

Rhodococcus equi is a gram-positive, intracellular bacteria that causes chronic suppurative bronchopneumonia with abscessation in foals 1–5 months of age. Clinical signs are mild and nonspecific early in the course of disease but become more pronounced as pneumonia progresses and include cough, fever, lethargy, and increased respiratory effort. A definitive diagnosis depends on culture of R equi and identification via PCR array of the VapA gene from a transtracheal wash sample. Recommended treatment for foals with confirmed R equi pneumonia involves prolonged macrolide and rifampin antimicrobial treatment.
Rhodococcus equi is the most common and serious cause of pneumonia in foals 1–5 months old. Mortality and costs associated with prolonged treatment can be high. The economic burden is even greater on farms where the disease is endemic, because of substantial costs associated with surveillance programs for early detection and relatively expensive prophylactic strategies. Clinical disease is rare in horses > 8 months old. Epidemiologic data indicates that younger foals are more susceptible to infection compared to older foals and that pulmonary infection for most foals probably originates within the first 1–2 weeks of life.
Etiology and Pathogenesis of R equi Pneumonia in Foals
R equi is a gram-positive, facultative intracellular pathogen that is nearly ubiquitous in the soil of most horse farms. R equi isolates associated with disease contain a virulence plasmid with the VapA gene. The prevalence of clinical disease varies farm-to-farm from endemic to sporadic to unreported. Evidence suggests that the risk of infection is greater on large, high density breeding farms with increased movement of horses on and off the property. Inhalation of dust particles laden with virulent R equi is the major route of pneumonic infection; manure from pneumonic foals is a major source of virulent bacteria contaminating the environment. Foals with pulmonary infections swallow sputum laden with R equi, which readily replicates in their intestinal tract. R equi infection is slowly progressive, with acute to subacute clinical manifestations.
Once inhaled, R equi is taken up by alveolar macrophages via phagocytosis. The pathogenicity of R equi is linked to its ability to survive intracellularly, which hinges on failure of phagosome-lysosomal fusion in infected macrophages and failure of functional respiratory burst upon phagocytosis of R equi. Macrophages are eventually destroyed by uncontrolled intracellular replication of R equi. Development of clinical disease in foals is multifactorial; in addition to microbial virulence, antibody- and cell-mediated immunocompetency of the individual foal is important. Because R equi is an intracellular pathogen, cell-mediated immunity plays an important role in prevention of disease. Evidence indicates that young foals are deficient in cytotoxic T lymphocytes when compared to older foals and adult horses. It has been suggested that low gamma interferon (IFN-gamma) concentrations may be another risk factor for infection with R equi.
Clinical Findings and Lesions of R equi Pneumonia in Foals


R equi pulmonary disease
Clinical signs of disease are difficult to detect until pulmonary infection reaches a critical mass, resulting in decompensation of the foal. Pulmonary lesions are relatively consistent and include subacute to chronic suppurative bronchopneumonia, pulmonary abscessation, and suppurative lymphadenitis. Early clinical signs in most foals include lethargy, fever, occasional cough, and slight tachypnea that may be absent at rest. In foals with advanced pneumonia, fever, cough, tachypnea, and increased respiratory effort are more obvious; purulent nasal discharge is less common. Stress or handling can exacerbate clinical signs at any stage of disease. Thoracic auscultation reveals crackles and wheezes with asymmetric/regional distribution. Pulmonary regions with marked consolidation lack breath sounds and exhibit dull resonance on thoracic percussion. In foals with subclinical infections, small to moderate-sized abscesses (with a sum of all combined abscess diameters being < 10 cm) may resolve spontaneously.(1)
Nonpulmonary R equi

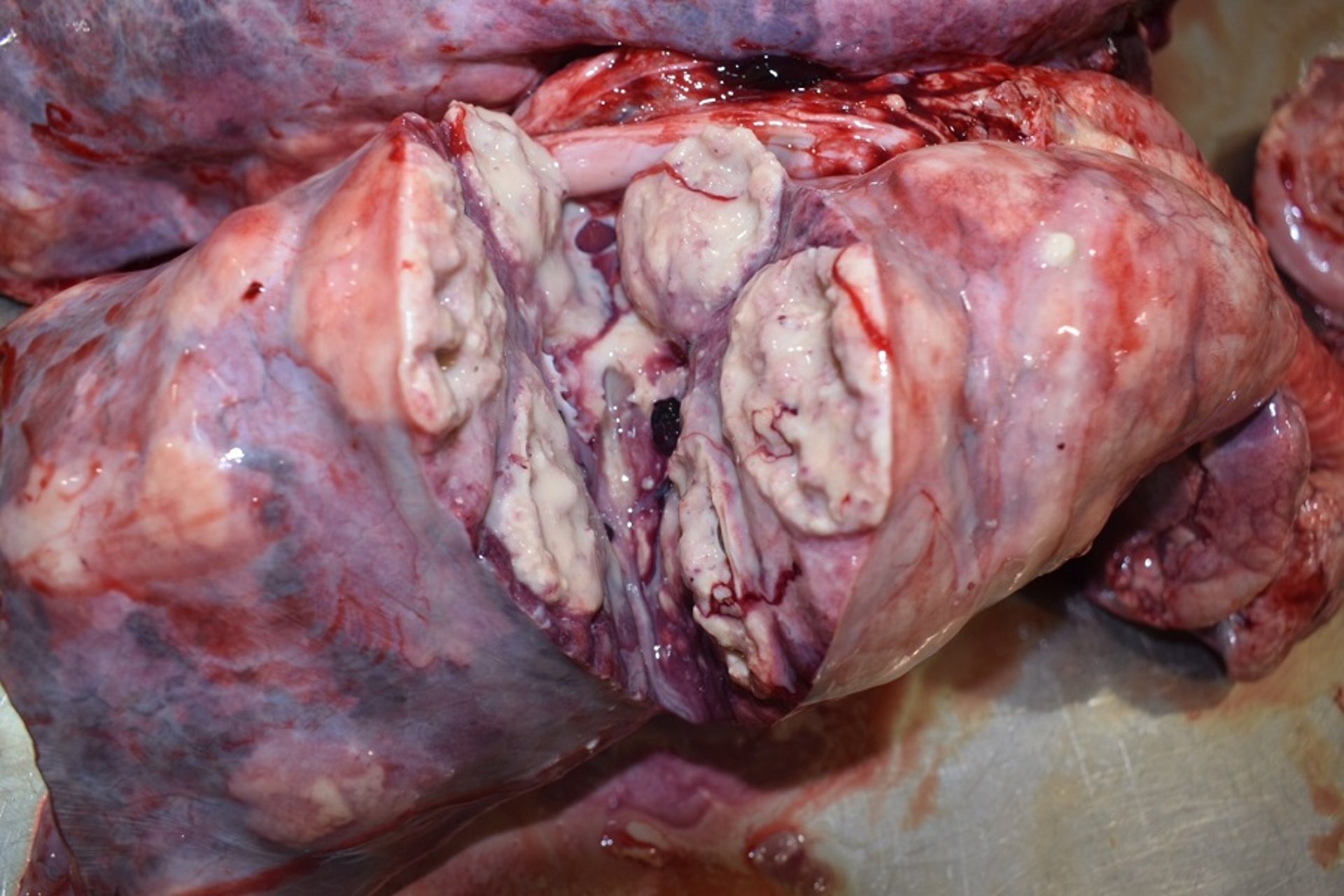
Courtesy of Dr. Kara Lascola.
Nonpulmonary clinical manifestations of R equi infection are reported as sequelae to or may be independent from pulmonary disease. Intestinal and mesenteric abscesses are the most common extrapulmonary sites of infection. Although intestinal lesions are identified at postmortem examination in close to 50% of foals with pneumonia, they do not always result in clinical signs of intestinal disease. Foals with abdominal involvement often present with fever, depression, anorexia, weight loss, colic, and diarrhea. Intestinal lesions are characterized by multifocal, ulcerative enterocolitis and typhlitis, with granulomatous or suppurative inflammation of the mesenteric and/or colonic lymph nodes. The prognosis for foals with abdominal forms of R equi is less favorable than for those with pulmonary disease.
Septic physitis and osteomyelitis are less common extrapulmonary sites of infection. Vertebral osteomyelitis may result in pathologic vertebral fracture and spinal cord compression and is a devastating manifestation of R equi osteomyelitis. Polysynovitis (eg, stifle and hock effusion) is often seen in affected foals at presentation and may represent an immune-mediated or septic process. Panophthalmitis, guttural pouch empyema, sinusitis, pericarditis, nephritis, nonseptic uveitis, and hepatic and renal abscessation with R equi have been less commonly reported.
Diagnosis of R equi Pneumonia in Foals
Laboratory evaluation
Imaging
Bacterial culture or PCR array amplification of the VapA gene in a tracheobronchial aspirate (TBA) from a foal with clinical, cytological, and radiographic signs of pneumonia is required for definitive diagnosis of R equi pneumonia. R equi is ubiquitous on some farms, and identification of R equi on TBA culture or PCR array and without supporting clinical or other diagnostic findings of pneumonia may represent an incidental finding. A combination of both TBA culture and VapA PCR may increase sensitivity of detecting R equi in foals with supportive clinical signs. Additionally, inclusion of TBA culture with VapA PCR allows for the detection of other bacterial pathogens in cases where there is a mixed bacterial pneumonia.
Cytologic evaluation of transtracheal wash samples reveals intracellular coccobacilli and can be used to guide appropriate antimicrobial treatment pending culture results. Routine laboratory evaluation of CBC and serum chemistry shows nonspecific abnormalities consistent with infection and inflammation. Hyperfibrinogenemia followed by neutrophilic leukocytosis are the most common abnormalities but cannot be used to determine prognosis in a foal. Serum amyloid A, another indicator of inflammation, correlates poorly with R equi disease severity. Serologic testing is not recommended for the diagnosis of R equi.
Thoracic radiography may reveal a perihilar alveolar pattern indicating consolidation, as well as discrete abscessation. The presence of nodular lung lesions and mediastinal lymphadenopathy in foals 1–5 months old is highly suggestive of R equi. Thoracic ultrasound can be used to evaluate both the thoracic and abdominal compartments. Ultrasound is best for identifying lesions of the peripheral lung and may miss abscesses that lie deep to aerated lung.
Treatment and Prognosis of Rhodococcus equi Pneumonia in Foals
Antimicrobials
Supportive care
The recommended treatment for foals with severe pneumonia is combination treatment with a macrolide antimicrobial (erythromycin, azithromycin, clarithromycin) and rifampin. These antimicrobials are bacteriostatic; however, their activity is synergistic and they are highly lipophilic allowing for penetration into abscess material and intracellular concentration in granulocytes and macrophages. Erythromycin was historically the macrolide of choice for treatment of R equi but clarithromycin and azithromycin are currently preferred over erythromycin because of their superior bioavailability. Of the three, clarithromycin has the most favorable MIC90 against R equi isolates obtained from pneumonic foals (90% isolates inhibited at 0.06, 0.5, and 1 mcg/mL for clarithromycin, erythromycin, and azithromycin respectively)(2) and is recommended in foals with severe pneumonia.
Antimicrobial Treatment for R equi in Foals
Drug | Dose, Route, Frequency | Usage Instructions |
|---|---|---|
Erythromycin (as estolate or base) | 25 mg/kg, PO, every 6–8 h | In combination with rifampin |
Erythromycin (as lactobionate) | 5 mg/kg, IV, every 6 h | In combination with rifampin |
Clarithromycin | 7.5 mg/kg, PO, every 12 h | In combination with rifampin |
Azithromycin | 10 mg/kg, PO, every 24 h for 5 days, then every 48 h 5 mg/kg, IV, every 24 h × 5 days, then every 48 h | In combination with rifampin |
Rifampin | 5 mg/kg, PO, every 12 h | In combination with a macrolide |
The duration of antimicrobial treatment for foals with severe pneumonia ranges from 2–12 weeks depending on disease severity and response to treatment. Parameters to guide discontinuation of medical treatment include improved clinical signs and resolution of pulmonary consolidation and abscessation on radiography or ultrasonography. Reported adverse reactions in foals treated with a macrolide-rifampin combination include self-limiting diarrhea, hyperthermia, and tachypnea. Life-threatening, antimicrobial-induced enterocolitis, due to Clostridium difficile, has been seen in the dams of nursing foals treated with all macrolide preparations.
Antimicrobial resistance of R equi isolates to macrolide-rifampin treatment is uncommon but has been reported. Based on reported in vitro susceptibility, alternatives for antimicrobial treatment include gentamicin, chloramphenicol, fluoroquinolones, minocycline, trimethoprim-sulfamethoxazole, vancomycin, imipenem, or linezolid. The decision to use an alternative antimicrobial for treatment of R equi should only be made when resistance to the macrolide-rifampin combination has been confirmed via laboratory susceptibility testing. Of these, gentamicin (intravenous or nebulized) may be the best choice because of its bactericidal action and reported ability to achieve concentrations > MIC90 for R equi at the site of infection.
Supportive treatment is important and includes provision of a clean, comfortable, well-ventilated environment, and good nutritional support and hydration. Judicious intravenous fluid treatment may be warranted and NSAIDs should be administered as needed to maintain rectal temperature < 103.5°F (39.7°C). Nasal insufflation with oxygen is necessary in foals with severe respiratory compromise. The use of saline nebulization and bronchodilator treatment may or may not be of clinical utility. Prophylactic antiulcer medication is indicated in foals stressed by respiratory difficulty, pain, and hospitalization. Antimicrobial treatment should be modified as needed to address confirmed mixed-bacterial infections or to address R equi septic arthritis or osteomyelitis.
The survival rate of R equi pneumonia is ~60%–90% with appropriate treatment, depending on disease severity. The case fatality rate without treatment (or with inappropriate antimicrobial treatment) in foals with clinical disease is ~80%. The prognosis for future performance is very good in foals with uncomplicated R equi pneumonia that respond to treatment.
Prevention of R equi Pneumonia in Foals
Several strategies have been proposed to decrease the incidence of R equi pneumonia on endemic farms: screening for early detection of clinical cases and enhanced passive immunity for neonatal foals are the most common of these. While useful on endemic farms, these methods are also labor intensive and expensive. Proposed screening strategies include serial monitoring by visual observation and physical examination, hematologic evaluation (WBC, fibrinogen concentration) and/or repeated thoracic ultrasound. Of these, serial ultrasonographic examination has been the most useful for detection of subclinical disease, with recommendations for antimicrobial treatment based on detection of pulmonary lesions ≥ 1 cm in diameter. A major concern with this strategy is that it may result in unnecessary antimicrobial administration to foals that would recover without treatment. This increases the risk for development of macrolide- and rifampin-resistant R equi strains.
A suitable vaccine is currently unavailable for prevention of R equi. Administration of hyperimmune plasma (HIP) might decrease the incidence and severity of R equi within the herd; however, it is not completely effective in preventing disease. A common protocol is administration of hyperimmune plasma (1 L, IV) within the first few days of life, followed by a second liter at ~25 days of age. Reduced detection of subclinical disease has also been reported in foals administered 2 L of HIP within 48 hours of birth. Foals with low IFN-gamma production in the first month of life appear more susceptible to development of clinical disease.
Key Points
R equi infection can cause severe suppurative bronchopneumonia in foals; however, on farms where R equi is endemic, many foals may only develop subclinical infection.
In a foal with clinical signs of respiratory disease and corresponding lesions identified on thoracic imaging, a definitive diagnosis of R equi pneumonia can be made with a positive culture or VapA gene identification in TBA sample.
The use of both culture and PCR may increase sensitivity in obtaining definitive diagnosis of R equi infection in foals with clinical signs of pneumonia and may also allow for identification of concurrent infection with other bacterial organisms.
Numerous extrapulmonary manifestations of infection are reported: gastrointestinal disease, septic physitis and osteomyelitis, polysynovitis, and uveitis are among the most common.
Combination treatment with a macrolide and rifampin is effective for R equi pneumonia; prophylactic antimicrobial treatment in “at-risk” foals is discouraged.
References
Venner M, Rodiger A, Laemmer M, et al. Failure of antimicrobial therapy to accelerate spontaneous healing of subclinical pulmonary abscesses on a farm with endemic infections caused by Rhodococcus equi. Vet J. 2012;192:293.
Giguère S, Jacks S, Roberts GD, et al. Retrospective comparison of azithromycin, clarithromycin, and erythromycin for the treatment of foals with Rhodococcus equi pneumonia. J Vet Intern Med. 2004;18:568.
For More Information
American Association of Equine Practitioners: Rhodococcus equi pneumonia
AAEP Infectious disease guidelines: R equi pneumonia
Also see pet health content regarding foal pneumonia.





