

Megaesophagus may be due to a congenital defect or may be an adult-onset, acquired disorder.
Congenital defects that may result in megaesophagus include:
vascular ring anomalies
congenital myasthenia gravis
idiopathic congenital megaesophagus
Adult-onset megaesophagus may be primary (most commonly idiopathic in dogs) or secondary to systemic disease. Secondary megaesophagus may be due to diseases including:
heavy metal (lead) toxicity
thallium toxicity
neurotoxin-induced cholinesterase inhibition
CNS disorders including neoplasia
hypothyroidism
Esophageal dilatation may also develop cranial to an esophageal lesion such as an esophageal stricture, foreign body, neoplasia, or extraesophageal compression. A subgroup of dogs may have lower esophageal sphincter achalasia, characterized by a lack of relaxation of the lower esophageal sphincter in response to pharyngeal swallowing. These dogs suffer from functional lower esophageal sphincter (LES) obstruction. It is critical to distinguish them from the other patients as they may respond to a targeted treatment (see below). Performing videofluoroscopic swallow studies while allowing dogs to stand and free-feed would be recommended to identify this subgroup of dogs.


Contrast esophagram demonstrating dilatation of the esophagus (megaesophagus) in a dog, ventrodorsal projection.
Courtesy of Dr. Ronald Green.

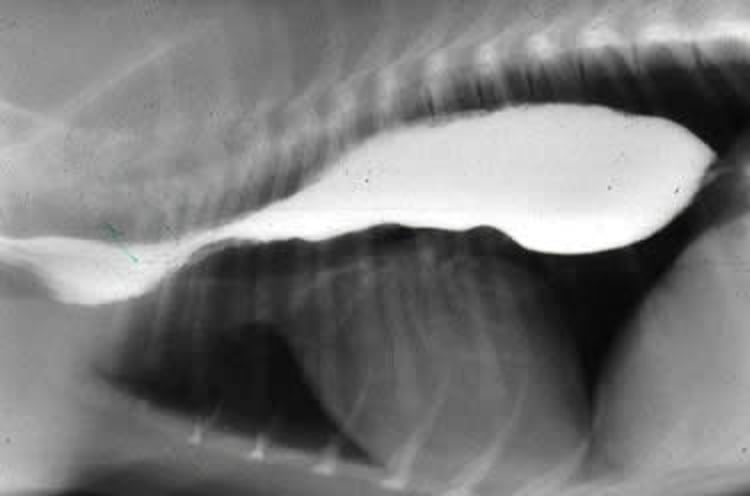
Contrast esophagram demonstrating dilatation of the esophagus (megaesophagus) in a dog, lateral projection.
Courtesy of Dr. Ronald Green.
The cardinal sign is regurgitation. A puppy with congenital megaesophagus characteristically begins to regurgitate at weaning when it starts to eat solid food. Affected pups are generally unthrifty and smaller than their littermates. Pressure applied to the abdomen may cause ballooning of the esophagus at the thoracic inlet. Aspiration pneumonia is a complication with associated clinical signs of cough, fever, and sometimes nasal discharge. Adult animals that develop megaesophagus also start to regurgitate and ultimately lose weight. Respiratory clinical signs may predominate, with little or no apparent regurgitation.
Thoracic radiographs reveal air, fluid, or food in a dilated esophagus. The esophagus is usually uniformly dilated. A large ventral deviation may be present cranial to the heart. Megaesophagus secondary to a stricture, foreign body, neoplasia, or vascular ring anomaly is visualized as a dilatation of the esophagus cranial to the defect only. Strictures, foreign bodies, or vascular ring anomalies can be excluded with an esophagram and/or esophagoscopy.
In adult dogs, associated diseases (eg, myasthenia gravis) should be excluded or, if found, treated. Surgery is indicated for a vascular ring anomaly. Intraoperative endoscopy is recommended to confirm the improvement of esophageal diameter and prolong surgery if necessary. Surgery may not successfully resolve the clinical signs in longstanding cases with severe esophageal dilatation cranial to the anomaly. Medical management is indicated for congenital or acquired idiopathic megaesophagus. Congenital megaesophagus may resolve as the animal ages, usually by 6 months old.
The consistency of the diet that best prevents regurgitation varies from dog to dog; a soft gruel works for some, while dry food works for others. Another possibility is canned food formed into a meatball shape. Frequent, small meals work best for most dogs. Feeding from an elevated position with the forelimbs higher than the hindlimbs and holding that position for at least 10–15 minutes after eating allows gravity to assist food passage into the stomach. Chairs have been commercialized over the years to help hold the dog in position after eating.
Neither surgery nor medications improve esophageal function for idiopathic megaesophagus. Ultimately, most animals succumb to aspiration pneumonia. Survival times of 1–3 months and a mortality rate of 74% have been reported.1 Radiographic evidence of aspiration pneumonia and the age at onset of clinical signs are significantly associated with survival time.
Dogs with lower esophageal sphincter achalasia may respond to mechanical dilation and botulinum toxin injection. Although esophageal dilatation and dysmotility may persist, clinical improvement has been reported in 14 dogs.2 Because the positive effects were short-lived, this mechanical dilation and botulinum toxin type A (BtA) combination is not considered a definitive treatment but rather a test to identify the patients that can benefit from surgical intervention.
Medical management with sildenafil has had variable effects in humans with LES achalasia. A recent study reported improved clinical signs in puppies with congenital megaesophagus treated with sildenafil.3 These dogs may have had some degree of LES obstruction.
References
McBrearty AR, Ramsey IK, Courcier EA, Mellor DJ, Bell R. Clinical factors associated with death before discharge and overall survival time in dogs with generalized megaesophagus. J Am Vet Med Assoc 2011;238(12):1622–1628.
Grobman ME, Hutcheson KD, Lever TE, Mann FA, Reinero CR. Mechanical dilation, botulinum toxin A injection, and surgical myotomy with fundoplication for treatment of lower esophageal sphincter achalasia‐like syndrome in dogs. J Vet Intern Med 2019;33(3):1423–1433.
Quintavalla F, Menozzi A, Pozzoli C, et al. Sildenafil improves clinical signs and radiographic features in dogs with congenital idiopathic megaoesophagus: a randomised controlled trial. Vet Rec 2017;180(16):404.





