

A follicular cyst is a thin-walled, fluid-filled structure that is larger than a normal follicle. It fails to ovulate due to hormonal abnormalities in some post-partum cows, resulting in a stalled reproductive cycle.
Follicular cystic ovary disease may be defined by several observations. Essentially all signs relate to disruption of the normal endocrine events of the estrous cycle that results from this failure of ovulatory events. Key features of follicular cystic ovary disease include the presence of a thin-walled, fluid-filled structure > 25 mm in diameter and present for > 10 days in the absence of a corpus luteum on ultrasonographic imaging of the ovary. Alongside occasional behavioral signs of nymphomania, such as short interestrus intervals and excessive heat behavior, are endocrine changes that include a suboptimal luteinizing hormone surge and persistently elevated estradiol concentrations.
Etiology and Pathogenesis of Follicular Cystic Ovary Disease in Cows
Cystic ovary disease or syndrome is commonly considered to be associated with negative energy balance and stress factors in high-milk-production dairy cows. A genetic predisposition to partition glucose to the udder to prioritize lactose synthesis and milk production is characterized by insulin resistance in Holstein cattle; increasingly, genomics offers insight to future control.
The incidence of cystic ovary disease increases with age. Most cases occur within 3–8 weeks of parturition, at the first attempted postpartum ovulation, coinciding with peak daily milk production and rapidly decreasing body condition. The reported herd incidence is between 6% and 30% per lactation; the incidence may be higher in problem herds.(1)

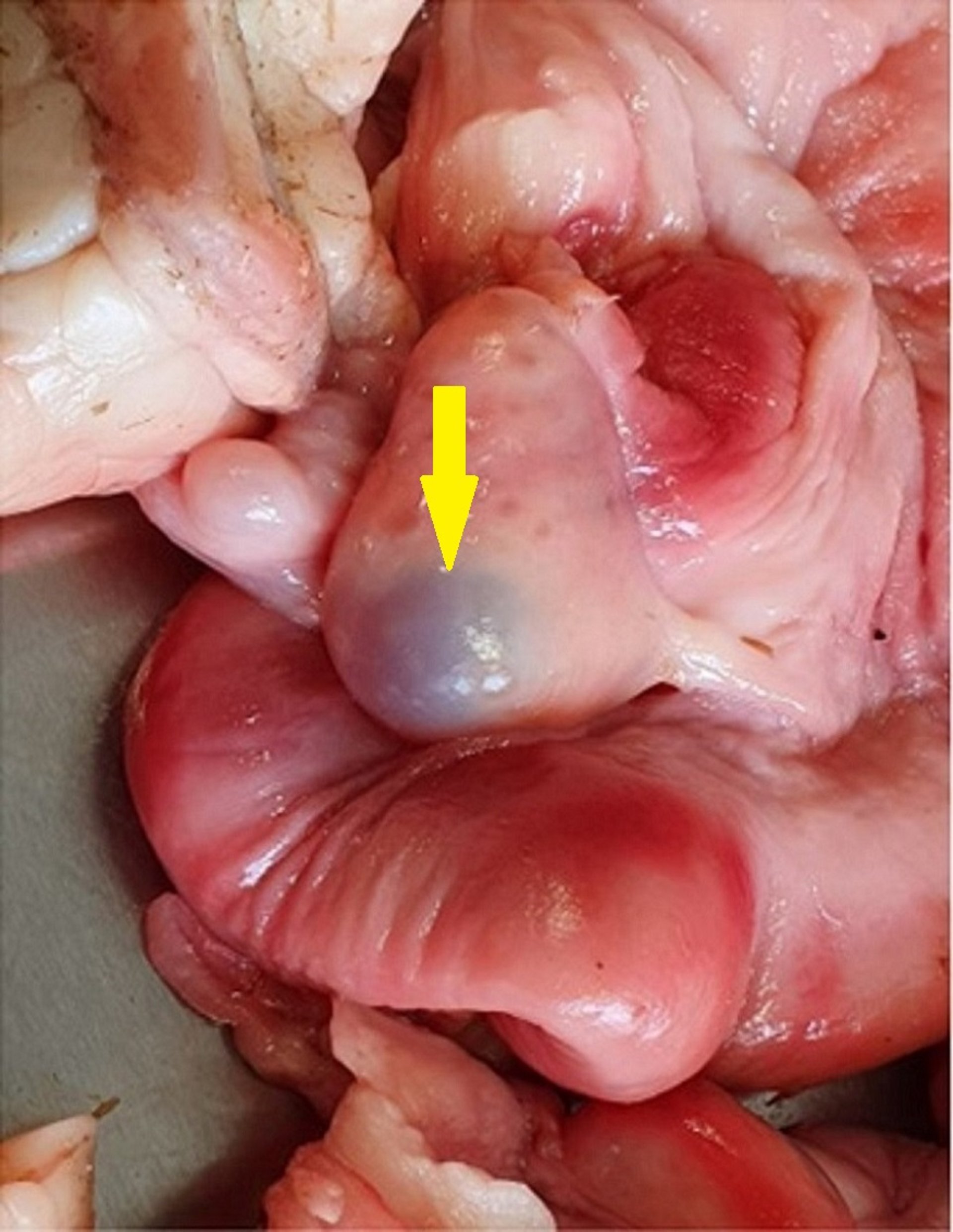
Courtesy of Dr. Jonathan Statham.

Courtesy of Dr. Jonathan Statham.
During normal proestrus, regression of the corpus luteum coincides with development of a selected dominant follicle, and the growth of any additional follicles is inhibited. In animals that develop cystic ovary disease, ovulation fails to occur and the dominant follicle continues to enlarge.
An important component of the etiology of cystic ovary disease is the failure of positive feedback of follicular estrogen on the hypothalamus via estrogen receptor alpha to release sufficient gonadotropin-releasing hormone (Gn-RH) during estrus to trigger a luteinizing hormone surge. Metabolic compromise contributes to this failure through decreased Gn-RH activity and hence absence of the spike in luteinizing hormone. The end result is a failure of ovulation at the time of estrus. Moreover, other follicles may grow and form multiple cysts either bilaterally or unilaterally.
Grossly, follicular cysts resemble enlarged follicles, generally defined as varying in diameter from 25 to 60 mm. The size and form of an affected ovary depends on the number and size of cysts present. The cystic ovary is capable, at least initially, of steroidogenesis, and its products vary from estrogens to progesterone to androgens.
The actions of the various hormones produced or the absence of the stabilizing action of a large amount of progesterone from the normal corpus luteum during ∼75% of the estrous cycle (or both) is responsible for the changes observed in the genital tract, body conformation, and general behavior. Importantly, the absence of progesterone inhibits the normal upregulation of luteinizing hormone receptors required for delivering the luteinizing hormone surge that is necessary for achieving ovulation, so the reproductive cycle stalls.
Clinical Findings of Follicular Cystic Ovary Disease in Cows
Behavioral aberrations range from frequent, intermittent estrus to bull-like behavior, including mounting, pawing the ground, and bellowing. This behavior may be accompanied by masculinization of the head and neck. Relaxation of the vulva, perineum, and the large pelvic ligaments, which causes the tail head to be elevated, can occur in chronic cases. Some affected cows show these signs, but others may be sexually quiescent; anestrous or subestrous cows are common.
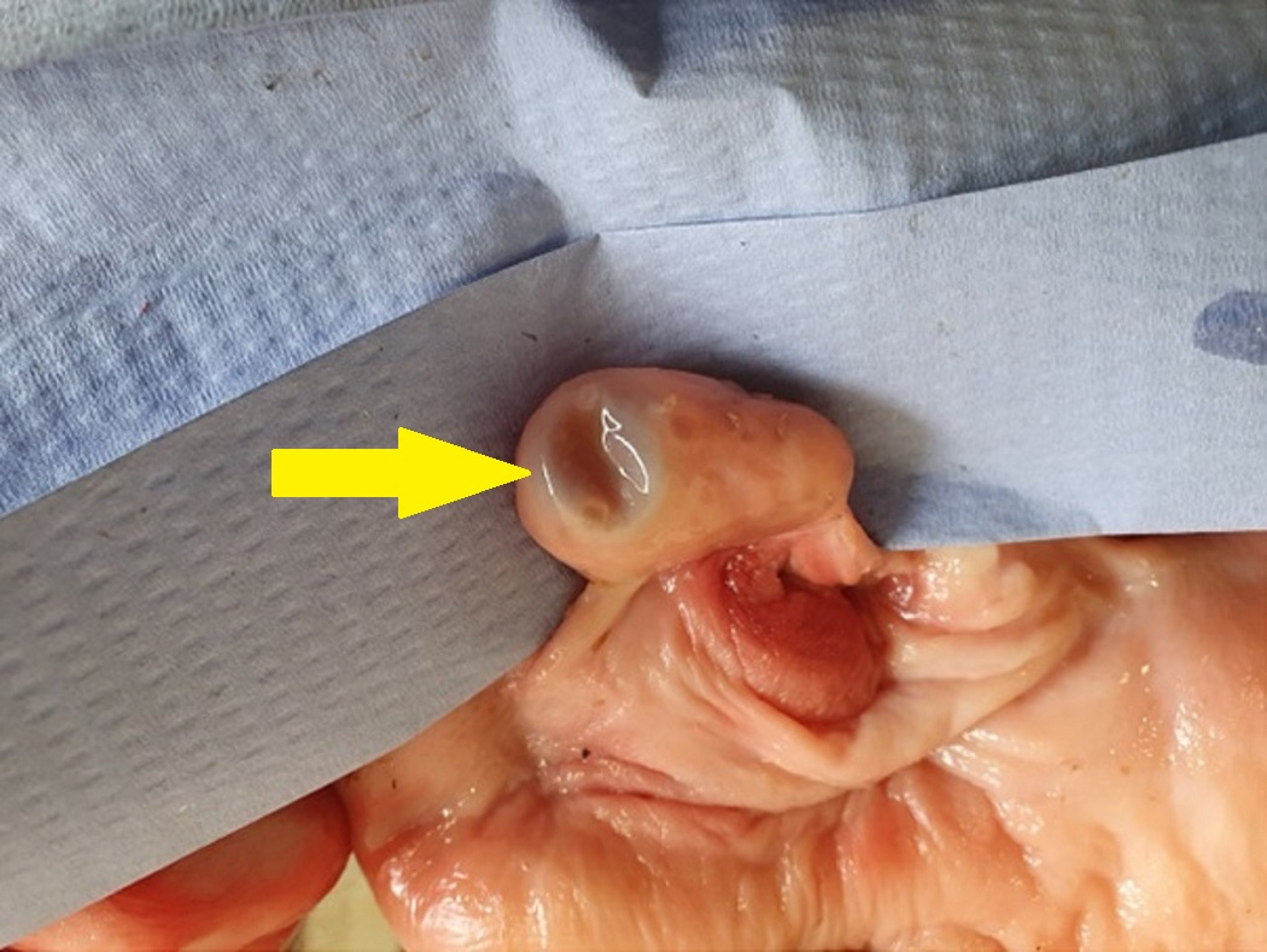
The affected ovaries generally are enlarged and rounded; however, their size varies by the number and size of the cysts. Their surface is smooth, elevated, and blisterlike. Cysts are frequently multiple and may be as large as 40–60 mm in diameter.
Under the influence of hormones produced by the cystic ovary or a lack of hormones (especially progesterone) normally present during estrous cycles, the uterus undergoes palpable changes, which in turn vary with the duration of the cystic condition. During the first week, the uterine wall is thickened and edematous as an extension of the preceding estrus. Toward the end of the first week, the uterine wall develops a spongelike consistency. In chronic cases, atony and atrophy of the uterine wall are common. Occasionally, the uterine horns become markedly shortened.
Some amount of mucoid to mucopurulent vaginal discharge is common. Hydrometra, a condition in which the uterus has extremely thin walls and is filled with fluid, occurs occasionally.
Diagnosis of Follicular Cystic Ovary Disease in Cows
Palpation of the uterus may be helpful to differentiate a follicular cyst from a dominant preovulatory follicle; the estrous cow has a coiled, extremely turgid uterus and a follicle. As noted earlier, cystic cows fail to ovulate a preovulatory follicle after undergoing corpus luteum regression and examination of the reproductive tract reveals a large follicle, absence of a corpus luteum, and absence of a turgid uterus.

Courtesy of Dr. Jonathan Statham.

Courtesy of Dr. Jonathan Statham.
Ultrasonography per rectum can be used to differentiate cysts from corpora lutea and may be helpful in diagnosing cyst type. For example, follicular cyst walls are < 3 mm in diameter, whereas luteal cyst walls are > 3 mm in diameter. Larger, multiple cysts are more easily identified by rectal palpation. History, conformation, and uterine changes, when present, provide supplemental diagnostic evidence. Cystic ovary disease usually lasts > 10 days.
Treatment of Follicular Cystic Ovary Disease in Cows
Cystic ovary disease may be refractory to initial treatment. Some cysts respond readily to treatment with a luteinizing-type hormone; human chorionic gonadotropin (hCG) has been commonly used.
Treatment with Gn-RH may be effective at a dose of 100 mcg and is less antigenic than treatment with hCG, which may become less effective on subsequent treatments because of the immune response. To hasten the onset of the first estrus after treatment, prostaglandin F2alpha products can be administered 7 days after hCG or Gn-RH.
Ovulation synchronization protocols, such as Ovsynch, combine Gn-RH and PGF2alpha to control follicular dynamics, luteolysis, and ovulation. They allow for fixed, timed artificial insemination of cattle without the need for estrus detection and have been successfully used to treat cows with cystic ovaries. Ovsynch consists of administering Gn-RH, then the prostaglandin 7 days later, then a second dose of Gn-RH 48 hours later, and finally timed artificial insemination 0–24 hours later.
Intravaginal progesterone devices may also be used to treat cystic ovary disease, providing critical progesterone for negative feedback, while upregulating luteinizing hormone receptors before device removal and luteinizing hormone surge. Breeding on the first estrus may minimize recurrence by establishing pregnancy as early as possible. However, recurrence of cystic ovary disease is a risk, especially if underlying metabolic risks mediated by IGF-1 and associated cytokines remain.
Manual rupture of cysts is one method of treating cystic ovary disease; however, the potential danger of traumatizing the ovary and causing hemorrhage with subsequent local adhesions should not be overlooked. Alternatively, ultrasonography can be used to guide fine-needle aspiration of the follicular fluid—eg, by means of the ovum pickup equipment that is used in ovum pickup/in vitro production procedures. Serial aspirations may be required but may provide benefit by removing physiologically active hormones.
Prognosis of Follicular Cystic Ovary Disease in Cows
After treatment with a luteinizing-type hormone, a normal, fertile estrus can be expected in 15–30 days. With Gn-RH treatment, 25% of cases required a second treatment, and 5% required a third. One-third of the cases treated for the third time failed to respond.(2,3) Spontaneous recovery is possible and is most common in cases arising during the first 50 days after calving.
References
BorŞ SI, BorŞ A. Ovarian cysts, an anovulatory condition in dairy cattle. J Vet Med Sci. 2020;82(10):1515–1522. doi: 10.1292/jvms.20-0381. Epub 2020 Aug 18. PMID: 32814749; PMCID: PMC7653308.
Tebble JE, O'Donnell MJ, Dobson H. Ultrasound diagnosis and treatment outcome of cystic ovaries in cattle. Vet Rec. 2001;148(13):411–413. doi: 10.1136/vr.148.13.411. PMID: 11327649.
Cantley TC, Garverick HA, Bierschwal CJ, Martin CE, Youngquist RS. Hormonal responses of dairy cows with ovarian cysts to GnRH. J Anim Sci. 1975;41(6):1666–1673. doi: 10.2527/jas1975.4161666x. PMID: 1107286.





