




Rabies is an acute, progressive encephalomyelitis caused by lyssaviruses. This zoonosis occurs worldwide in mammals, with dogs, bats, and wild carnivores as the principal reservoirs. Typical clinical signs include acute behavioral changes and progressive paralysis. The disease is fatal once clinical signs appear; however, appropriate and timely administration of local wound care, immune globulin, and vaccination can prevent disease in unvaccinated humans after exposure. Vaccines are available for domestic animals, wildlife, and humans to prevent rabies and to help control transmission in reservoir populations.
Rabies is a fatal viral zoonosis and serious public health concern. The disease principally affects carnivores and bats, although any mammal can be affected.
Etiology of Rabies in Animals
Rabies is caused by viruses in the genus Lyssavirus in the family Rhabdoviridae. Globally, rabies virus is the most important member of the genus. Information regarding the diagnosis, pathogenesis, clinical signs, and prevention of rabies virus infection is generally applicable to other lyssaviruses as well.
Classification of Viral Genome
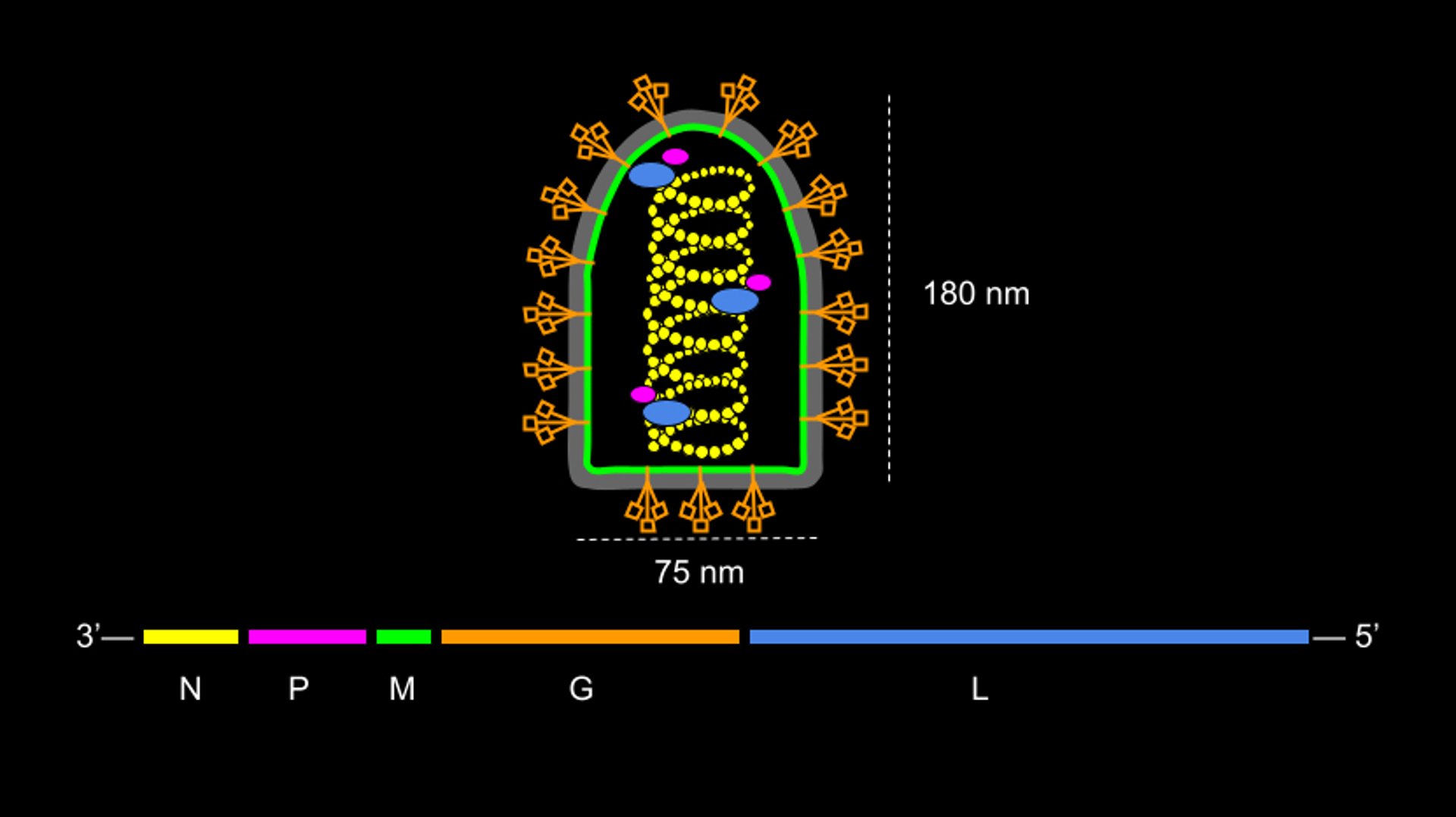
Rabies virus has a nonsegmented single-stranded negative-sense RNA genome (~12 kb) encoding five viral proteins:
nucleocapsid protein (N)
matrix protein (M)
glycoprotein (G)
large protein (L), the enzymatically active RNA-dependent RNA polymerase
phosphoprotein (P), L protein's cofactor

Courtesy of Dr. Nicholas Roman.
Besides rabies virus, the International Committee on Taxonomy of Viruses lists 16 other species in the genus Lyssavirus, demarcated according to their genomic sequences. Additional putative novel species have been reported but have yet to be fully characterized.1
Structure
Rabies virus is an enveloped virus; lipid bilayer primarily derived from host cell membrane comprises the outer envelope, which is lined by the matrix protein. Virions are distinctively bullet-shaped and measure approximately 75 nm wide and 180 nm long.
The surface of the virion is covered with transmembrane trimeric glycoprotein spikes, which recognize and bind cell receptors. Internally, the genomic RNA is encapsidated to form a helical ribonucleoprotein closely associated with a viral RNA polymerase complex.
Replication
Rabies virus replicates by budding from host cell membranes. Following adsorption via receptor-virion interaction, free virus particles infect new cells by fusing their envelopes with the host cell membrane, allowing entry of viral genetic material. Messenger RNA is transcribed from the RNA genome.
Translation into proteins occurs on free ribosomes, and viral nucleocapsid develops in the cytoplasm. Complete viral particles may be formed at the cell surface but more commonly bud from intracytoplasmic membranes.
Pathogenic Mechanisms
Rabies virus replicates initially in non-nervous tissue at the site of inoculation.
Lyssaviruses such as rabies virus are highly neurotropic. Rabies virus travels via the peripheral nerves to the spinal cord and ascends to the brain. After reaching the brain, the virus travels via peripheral nerves to the salivary glands and other organs.
If an animal is capable of transmission via its saliva, virus will be detectable in the brain. Virus is shed intermittently in the saliva.
Near the end of the clinical phase, after replication in the CNS, rabies virus may be found in nearly every innervated organ.
Epidemiology of Rabies in Animals
Identification of different virus variants by laboratory procedures, such as monoclonal antibody analysis or genetic sequencing, has greatly enhanced understanding of rabies epidemiology.
Rabies virus is adapted to its reservoir host, and antigenically distinct rabies virus variants are maintained within specific animal reservoir species (eg, the virus variant associated with rabies maintained by dog-to-dog transmission is termed the canine rabies virus variant).
Generally, each rabies virus variant is responsible for virus transmission between members of a major reservoir species in the geographic area in which it is enzootic. However, cross-species transmission of rabies virus variants does occur (eg, rabies in a dog as a result of infection with a variant from a skunk would be referred to as skunk rabies virus variant infection in a dog).
At least 30 species are known reservoirs, primarily terrestrial carnivores, hematophagous bats, and insectivorous bats. Globally, the dog is the most important reservoir, particularly in Asia and Africa.
In North America, distinct virus variants are responsible for rabies perpetuation in red and Arctic foxes in Canada and Alaska, raccoons along the eastern seaboard from Maine to Florida, and gray foxes in the southwest, including Arizona and New Mexico.
Two variants are responsible for rabies in striped skunks, one in the south-central states and the other in the north-central states, often extending into the Canadian prairies. Another skunk rabies virus variant is found in California.
By comparison, the epidemiology of rabies in bats is complex. In general, each variant found in bats may be characterized with a predominant bat species. Spillover from bats to other mammals occurs infrequently.
Most indigenous human cases of rabies in the US are due to bat rabies virus variants (especially viruses associated with Lasionycteris noctivagans, the silver-haired bat; Perimyotis subflavus, the tricolored bat; and Tadaridabrasiliensis, the Brazilian free-tailed bat).
Geographic Distribution
Rabies is found throughout the world, with the exception of Antarctica. A few countries claim to be free of the disease because of either successful elimination programs or thanks to island status and enforcement of rigorous quarantine regulations.
Rabies emergence may be affected by changes in virus-host dynamics or human translocation of infected species. For many years, skunks were the most commonly reported rabid animal in the US; however, in 1990, raccoons became the most numerous rabid carnivore.
The canine rabies virus variant became established in dogs and coyotes (Canis latrans) in Texas but was eliminated by the beginning of the 21st century. The canine rabies virus variant exists in Africa, Asia, the Middle East, and parts of Central and South America and the Caribbean, with the potential to spread throughout the US if reintroduced.
Skunk, raccoon, and fox rabies virus variants are each found in fairly distinct geographic regions of North America, although some overlap occurs. Bat rabies virus variants are distributed throughout the Americas. The vampire bat is an important reservoir in Latin America and is the source of multiple outbreaks in cattle, as well as in humans, particularly in parts of Amazonia.
In western Europe, the red fox rabies virus variant predominated before its elimination thanks to oral vaccination efforts. In parts of eastern Europe, rabies in raccoon dogs is of increasing concern. Bat rabies virus variants, maintained by several lyssaviruses in insectivorous chiropterans, appear to be widely distributed throughout Europe.
Other wildlife play an important role in the transmission of rabies virus in certain areas, including different species of mongooses in the Caribbean, southern Africa, and parts of Asia; jackals in parts of Africa; marmosets in Brazil; and ferret badgers in China.
Incubation Period
The incubation period of rabies is both prolonged and variable, depending on the exposure site and dose of viral inoculum. Exposure of highly innervated tissue is associated with a shorter incubation period for the development of CNS signs.
Typically, rabies virus remains at the inoculation site for a considerable time. The unusual length of the incubation period helps to explain the effective action of local infiltration of rabies immune globulin during human postexposure prophylaxis, even days after exposure.
Most clinical cases of rabies in dogs develop within 21–80 days after exposure; however, the incubation period may be shorter or considerably longer. One recorded case of rabies in a person in the US had an incubation period estimated reliably to be > 8 years.
Transmission Dynamics
A predominant animal reservoir is the principal source of rabies virus transmission (eg, infected dogs are the are the main reservoir for disease transmission in Asia and Africa). All animal reservoirs are also vectors of the virus; however, not all vectors are reservoirs. For example, although cats can effectively transmit rabies virus, no cat-to-cat transmission of rabies virus perpetuates, and no unique feline rabies virus variant has been documented.
Nonetheless, cats are the most commonly reported rabid domestic animal in the US. Virus is present in the saliva of rabid cats, and humans have developed rabies after being bitten by rabid cats. Reported cases in domestic cats have outnumbered those in dogs in the US every year since 1990.
Transmission of rabies virus almost always occurs via introduction of virus-laden saliva into tissues, usually by the bite of a rabid animal. Although much less likely, virus from saliva, salivary glands, or neural tissues can also cause infection by entering the body through fresh wounds or intact mucous membranes.
Saliva is infectious at, or before, the time clinical signs occur. Domestic dogs, cats, and ferrets may shed virus up to 10 days before onset of clinical signs; viral shedding in wildlife has been reported for several weeks before onset of signs.
Rabies virus has not been isolated from skunk musk (spray).
Hematogenous transmission does not occur.
According to the US Advisory Committee on Immunization Practices, under most circumstances, there is no danger of aerosol transmission of rabies virus.3 However, aerosol transmission has occurred under very specialized conditions in which the air contained a high concentration of suspended particles or droplets containing viral particles. Such conditions have been responsible for laboratory transmission under less than ideal containment situations.
There has been a suggestion of very rare natural aerosol transmission in a cave inhabited by millions of bats. Oral and nasal secretions containing virus were probably aerosolized from tens of thousands of rabid bats in a confined roost space within a cave. Aerosol infection may occur via direct attachment of the virus to olfactory nerve endings.
Rabies virus has been transmitted by transplantation of tissues and organs from infected humans.
Clinical Findings of Rabies in Animals
Clinical signs of rabies are suggestive but rarely definitive. Rabid animals of all species usually exhibit typical signs of CNS disturbance, with minor variations among species. The most reliable clinical signs, regardless of species, are acute behavioral changes and unexplained progressive paralysis.
Behavioral changes may include:
sudden anorexia
signs of apprehension or nervousness
irritability
hyperexcitability (including priapism)
Affected animals may seek solitude. Ataxia, altered phonation, and changes in temperament are apparent. Uncharacteristic aggressiveness may develop—a normally docile animal may suddenly become vicious. Commonly, rabid wild animals may lose their fear of humans, and normally nocturnal species may be observed wandering about during the daytime.
The clinical course of rabies may be divided into three general phases—prodromal, acute excitative, and paralytic (end stage). However, this division is of limited practical value because of the variability of clinical signs and the irregular lengths of the phases.
Pearls & Pitfalls
|
During the prodromal period, which lasts ~1–3 days, animals show only vague nonspecific signs, which intensify quickly. The disease is fatal once clinical signs appear.
The disease progresses swiftly after the onset of paralysis, and death is virtually certain a few days thereafter. Some animals die rapidly without marked clinical signs.
Furious Form
In the furious form of rabies, aggression (the acute neural excitative phase) is pronounced in animals. This is what is meant by “mad-dog syndrome,” although it may be found in all species. There is rarely evidence of paralysis during this stage.
In this phase of rabies, the animal becomes irritable and, with the slightest provocation, may viciously and aggressively use its teeth, claws, horns, or hooves. The posture and expression is one of alertness and anxiety, with pupils dilated. Noise may invite attack. Such animals lose caution and their fear of humans and other animals.
Carnivores with the furious form of rabies frequently roam extensively, attacking other animals, including humans, and any moving object. They commonly swallow foreign objects (eg, feces, straw, sticks, and stones).
Rabid dogs may chew the wire and frame of their cages, breaking their teeth, and will follow a hand moved in front of the cage, attempting to bite. Young pups can seek human companionship and are overly playful, but bite even when petted, usually becoming vicious in a few hours. Rabid skunks may seek out and attack litters of puppies or kittens. Rabid domestic cats and bobcats can attack suddenly, biting and scratching viciously.
As the disease progresses, muscular incoordination and seizures are common. Death results from progressive paralysis.
Paralytic Form
The paralytic form of rabies is manifested by ataxia and paralysis of the throat and masseter muscles, often with profuse salivation and the inability to swallow. Dropping of the lower jaw is common in dogs.
Owners frequently examine the mouth of dogs and production animals searching for a foreign body or administer medication with their bare hands, thereby exposing themselves to rabies virus. These animals may not be vicious and rarely attempt to bite.
The paralysis progresses rapidly to all parts of the body, and coma and death follow in a few hours.
Species Variations
Cattle with furious rabies can be dangerous, attacking and pursuing humans and other animals. Lactation ceases abruptly in dairy cattle. The usual placid expression is replaced by one of alertness. The eyes and ears follow sounds and movement intently. A common clinical sign is a characteristic abnormal bellowing, which may continue intermittently until shortly before death.
Horses and other equine species frequently show evidence of distress and extreme agitation. These clinical signs, especially when accompanied by rolling, may be misinterpreted as evidence of colic.
As in other species, horses may bite or strike viciously and, because of their size and strength, become unmanageable in a few hours. People have been killed outright by such animals. These animals frequently have self-inflicted wounds.
Rabid foxes and coyotes often invade yards or even enter houses, attacking dogs and humans. In this state, sometimes an animal will attack a porcupine; finding a fox or another animal with porcupine quills is otherwise considered abnormal and can, in many cases, raise the index of suspicion for rabies.
Rabid raccoons, foxes, and skunks typically show no fear of humans and are ataxic, frequently aggressive, and active during the day, despite their often crepuscular nature. In urban and suburban areas especially, they may attack domestic pets.
In general, rabies should be suspected in wildlife acting abnormally. The same is true of bats that can be observed flying in the daytime; resting on the ground, paralyzed and unable to fly; attacking humans or other animals; or fighting.
Rodents and lagomorphs rarely constitute a risk of exposure to rabies virus. However, each incident should be evaluated individually. Reports of laboratory-confirmed rabies in woodchucks and beavers are not uncommon in association with the raccoon rabies virus variant epizootic in the eastern US.
Diagnosis of Rabies in Animals
Immunofluorescence microscopy on fresh brain tissue
Molecular testing
Clinical examination findings may be suggestive of an apparent encephalitis but may be similar to a number of other diseases. In the early stages, rabies can easily be confused with other diseases or with individual aggressive tendencies. Furthermore, rabies may be overlooked as a differential diagnosis, especially in areas where the disease is uncommon. Rabies should always be considered as a differential diagnosis for clinical signs related to the CNS.
Diagnosis based on clinical signs alone should not be relied on when making public health decisions. When rabies is suspected and definitive diagnosis is required, laboratory confirmation is indicated. Rabies virus diagnosis should only be made by a qualified laboratory, designated by the local or state health department in accordance with established standardized national protocols for such viral testing.
No definitive antemortem test is available for rabies diagnosis. Typically, the suspect animal is euthanized and the head removed for laboratory shipment. The euthanasia method should ensure that the brain is not damaged and the brainstem is included.
Pearls & Pitfalls
|
At the laboratory, the brain (including the brainstem) is removed as the preferred organ for testing. Immunofluorescence microscopy on fresh brain tissue, which allows direct visual observation of a specific antigen-antibody reaction, is the current test of choice. When properly used, it can establish a highly specific diagnosis within a few hours.
Brain tissues examined must include the medulla oblongata and cerebellum (and should be preserved by refrigeration with wet ice or cold packs). The tissues should not be placed in fixative.
Virus isolation by tissue culture techniques using mouse neuroblastoma cells may be used for confirmation of indeterminate fluorescent antibody results; however, it is no longer in common use in the US.
Molecular testing, including real-time PCR assay, is becoming standard in modern diagnostic laboratories. The WHO recommends several diagnostic procedures for antigen detection.
Veterinarians who encounter a suspected case of rabies should follow their national and local guidelines for disease reporting.
Prevention and Control of Rabies in Animals
Rabies vaccination and registration of cats and dogs
Promotion of responsible animal ownership
Management of stray populations
Oral vaccination of wildlife reservoirs
Education to avoid exposure to suspect animals
Integrated veterinary management of local animal populations, by mass vaccination of dogs and community promotion of responsible pet ownership, is the most cost-effective, humane, longterm solution to eliminating regional rabies virus variants in a One Health context.
Domestic Animal Management
Comprehensive guidelines for control in dogs have been prepared internationally by the WHO and in the US by the National Association of State Public Health Veterinarians (NASPHV). The guidelines include:
Notification of suspected cases and euthanasia of dogs with clinical signs and dogs bitten by a suspected rabid animal
Decrease of contact rates between susceptible dogs by leash laws, dog movement control, and quarantine
Mass immunization of dogs by campaigns and by continuing vaccination of young dogs
Stray dog control and euthanasia of unvaccinated dogs with low levels of dependency on, or restriction by, people
Dog registration
The Compendium of Animal Rabies Control, compiled and updated regularly by the NASPHV, summarizes the most current recommendations for the US and lists all USDA-licensed animal rabies vaccines marketed in the US. Many effective vaccines, such as modified live virus, recombinant, and inactivated types, are available for use throughout the world; in the US, no modified live rabies virus vaccines are currently marketed (for any species).
Recommended vaccination frequency is typically every 3 years (unless otherwise indicated), after an initial series of two vaccines 1 year apart. Several vaccines are also available for use in cats, and a few for use in ferrets, horses, cattle, and sheep. Because of the increasing importance of rabies in cats, vaccination of cats is critical.
No parenteral vaccine is licensed for wildlife; however, use in captive or free-ranging species has occurred on a case-by-case basis for prophylaxis in zoos or to augment control in the field, respectively. Protective immunity and efficacy from the commercially available vaccines for domestic species have not been definitively demonstrated in all wildlife species.
Oral Vaccination of Wildlife
Historically, the control of rabies in wildlife populations relied on population reduction to decrease the contact rate between susceptible animals; however, this proved difficult and often not publicly acceptable, ecologically sound, economically warranted, or programmatically effective.
In Europe and Canada, administration of oral vaccines distributed in baits to control rabies in foxes has been widespread and effective. The disease in foxes has been eliminated from most of western Europe and curtailed substantially in Ontario.
Use of a vaccinia-rabies glycoprotein recombinant virus vaccine in the US has successfully eliminated coyote and gray fox rabies virus variants in southern and west-central Texas, respectively, and has limited the western expansion of raccoon rabies virus variant from the eastern US. Another product, a human adenovirus-rabies recombinant vaccine, has also been used successfully for the oral vaccination of wildlife within North America.
Licenses limit use of these vaccines to state or federal rabies programs; they are not available to private veterinarians or for individual animal use. Together with other biologics, such oral vaccines may also be used to assist in the control of the canine rabies virus variant in resource-limited countries.
Disinfection
As an enveloped virus, rabies virus is inactivated by various disinfectants (eg, formalin, phenol, alcohol, halogens, mercurials, mineral acids). The virus is extremely labile when exposed to heat or ultraviolet light.
Management of Suspected Rabies Cases—Exposure of Pets
Where carnivore or bat rabies virus variants are enzootic, any animal bitten or otherwise exposed by a wild, carnivorous mammal (or a bat) not available for testing should be regarded as having been exposed to rabies virus.
The NASPHV recommends that any unvaccinated dog, cat, or ferret exposed to rabies be euthanized immediately. If the owner is unwilling to do this, the animal should be placed in strict isolation (ie, no human or animal contact) for 4–6 months and vaccinated against rabies as soon as possible upon entry into quarantine. If an exposed domestic animal is currently vaccinated, it should receive medical assessment and wound care, be revaccinated immediately, and be closely observed for 45 days.
Zoonotic Risk of Rabies
Rabies has the highest case fatality of any infectious disease. When a person is exposed to an animal suspected of having rabies, the risk of rabies virus transmission should be evaluated carefully. Risk assessment should include:
consideration of the species of animal involved
prevalence of rabies in the area
whether exposure sufficient to transmit rabies virus occurred
current status of the animal
animal's availability for diagnostic testing
Wild carnivores and bats present a considerable risk where the disease is found, regardless of whether abnormal behavior has been observed. Insectivorous bats, though small, can inflict wounds with their teeth and should never be caught or handled with bare hands. Bat bites may be ignored or go unnoticed, so direct contact with bats could be considered a risk of virus exposure.
Any wild carnivore or bat suspected of exposing a person to rabies should be considered rabid unless proved otherwise by laboratory diagnosis; ideally, this includes bats in direct contact with people, such as those found in rooms with sleeping or otherwise unaware persons. Wildlife, including wolf hybrids, should never be kept as pets; if one of those animals exposes a person or domestic animal, the wild animal should be managed like free-ranging wildlife.
Any healthy domestic dog, cat, or ferret, whether vaccinated against rabies or not, that exposes (bites or deposits saliva in a fresh wound or on a mucous membrane) a person should be confined for 10 days; if the animal develops any clinical signs of rabies during that period, it should be euthanized and its brain promptly submitted for rabies diagnosis (taking care not to damage the brain and to include the brainstem).
If the dog, cat, or ferret responsible for the exposure is stray or unwanted, it may be euthanized as soon as possible and submitted for rabies diagnosis. Since the advent of testing by immunofluorescence microscopy, there is no value in holding such animals to “let the disease progress” as an aid to diagnosis.
Internationally, the WHO recommends several types of cell-culture vaccines for human groups at risk. In the US, CDC guidelines for prevention of rabies in humans follow recommendations prepared by the Advisory Council on Immunization Practices.
Preexposure immunization is strongly recommended for people in high-risk groups, such as veterinary staff, animal control officers, rabies and diagnostic laboratory workers, and, under certain circumstances, some travelers to areas in which the canine rabies virus variant is enzootic.
Preexposure vaccine is administered with a primary series on days 0 and 7, with the need for follow-up serologic testing or booster doses dependent upon the risk of viral exposure.2 However, preexposure prophylaxis alone cannot be relied on in the event of subsequent rabies virus exposure and must be supplemented by a limited postexposure regimen (two doses of vaccine, IM, on days 0 and 3).
For healthy, unvaccinated patients bitten by a rabid animal, postexposure prophylaxis consists of wound care, local infiltration of rabies immune globulin, and vaccine administration on days 0, 3, 7, and 14. When provided in a timely and appropriate manner, modern postexposure prophylaxis virtually assures human survival.
Key Points
Rabies is an acute, progressive, incurable viral encephalitis. This zoonosis has the highest case fatality of any infectious disease.
All mammals are believed susceptible to rabies virus and other lyssaviruses. Dog vaccination is the single most useful and cost-effective measure for modern rabies prevention and control.
All persons at occupational risk of rabies virus exposure, including veterinarians, should receive preexposure vaccination.
Rabies in humans can be prevented after exposure by proper wound care, infiltration of all bite sites with rabies immune globulin (in the unvaccinated individual), and the administration of several doses of rabies vaccine.
References
Subfamily: Alpharhabdovirinae, Genus: Lyssavirus. Virus Taxonomy: The ICTV Report on Virus Classification and Taxon Nomenclature; 2022 [database online]. International Committee on Taxonomy of Viruses. Accessed June 27, 2023. https://ictv.global/report/chapter/rhabdoviridae/rhabdoviridae/lyssavirus
Manning SE, Rupprecht CE, Fishbein D, et al. Human rabies prevention—United States, 2008: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2008;57(RR-3):1-28.
Rao AK, Briggs D, Moore SM, et al.Use of a modified preexposure prophylaxis vaccination schedule to prevent human rabies: recommendations of the Advisory Committee on Immunization Practices—United States, 2022. MMWR Morb Mortal Wkly Rep 2022;71:619–627. doi:10.15585/mmwr.mm7118a2
For More Information
Rabies. Centers for Disease Control and Prevention. Updated December 8, 2022.
National rabies management program. USDA Animal and Plant Health Inspection Service. Updated June 1, 2023.
Listed disease: rabies. World Organisation for Animal Health (WOAH).
Rabies. World Health Organization (WHO). Updated January 19, 2023.
National Association of State Public Health Veterinarians (NASPHV)
Ellis R, Ellis C. Dog and cat bites. American Academy of Family Practitioners (AAFP). August 15, 2014.
Also see pet health content regarding rabies in dogs, rabies in cats, and rabies in horses.




