

Equine herpesviruses are ubiquitous worldwide, with EHV-1 and EHV-4 having the greatest clinical importance in causing respiratory disease in horses. Fever, nasal discharge, malaise, pharyngitis, and cough are key symptoms. EHV-1 may also cause late term abortions or neurologic disease (equine herpesvirus myeloencephalopathy, EHM). Diagnosis is primarily via PCR array on nasal swab or whole blood. Treatment is largely supportive, although use of antiviral medications has been described for treatment of horses with EHM.
Etiology and Epidemiology of Equine Herpesvirus Infection
Equine herpesvirus 1 (EHV-1) and equine herpesvirus 4 (EHV-4) are alpha-herpesviruses and comprise two antigenically distinct groups of viruses previously referred to as subtypes 1 and 2 of EHV-1. EHV-4 infection and disease is limited to horses, and EHV-1 causes disease in most equids as well as other species. Both viruses are ubiquitous in horse populations worldwide and produce an acute febrile respiratory disease upon primary infection, characterized by rhinopharyngitis and tracheobronchitis.
The natural reservoir of both EHV-1 and EHV-4 is the horse and latency is a hallmark of infection. Transmission is via nasal secretions (direct contact, fomite, aerosolized). Viral replication occurs in the mucosa and lymph nodes of the upper respiratory tract and is followed by cell-associated viremia. Once infected, viral latency occurs (eg, in the trigeminal ganglia or peripheral blood lymphocytes) and a carrier state is established in young horses. Stress precipitates viral reactivation, shedding, and new infections, thus perpetuating the virus in the equine population. Transmission occurs by direct or indirect contact with infectious nasal secretions, aborted fetuses, placentas, or placental fluids. In individual horses, the outcome of exposure is determined by viral strain, immune status, pregnancy status, and possibly age.
Outbreaks of respiratory disease occur annually among groups of foals or younger performance horses in areas with concentrated horse populations. Most of these outbreaks in weanlings are caused by strains of EHV-4. Outbreaks may also occur sporadically affecting horses of any age and vary according to seasonal and geographic distribution with disease manifestation determined by immune status and horse population. In addition to respiratory disease, EHV-1 outbreaks are associated with other diseases including late gestation abortion (abortion storms), equine herpesvirus myeloencephalopathy (EHM), and neonatal foal death. Mares may abort several weeks to months after clinical or subclinical infection with EHV-1. The neurologic form of EHV-1 (EHM) has demonstrated increasing morbidity and mortality in documented outbreaks since 2000. The USDA-APHIS designated EHV-1 as an emerging disease and it is reportable in many states within the US. Infection with EHV-4 can cause respiratory disease outbreaks but only rarely results in abortion in pregnant mares.
Clinical Findings of Equine Herpesvirus Infection
Respiratory disease
Abortion
Neurologic disease
The incubation period of EHV is 2–10 days. Susceptible horses develop fever of 102°–107°F (38.9°–41.7°C), neutropenia and lymphopenia, serous nasal discharge, malaise, pharyngitis, cough, inappetence, and/or submandibular or retropharyngeal lymphadenopathy. Horses infected with EHV-1 strains often develop a biphasic fever (1–2 days and 4–8 days), with lymphocyte-associated viremia coinciding with the second temperature peak. Secondary bacterial infections are common and manifest with mucopurulent nasal exudate and pulmonary disease. The infection is mild or inapparent in horses with prior immune exposure to the virus, via previous infection or vaccination.
Mares that abort after EHV-1 infection seldom display premonitory signs. Abortions occur 2–12 weeks after infection, usually between months 7 and 11 of gestation. Aborted fetuses are fresh or minimally autolyzed, and the placenta is expelled shortly after abortion. There is no evidence of damage to the mare’s reproductive tract, and subsequent conception is unimpaired. Mares exposed late in gestation may not abort but give birth to live foals with fulminating viral pneumonitis. Such foals are susceptible to secondary bacterial infections and usually die within hours or days.
Outbreaks with specific strains of EHV-1 infection result in neurologic disease due to EHM. Clinical signs vary from mild incoordination and caudal paresis to severe caudal paralysis with recumbency, loss of bladder and tail function, and loss of skin sensation in the perineal and inguinal areas. In exceptional cases, the paralysis may progress to quadriplegia and death. Prognosis depends on severity of signs and the period of recumbency.
Lesions
The pathogenic mechanisms of EHV-1 and EHV-4 differ: EHV-4 infection is restricted to the respiratory tract epithelium and associated lymph nodes, whereas EHV-1 strains develop lymphocyte-associated viremia and have a predilection for vascular endothelium, especially within the nasal mucosa, lungs, placenta, adrenal, thyroid, and CNS. The neuropathic strain of EHV-1 produces a viremic load 10- to 100-fold higher than that of non-neuropathic strains.
Gross lesions of viral rhinopneumonitis are hyperemia and ulceration of the respiratory epithelium, and multiple, tiny, plum-colored foci in the lungs. Histologically, there is evidence of inflammation, necrosis, and intranuclear inclusions in the respiratory epithelium and germinal centers of the associated lymph nodes. Lung lesions are characterized by neutrophilic infiltration of the terminal bronchioles, peribronchiolar and perivascular mononuclear cell infiltration, and serofibrinous exudate in the alveoli.
Typical lesions in EHV-1 aborted fetuses include interlobular lung edema and pleural fluid; multifocal areas of hepatic necrosis; petechiation of the myocardium, adrenal gland, and spleen; and thymic necrosis. Intranuclear inclusions are found in lung, liver, adrenal, and lymphoreticular tissues.
Horses with EHV-1–associated neurologic disease may have no gross lesions or only minimal evidence of hemorrhage in the meninges, brain, and spinal cord parenchyma. Histologically, lesions are discrete and comprised of vasculitis with endothelial cell damage and perivascular cuffing, thrombus formation and hemorrhage, and in advanced cases, areas of malacia. Lesions may occur at any level of the brain or spinal cord.
Diagnosis of Equine Herpesvirus Infection
PCR assay
Virus isolation
Equine viral rhinopneumonitis is difficult to clinically differentiate from equine influenza, equine viral arteritis, or other equine respiratory infections solely on the basis of clinical signs. Definitive diagnosis is most frequently determined by PCR assay from samples obtained via nasopharyngeal swab and citrated blood sample (buffy coat) early in the course of the infection; viral isolation is also possible but more time-consuming. Nasal swab PCR assay provides a more accurate assessment of whether an animal is shedding virus, but because horses can intermittently shed, it may result in false negative results.
In cases of suspected EHV-1 abortion, definitive diagnosis is based on PCR assay, virus isolation, and characteristic gross and microscopic lesions in the aborted fetus. Lung, liver, adrenal, and lymphoreticular tissues are productive sources of virus. Serologic testing of mares after abortion has little diagnostic value.
Diagnosis of neuropathic EHV-1 is determined by real-time PCR assay on samples obtained from nasal secretions, CSF, or neural tissue. A presumptive diagnosis can be based on clinical signs and CSF analysis (xanthochromia, albuminocytologic dissociation). Postmortem examination reveals characteristic perivascular cuffing and hemorrhage in the CNS.
Treatment of Equine Herpesvirus Infection
Supportive care
Antivirals
There is no specific treatment for EHV infection. Rest, supportive care, and NSAIDs are indicated to minimize secondary complications and to treat fever > 102.5°F (39°C). Antimicrobial treatment is only instituted upon suspicion of secondary bacterial infection evidenced by purulent nasal discharge or pulmonary disease. Most foals infected prenatally with EHV-1 die shortly after birth despite intensive nursing and antimicrobial medication. If horses with neuropathic EHV-1 remain ambulatory or are recumbent for only 2–3 days, the prognosis is usually favorable.
Acyclovir administration (10 mg/kg, PO, 5 times per day) has been described for use in horses with EHM, but has very low bioavailability. Valacyclovir (30 mg/kg, PO, q 6–8 h), a prodrug of acyclovir, has shown promise in the treatment of experimentally affected horses and in prophylaxis during EHV-1 outbreaks, although more information is needed regarding its efficacy in natural infection. Recently, the use of heparin products has been described for the treatment of EHM. Intensive nursing care is necessary to avoid pulmonary congestion, pneumonia, ruptured bladder, or bowel atony in patients with EHM. Recovery may be complete; however, a small percentage of cases have neurologic sequelae.
Control of Equine Herpesvirus Infection
Natural immunity
Management and biosecurity
Vaccination
Immunity after natural infection with either EHV-1 or EHV-4 involves a combination of humoral and cellular immunity. Whereas little cross-protection occurs between virus types after primary infection of immunologically naive foals, cross-protection does develop in horses after repeated infections with a particular virus type. Equine herpesviruses 1 (EHV-1) and 4 (EHV-4) are endemic in horse populations as a result of viral latency in most adult horses.(1) The infection remains dormant for most of the horse’s life, although stress or immunosuppression may result in recrudescence of disease and shedding of infectious virus. Immunity to reinfection of the respiratory tract may persist for up to 3 months; however, multiple infections result in a level of immunity that prevents clinical signs of respiratory disease. Diminished resistance in pregnant mares allows cell-associated viremia, which may result in transplacental infection of the fetus.
For prevention and control of EHV-4– and EHV-1–related diseases, management and biosecurity practices that decrease viral spread are recommended. In an outbreak, these include barrier protection, strict hygiene and disinfection, and isolation of in-contact and affected horses for 28 days after recovery of the last clinical case. Transmission is via airborne droplets or contact and virus may remain viable on common surfaces for approximately 48 hours under realistic environmental conditions. New horses (or those returning from other premises) should be isolated for 21 days before commingling with resident horses, especially pregnant mares. Management-related, stress-inducing circumstances should be avoided to prevent recrudescence of latent virus. Pregnant mares should be maintained in a group away from the weanlings, yearlings, and horses out of training.
Currently, a vaccine that offers comprehensive protection against EHV, particularly EHV-1-associated abortion and EHM, does not exist. Vaccination (EHV-4 and EHV-1) with currently available products should begin when foals are 4–6 months old. A second dose is administered 4–6 weeks later, and a third dose at 10–12 months of age. Booster vaccinations may be indicated as often as every 6 months through maturity (5 years of age). For nonpregnant adult horses, current vaccination guidelines recommend that horses that are < 5 years of age, on breeding farms or in contact with pregnant mares, housed at facilities with frequent movement on or off the premises, or that are performance/race horses in high-risk situations should be revaccinated at 6-month intervals or more frequently, depending on facility- or event-specific vaccination rules. A high-antigen load, inactivated EHV-1 vaccine is recommended to prevent EHV-1 abortion. Vaccine should be administered during months 3, 5, 7, and 9 of pregnancy. Mares are often vaccinated with inactivated EHV-1/EHV-4 at an interval 4–6 weeks before foaling. A modified-live EHV-1 vaccine is available to help prevent respiratory disease caused by EHV-1. United States Equestrian Federation (USEF) events currently require documentation of vaccination for EHV (and equine influenza virus) within 6 months of entering event grounds.
Infection by Other Equine Herpesviruses
Equine herpesvirus 2 (EHV-2), a gamma-herpesvirus, is ubiquitous in respiratory mucosa, conjunctiva, and WBCs of normal horses of all ages. Its pathogenic importance remains unclear. It has been suggested that EHV-2 is the cause of herpetic keratoconjunctivitis and pharyngitis in foals and it is has been implicated in the development of mild-moderate asthma in young, athletic horses. Equine herpesvirus 3 (EHV-3) is the cause of equine coital exanthema, a benign, progenital exanthematous disease. Respiratory disease associated with EHV-3 infection is not described.
Equine herpesvirus 5 (EHV-5), a gamma-herpesvirus, has been identified as a pathogen associated with equine multinodular pulmonary fibrosis (EMPF). The role of EHV-5 in EMPF is unclear (ie, whether precipitating, causative, or incidental). Clinical signs include weight loss, cough, fever (variable), and respiratory difficulty. EMPF is seen primarily in middle-aged horses, although it has been reported in young horses. Physical examination findings include tachycardia, tachypnea, increased respiratory effort (inspiratory), and poor body condition. Wheezes and crackles are often ausculted without a rebreathing procedure. In early cases, EMPF may be mistaken as severe asthma or bronchopneumonia. In addition to EMPF, EHV-5 has been associated with lymphoproliferative disease and lymphoma. One unusual case report describes a 21-year-old horse with profound pancytopenia and pulmonary fibrosis; EHV-5 was isolated from the bone marrow of this horse.

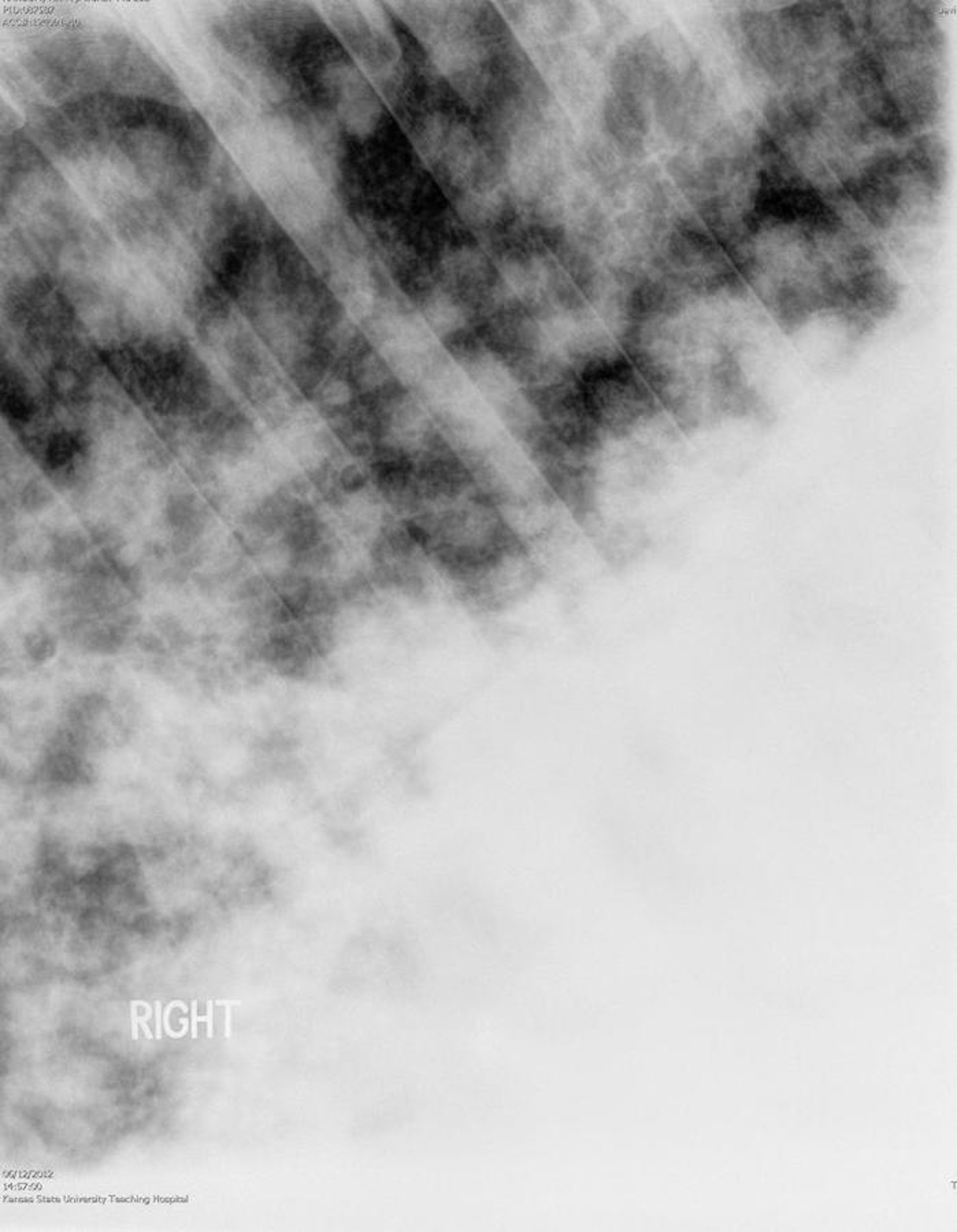
Courtesy of Dr. Bonnie R. Rush.
Diagnostic testing for EMPF includes routine blood work, thoracic radiographs, and virus-specific PCR array on pulmonary secretions (bronchoalveolar lavage) or percutaneous lung biopsy sample. CBC shows neutrophilic leukocytosis with or without hyperfibrinogenemia and anemia. Findings on thoracic radiographs range from a moderate interstitial pattern to a severe reticulonodular pattern. Thoracic ultrasound may reveal diffuse pleural roughening as well as discrete nodules in advanced disease. Differential diagnoses of radiographic images include fungal pneumonia and metastatic neoplasia, both of which are also relatively rare. The most common antemortem diagnostic test is virus-specific PCR array of bronchoalveolar lavage fluid. Percutaneous, ultrasound-guided lung biopsy can be performed to confirm the diagnosis and establish a prognosis. Histopathologic evaluation shows multifocal granulomas, type II pneumocyte hyperplasia, and intraluminal cellular accumulation. Advanced pulmonary fibrosis indicates a poor prognosis for survival.
The overall prognosis for survival in horses diagnosed with EMPF is ~50% and treatment is prolonged. Horses with EMPF have responded to treatment with antiviral treatment. Valacyclovir (30 mg/kg, PO, q 8 h) and/or acyclovir (10 mg/kg, IV in 1 L of isotonic crystalloid fluid as a constant-rate infusion over 1 hour, q 12 h × 2 days) appear promising, although sensitivity of the virus to these medications and efficacy in treatment of EMPF is unknown. Broad-spectrum antimicrobial treatment is also administered to combat secondary bacterial infection. Administration of corticosteroids is controversial, although they are commonly used. Corticosteroids (0.08-0.1 mg/kg, IV, every 24–48 hours) may improve disease outcome via reduction of pulmonary cytokines and inflammatory mediators; however, they may also cause immunosuppression, which may enhance viral replication and disease severity.
Key Points
EHV-1 and EHV-4 are major causes of viral respiratory disease in horses. EHV-1 also causes abortion and neurologic disease and is reportable in several states within the US.
Viral latency and a carrier state are associated with EHV infection; this allows the virus to be maintained within populations of horses.
Transmission is primarily via respiratory secretions; diagnosis is based on PCR array of a nasal swab in actively shedding horses and PCR array of whole blood in viremic horses.
Vaccination and appropriate biosecurity practices are essential in controlling outbreaks and preventing the spread of EHV.
EHV-5 is a potential causative agent for EMPF, while EHV-2 is of questionable importance as a cause of respiratory disease in horses.
References
Patel JR, Heldens J. Equine herpesviruses 1 (EHV-1) and 4 (EHV-4): epidemiology, disease and immunoprophylaxis: a brief review. Vet J. 2005;170:14-23.
For More Information
American Association of Equine Practitioners: General Infectious Disease Guidelines
AAEP: Equine herpesvirus disease-specific guidelines
Also see pet health content regarding equine herpesvirus infection.





