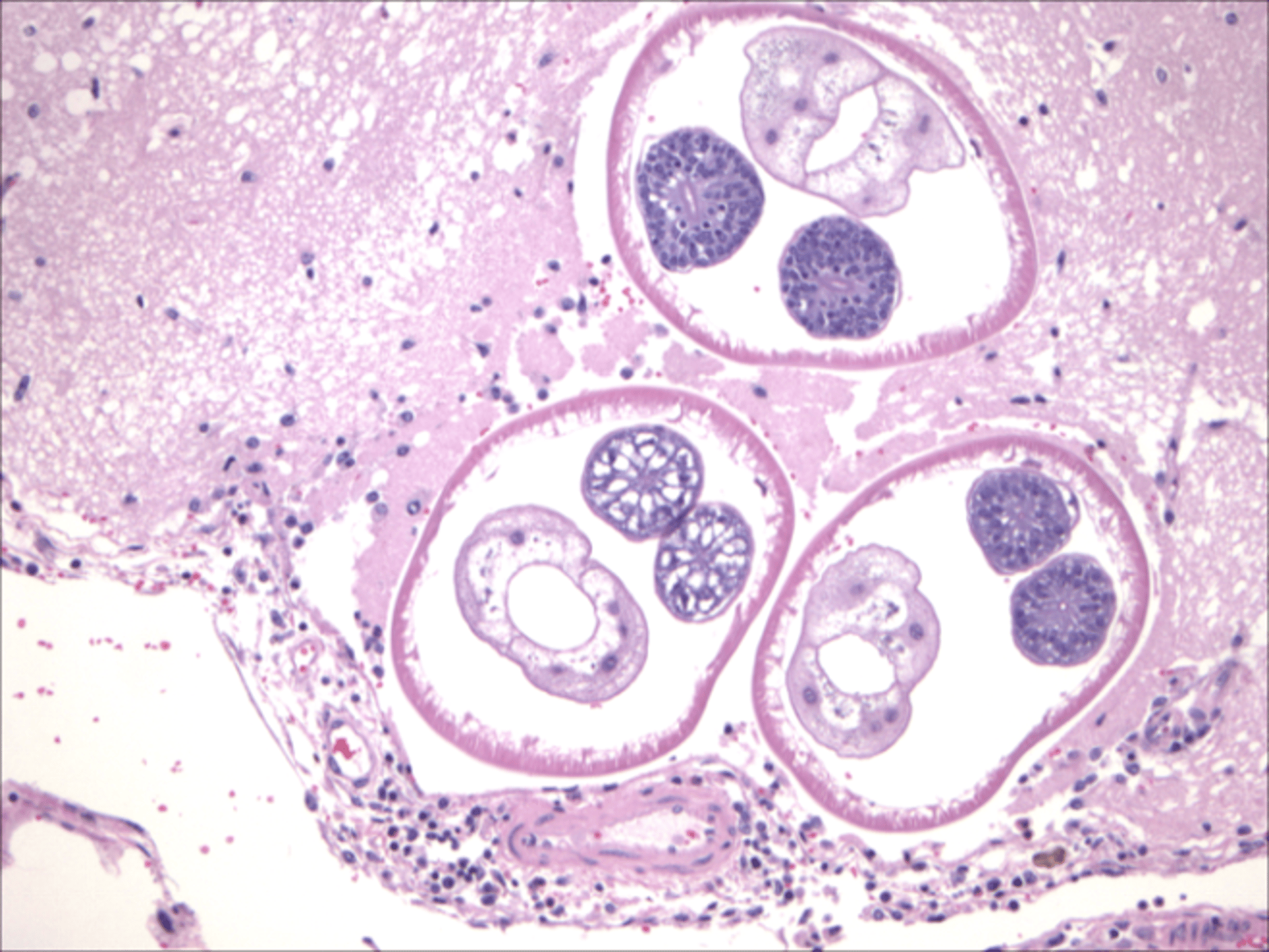
Parelaphostrongylus tenuis within the cerebrum of a sika deer with neurologic disease.
Courtesy of Dr. Kevin Keel.
Parelaphostrongylus tenuis is a metastrongylid nematode often referred to as brain worm or meningeal worm, given its location in vertebrate hosts. Adult nematodes are long and threadlike, with females up to 9 cm long X 0.25 mm wide. In the definitive host, white-tailed deer, adult nematodes are found in the veins and venous sinuses of the cranial meninges as well as free in the cranial subdural space. Generally, P tenuis infection causes little to no disease in white-tailed deer.
The Parelaphostrongylus tenuis life cycle includes two distinct hosts. White-tailed deer excrete the live L1 larvae in feces. Several terrestrial gastropods (eg, snails, slugs) serve as the required intermediate hosts by ingesting the L1 larva in deer excrement or where dispersed into the soil. The nematode matures to the infective third larval stage (L3) within the gastropod in approximately four weeks at temperatures between 18° C and 30° C. White-tailed deer are infected with P tenuis by ingestion of a gastropod while grazing; L3s released from the gastropod penetrate the abomasal wall and travel via spinal nerves to the spinal cord, where they molt to L4. The L4 move into the subdural space and then migrate to the cranium, where they complete their development in the meninges, mate, and lay eggs. Eggs travel to the lungs, where they hatch to L1 stage, are coughed up, swallowed, and eventually defecated.
Clinical Signs, Pathogenesis, and Diagnosis in Accidental Hosts
In accidental hosts, including moose, elk, caribou, llamas, alpacas, horses, cattle, sheep, goats, antelope, and Guinea pigs, P tenuis does not migrate to the appropriate meningeal tissue and instead migrates through the nervous tissue in either the brain or spinal cord or both. Neurologic damage to the animal occurs by both mechanical injury and inflammation. Resulting clinical signs are nonspecific and includes
rear leg paresis
ataxia
circling
head tilt
inability to stand
cervical scoliosis
blindness
The signs depend on the location within the CNS where parasite migration occurs. There are rare reports of elk, and to a lesser extent moose, serving as patent hosts, with L1 larvae found in the feces.
Currently, the most reliable diagnosis of P tenuis in aberrant hosts entails a necropsy in which worms or migration tracts and associated lesions are observed in the brain or spinal cord. Examination of CSF from affected animals may demonstrate eosinophils, and previous research indicated that camelids with neurologic disease and more than 17% eosinophils in CSF had a high probability of P tenuis if the animal originated from a region where P tenuis is endemic.
Treatment and Control
Prevention of P tenuis in livestock is much more effective than treatment. Prevention may include use of fences to exclude deer from sensitive species, the use of livestock guardian dogs to discourage deer from approaching a fence, and use of rocks lining the outside of the fence. In addition, molluscicides may be applied to the rock bed to prevent entry of gastropods into pasture.
The use of monthly injectable ivermectin has been used to prevent P tenuis infection; however, unintentional side effects of this include selection of ivermectin-resistant GI nematodes, which can lead to high morbidity and potentially mortality. Treatment of infected animals is often expensive and unrewarding. If P tenuis infection is suspected, treatment should be attempted as early as possible before clinical signs progress. If animals are unable to or have difficulty standing, they should be placed in a sling, generally at a veterinary college or referral hospital. Treatment of camelids generally consists of fenbendazole (50 mg/kg, PO for 5 days) and NSAIDs. Vitamin E and antibiotics have also been used, but their effectiveness is unknown. Corticosteroids should be avoided in treatment of suspect P tenuis cases. Owners should be warned that animals showing clinical signs of P tenuis have a poor prognosis.
Finally, the movement of cervids should be minimized or prohibited, particularly from the parasites' endemic location in the eastern and midwestern US to the mountain and western locations or regions of Canada where the parasite is not known to exist, to limit the spread of P tenuis into new areas.
Canine neuroangiostrongylosis
Etiology of Canine Neuroangiostrongylosis
Canine neuroangiostrongylosis (neural angiostrongylosis), or rat lungworm disease, is due to aberrant migration of rat lung worm (Angiostrongylus cantonensis) in the central nervous system (CNS) of dogs. Infection occurs after ingestion of the intermediate host—snails and slugs, and less commonly after ingestion of transport hosts—planarians, centipedes and reptiles. Rat lungworms do not generally reach sexual maturity in dogs.
Pathogenesis and Clinical Findings of Canine Neuroangiostrongylosis
Canine neuroangiostrongylosis is characterized by lumbosacral and caudal weakness, with a mix of lower and upper motor neuron signs. Clinical signs progress cranially. A prominent clinical sign is adoption of a hunched posture due to marked hyperesthesia. In some dogs it leads to an aggressive and disproportionate response to stimuli such as spinal or caudal manipulation. Clinical signs appear 10–12 days after ingestion of the infective larvae. The most likely causes for clinical signs are mechanical trauma due to migration of the larvae and the host response to dead or dying larvae.


Canine neuroangiostrongylosis is present in eastern Australia and Hawaii. In Australia, dogs are most commonly affected in the fall, and puppies make up a preponderance of the cases. In other countries where A cantonensis has been introduced it may be unrecognized.
Diagnosis of Canine Neuroangiostrongylosis
Definitive diagnosis requires CSF testing for detection of A cantonensis DNA
History of ingesting a slug or snail by the dog is suggestive. Peripheral eosinophilia is suggestive but hardly specific, as it may be due to intestinal parasites or ectoparasites. Marked eosinophilic pleocytosis in cerebrospinal fluid is strongly suggestive of canine neuroangiostrongylosis based on reports from Australia and Hawaii. Detection of A cantonensis DNA using qPCR assay confirms the diagnosis. CSF serologic testing can also be helpful.
Treatment and Control of Canine Neuroangiostrongylosis
Administration of glucocorticoids and supportive care
Fenbendazole may assist recovery
No specific preventive product exists
Glucocorticoids are administered to reduce the inflammation associated with dead or dying larvae in CNS. Supportive care is also indicated. In dogs, there is a consensus that administration of glucocorticoids is useful and effective. Initially, administration via parenteral route is advisable as dosing can be painful in severely affected individuals. Whether administration of anthelmintics aids or worsens the disease process in aberrant hosts such as dogs is equivocal. In most cases of canine neuroangiostrongylosis, analgesia is required. Opioids are indicative because of the magnitude of the hyperaesthesia, although in some cases neuropathic pain is a feature and requires other strategies (eg, gabapentin). Supportive care such as bladder evacuation is important for severely affected cases. Antimicrobials are considered in cases when bacteria have been translocated with the migrating larvae in combination with high doses of glucocorticoids.
Rhabditoids
Halicephalobus deletrix is a free-living soil rhabditiform associated with soil and decaying vegetation in the host's environment. This nematode has been reported in the CNS of horses and humans. It may reach the CNS via soil contamination of wounds or through abscesses in the oral and nasal cavities. It multiplies in the CNS and is highly destructive to neural tissues. It may also transport pathogenic microorganisms to the CNS. Clinical signs are related to the location of and lesions produced by the parasitic infection. Clinical signs resemble viral encephalitis and include motor weakness, ataxia, head deviation, circling, depression, blindness, drooping of the ears or eyelids, loss of the herding instinct, and paralysis. Histologic lesions consist of vasculitis, hemorrhagic necrosis, and malacia.
Miscellaneous Nematodes
Migrating larvae of strongyles (possibly Strongylus vulgaris) have been reported in the CNS of horses. Larvae of Stephanurus dentatus rarely invade the CNS of pigs. Larvae of Trichinella spiralis have been reported post-mortem in the brain in a fatal case of trichinosis in a human patient. Larvae of Strongyloides stercoralis may invade the brain of experimentally infected animals. Gnathostoma spinigerum has been found rarely in the CNS of humans. Eustrongylides ignotus implanted subcutaneously in rats and chickens migrated to the CNS, and caused death of the host.
For More Information





