

Noninfectious diseases
Heat Stress of Llamas and Alpacas


Photograph of the perineal region of a llama with heat stress. Scrotal edema is a common finding in camelids with heat stress, part of an adaptive mechanism to enhance dissipation of heat.
Courtesy of Dr. LaRue Johnson.
Camelids are adaptable to a wide climatic range and have been successfully raised in regions with winter temperatures as low as –10°C (–14°F) if reasonable wind shelter is provided.
Heat stress is an emergency and can occur in animals with moderate to heavy fiber coats that are subjected to high environmental temperatures and humidity. Subclinical disease, stress, obesity, and overcrowding can also predispose to heat stress.
Signs of heat stress include tachypnea, open-mouthed breathing, shaking, foaming at the mouth, anuria or oliguria, collapse, and coma. Physical examination findings include elevated body temperature (>102°F [38.9°C] and as high as 107°F [41.7°C]; reference range, 99°F to 101.8°F [37.2°C to 38.8°C]), cardiac arrhythmias, thready pulses, and abnormal mentation. Common clinicopathologic findings include metabolic acidosis, electrolyte derangement, thrombocytopenia, markedly elevated hematocrit, and azotemia. Untreated, these animals will develop disseminated intravascular coagulation (DIC), liver and renal failure, intestinal sloughing, multisystem organ failure, and death.
In mild cases, clipping thermal windows in the coat and placing the patient in air-conditioning can be curative. Unfortunately, many cases are advanced by the time they are recognized. Patients should be rapidly clipped of hair, with attention to the abdomen and thorax, and ice packs placed on core regions of the body. Unshorn animals should not be soaked with water because the fiber will trap water and cause additional retention of heat. Cool IV fluid therapy and cool water enemas are helpful. Body temperature should be monitored every few minutes and intensive cooling stopped when rectal temperature decreases to 102°F (38.9°C). If cooling is continued to normal body temperature, the patient will overcool. Unfortunately, many affected animals will decompensate and die within 24 to 72 hours despite initially showing improvement.
Prevention of heat stress is critical. Animals should be sheared in warm weather, and they should be acclimated slowly to warmer environments. Fans, shade, and deep pools are helpful. Veterinary procedures should be scheduled in the cool times of the day, and sedated animals should never be left untended outdoors.
Neoplasia of Llamas and Alpacas
Lymphosarcoma is the only neoplasia found with notable frequency in camelids. It can occur as either a juvenile lymphoma or a primitive malignant round cell tumor. Clinical signs and course vary depending on organ involvement.
Hepatic disease
Camelid Liver


Photograph of the liver of a camelid. Camelids do not have a gallbladder.
Courtesy of Dr. LaRue Johnson.
The visceral surface of the liver normally has multiple fissures, whereas the parietal surface is smooth with indistinct lobation. Camelids do not have a gallbladder. Ultrasonographically, the normal liver is visible by imaging on the right side of the body.
Hepatic lipidosis is arguably the most common liver disease in camelids. Fatty livers occur in crias as well as adults. Pregnant and lactating females are susceptible because of deranged fat mobilization. Inappetant camelids are particularly at risk. Stress and abrupt changes in diet also appear to play roles. Animals that develop hyperlipidemia may have other concurrent problems that need to be addressed for the lipidosis to resolve. Clinical signs and changes in clinicopathologic parameters associated with liver disease in other species are frequently seen in camelids, although acute death without prior indication of pending problems also has been reported. Depending on the underlying cause of the inappetance, nutritional support can be given orally, using an orogastric tube, or parenterally. Diagnosis is through confirmation of elevated concentrations of serum triglycerides and lipids. Ultrasonographic changes of liver echogenicity can also support diagnosis. Treatment of even mild hyperlipemia is necessary in camelids. Furthermore, hydration and electrolytes are likely to be abnormal in affected animals as well, also requiring appropriate therapy. In untreated animals, death is a common sequelae.
Camelids appear to be particularly susceptible to Fasciola hepatica, with fecal shedding beginning 10–12 weeks after infection. Clinical signs can include ill thrift, diminished growth, and acute death. Icterus is rarely seen. Increased serum bile acids concentration (>25 mcmol/L), alkaline phosphatase activity (>121 U/L), or AST activity (>235 U/L) are also diagnostically useful.
Hyperglycemia, Hyperosmolarity, and Insulin Resistance of Llamas and Alpacas
Hyperglycemia, not hypoglycemia, is a typical finding in very sick camelids, with blood glucose concentrations sometimes elevating as high as 500 mg/dL. High glucose levels can be transient, associated with stress; if they return to baseline quickly, they do not require treatment. However, because camelids have low endogenous insulin release and partial insulin resistance, they frequently cope poorly with hyperglycemia and require treatment with insulin. Persistent hyperglycemia can lead to elevated blood osmolarity and neurologic signs. Increased urination and fine muscle tremors are early warning signs. Seizures and coma occur later. Concurrent hypernatremia may be present.
Treatment of hyperglycemia involves administration of regular insulin (0.2 U/kg, IV, every 6 hours for 24 hours). A continuous rate infusion (CRI) of regular insulin is another option. In one report, the insulin solution was prepared by adding 100 U of regular insulin to 500 mL of saline (0.9% NaCl) solution to yield a concentration of 0.2 U/mL. The CRI was administered at an initial rate of 1 mL/hr (0.02 U/kg/hr) and was readjusted regularly based on blood glucose concentration and hydration status.
Treating hyperosmolarity, if present, requires reducing blood glucose concentration while correcting hypernatremia. This can usually be done considerably more rapidly in camelids than in small animals because the disorder itself occurs so quickly that the brain has not had time to produce idiogenic osmoles. Thus, IV administration of half-normal saline (0.45% NaCl) solution can be given along with insulin. In neonates, if oral milk or formula is given, it must be diluted first because of its high sodium content. Repeated monitoring of serum concentrations of glucose and sodium is essential.
Gastrointestinal Diseases
Gastric Ulcers of Llamas and Alpacas
Stomach, llama

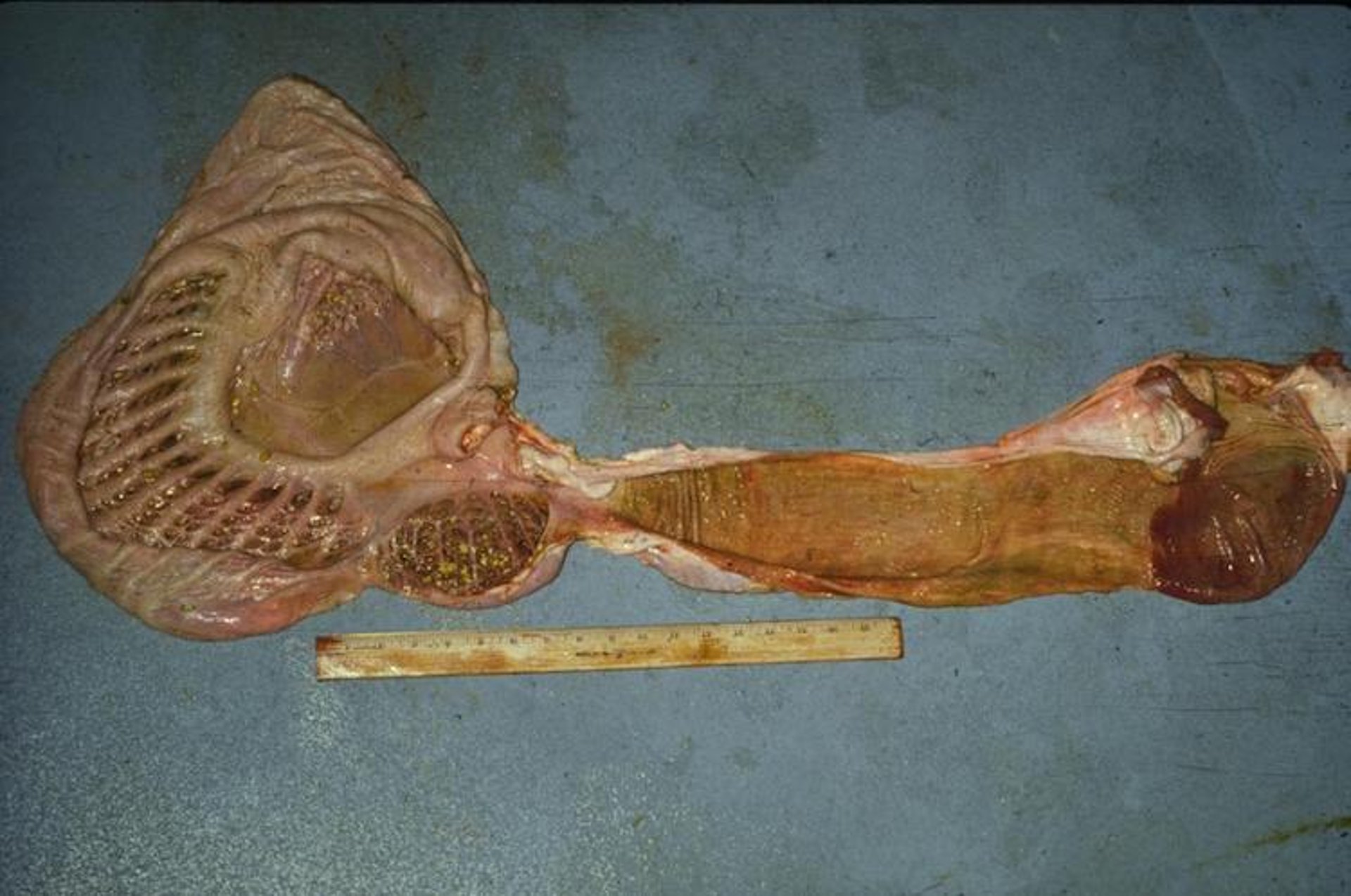
Photograph of a dissected specimen of the stomach of a llama showing the interior (mucosal) aspect. From left to right, note the muscular septae dividing the glandular saccules of the first compartment (C1), the wider saccules of the smaller reniform second compartment (C2), and the long, tubiform third compartment (C3), of which the aborad fifth of the mucosa is thicker and lined with gastric glands. Ruler shown for scale.
Courtesy of Dr. LaRue Johnson.
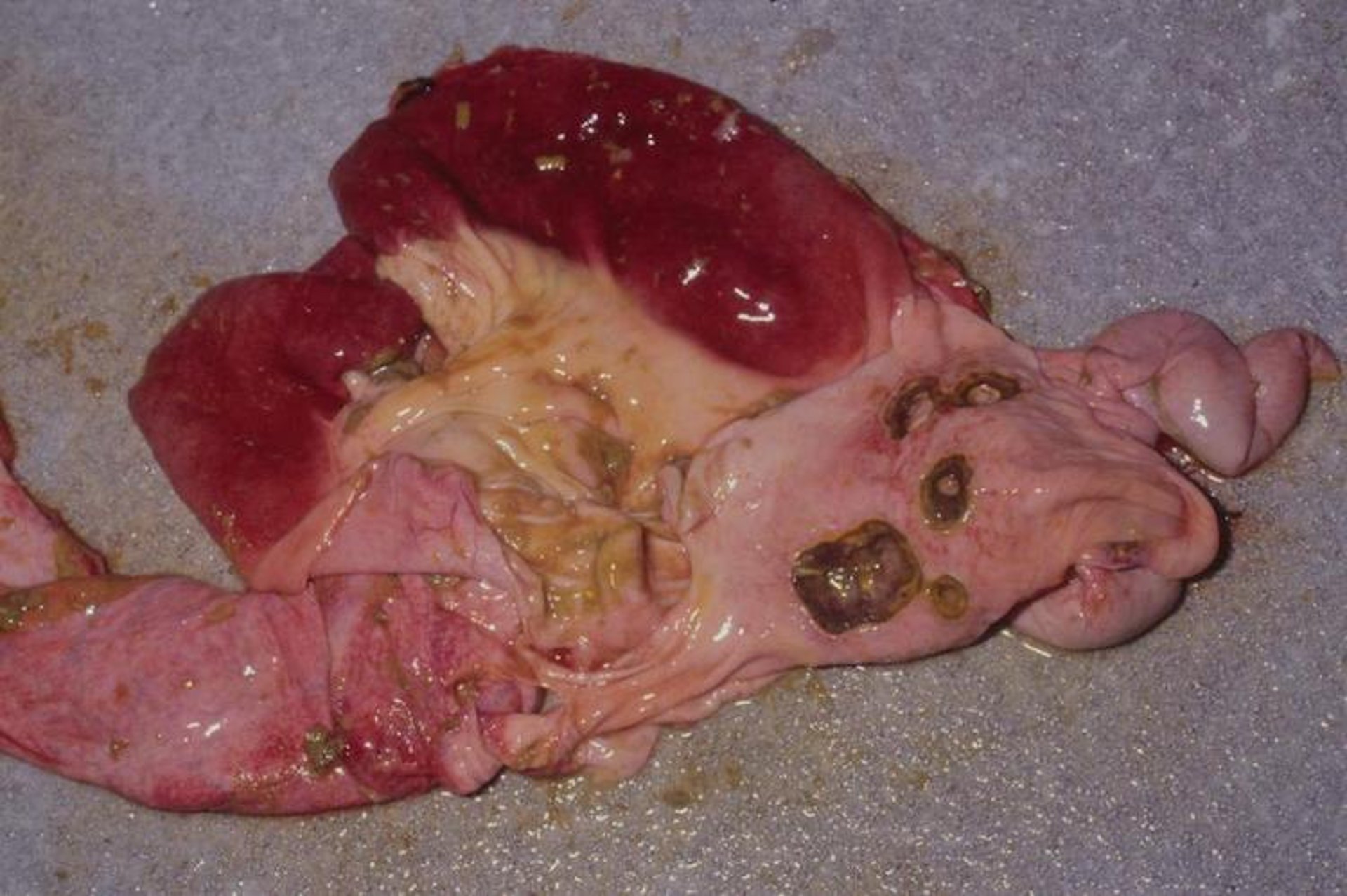
Gross pathology photograph of gastric ulcers in a llama. Ruptured gastric ulcers can cause peritonitis.
Courtesy of Dr. LaRue Johnson.
Partial and complete thickness erosions of the acid-secreting aborad portion of C3 and most proximal portion of the duodenum are not uncommon. Clinical signs may include decreased food consumption, intermittent to severe colic, tooth grinding (bruxism), and depression. Stress appears to be a major component, with problems often developing 3–5 days after change of environment affecting social structure, serious injuries, and illnesses.
No reliable premortem diagnostic procedures are available; treatment is usually based on history and clinical signs. Oral medications such as proton pump blockers and H2 blockers are not effective, although parenteral administration of omeprazole or pantoprazole reduces acid production. Stress reduction, including clinical housing with a cohort animal, parenteral antimicrobials, and supportive therapy, is helpful. Gastric ulcers secondary to another disease process may resolve after successful treatment of the primary problem.
Megaesophagus of Llamas and Alpacas
Moderate to severe dilatation of the esophagus is relatively common in llamas and alpacas. Clinical signs include chronic weight loss, sometimes in conjunction with postprandial regurgitation, hypersalivation, and excess frothing at the mouth associated with eating. No identified age or sex predilection has been identified, nor any consistent causes. A suspected case of megaesophagus should be confirmed with barium contrast radiography or fluoroscopy. No treatments have been consistently successful, but altering diet to make swallowing easier and offering feed on an elevated platform can sometimes alleviate clinical signs somewhat. The long-term prognosis is fair to poor, with some animals maintaining condition for an extended period and others continuing to lose weight.
Small and Large Intestinal Diseases of Llamas and Alpacas
Diarrhea is relatively uncommon in llamas and alpacas. Shortly after birth, crias may develop mild diarrhea due to abundant dam milk production, essentially a substrate purge. The primary recognized infectious causes of diarrhea in neonates include rotavirus, coronavirus, cryptosporidia, and enteropathogenic strains of Escherichia coli. Some crias also have transitory diarrhea 2–3 weeks after birth, at about the time they experience new food matter. During this time, some crias will develop colic signs due to blockage in the spiral colon. Diarrhea in older neonates is more likely associated with Eimeria spp infection, especially associated with the stress of weaning. Identified causes of diarrhea in older animals include Yersinia pseudotuberculosis, Salmonella spp, Giardia spp, and Cryptosporidium parvum. Treatment options are the same as for other species (ie, fluid and electrolyte replacement and appropriate antibacterials).
Diarrhea in adult camelids is relatively rare but often accompanies a change of feed. Serious conditions characterized by diarrhea include eosinophilic enteritis, infection with Eimeria macusaniensis or Mycobacterium paratuberculosis, or severe nematode parasitism. In contrast to cattle with Johne's disease, the clinical course in camelids tends to be short and fatal. When diagnosed by fecal examination, E macusaniensis must be promptly treated, because infection can cause marked debilitation. Although variable, current treatment recommendations include oral administration of ponazuril followed by parenteral administration of sulfadimethoxine.
Stomach Atony of Llamas and Alpacas
Gastric atony is an occasional problem of unknown cause in camelids. Clinical signs include decreased or complete cessation of food consumption, loss of body condition, and depression. Other GI problems, including diarrhea, may be present. Supportive therapy, including fluids, is frequently helpful. Lack of food for 3–5 days also usually causes the death of bacteria and protozoa in C1 and C2. Transfaunation (0.5–1 L) of camelid C1 or strained rumen contents (sheep or cow), administered by gavage, frequently results in a dramatic improvement in appetite and reestablishment of appropriate flora.
Congenital Diseases
Although few congenital anomalies have conclusively been shown to be genetic in origin, it is assumed that defects inherited in other species are inherited in camelids as well. Accordingly, this should be considered in breeding decisions. Facial and cardiac defects are reported to be the most frequent inherited anomalies. A historically narrow gene pool is likely the reason that congenital defects are relatively common in camelids. Affected individuals commonly have more than one defect.


Photograph of a llama cria with choanal atresia. For diagnostic procedures, a tracheostomy has been performed.
Courtesy of Dr. LaRue Johnson.
Choanal atresia, a condition caused by failure of the inner nares (choanae) to open during embryologic development, is the most widespread congenital defect. It can be unilateral or bilateral and may result in complete or partial blockage. Because camelids are obligate nasal breathers, the primary clinical presentation is a variable degree of respiratory distress in the neonate. Distress becomes more apparent during nursing, and crias commonly gasp as milk is inhaled. Surgical correction is not recommended.


Photograph of an alpaca with campylorrhinus lateralis (wry nose).
Courtesy of Dr. Ellen Wiedner.

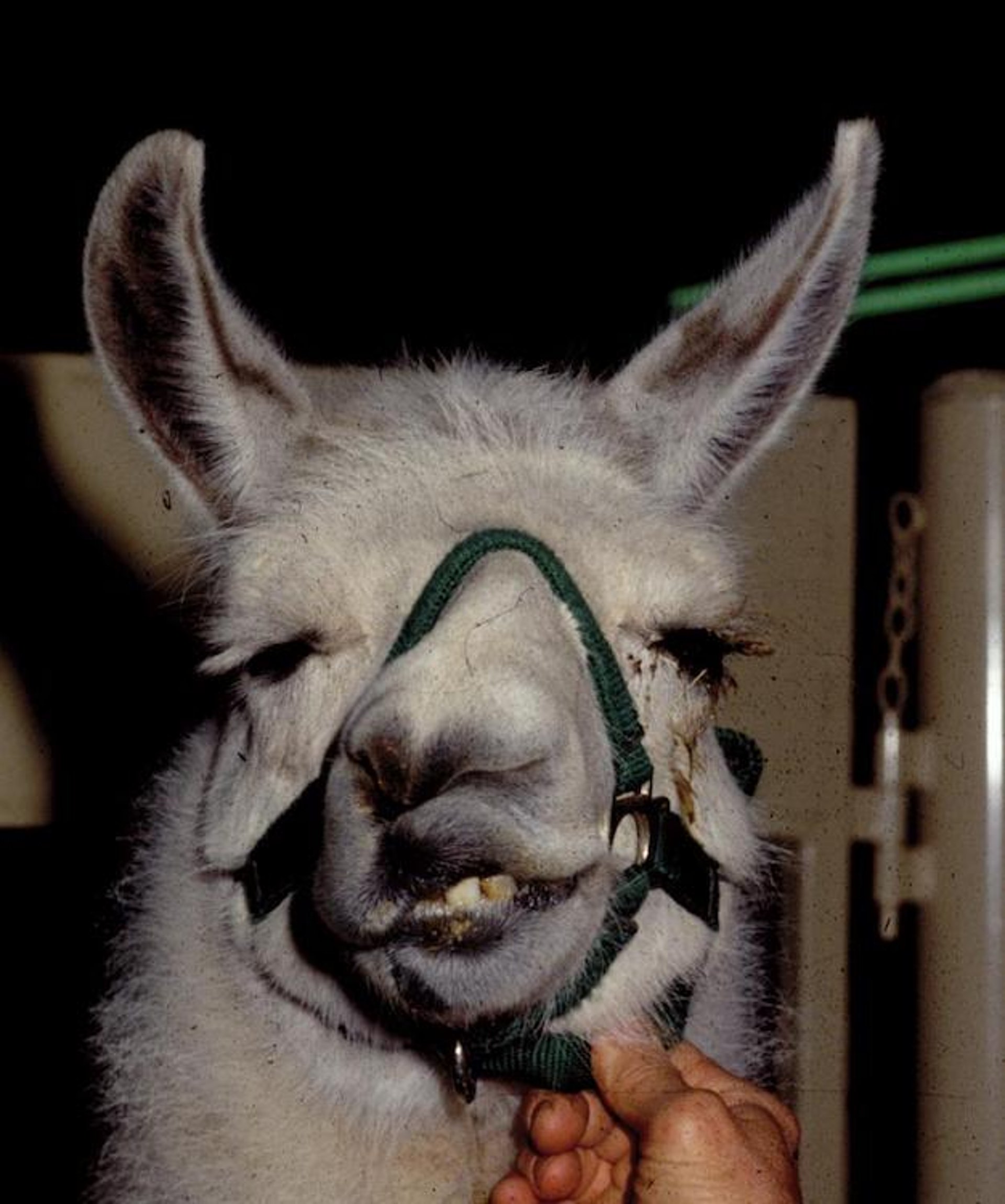
Photograph of a llama with lateral deviation of the maxilla (wry face).
Courtesy of Dr. LaRue Johnson.
Maxillofacial dysgenesis (wry face or wry nose) is characterized by a slight (< 5°) to severe (>60°) lateral deviation of the maxilla. The mandible may or may not have a similar deviation (campylognathia). When severe, occlusion of the nares and lack of apposition of the incisors and dental pad usually necessitate euthanasia of the cria. There appears to be a relationship of this defect to choanal atresia, in that they occasionally occur together.

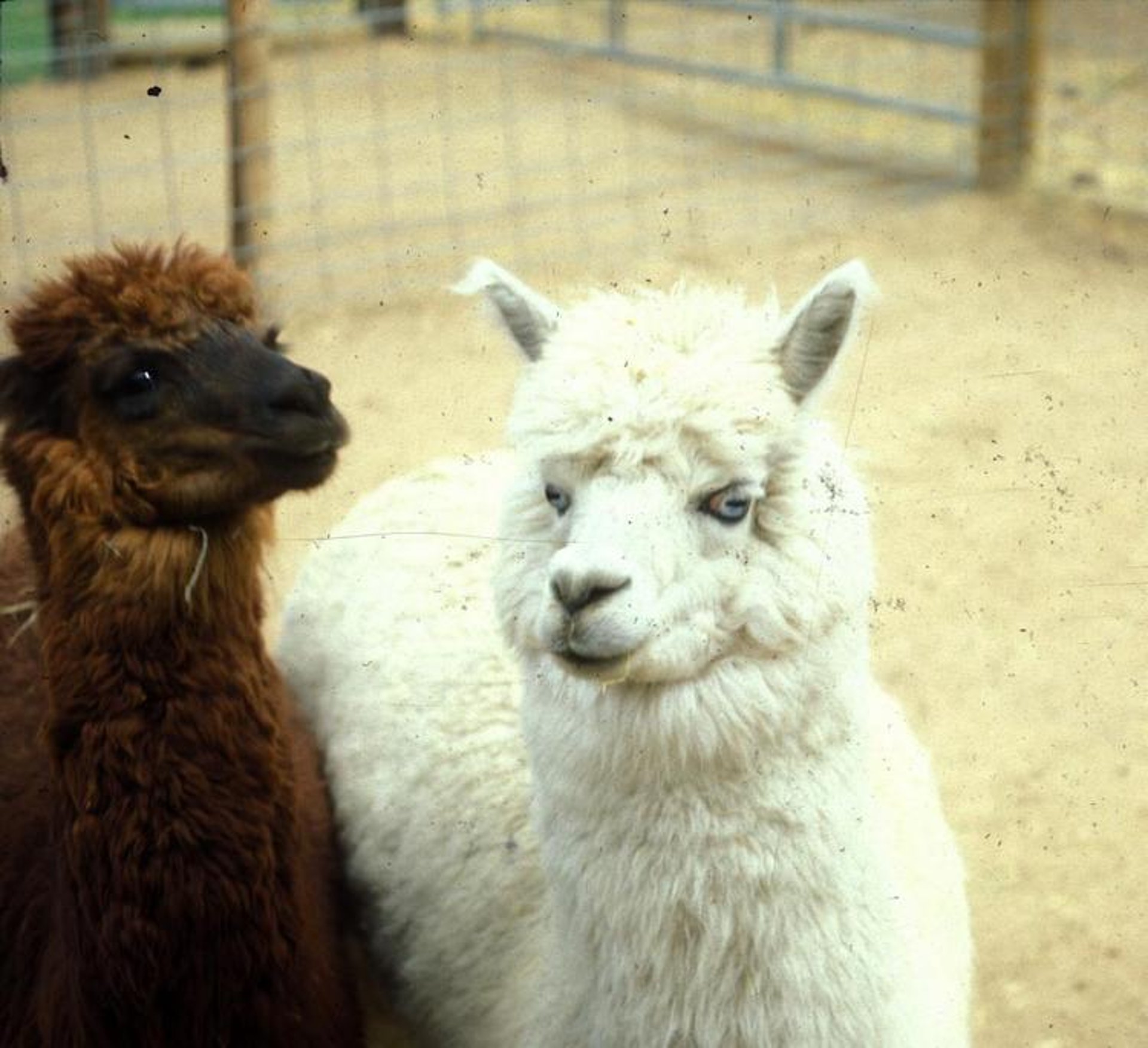
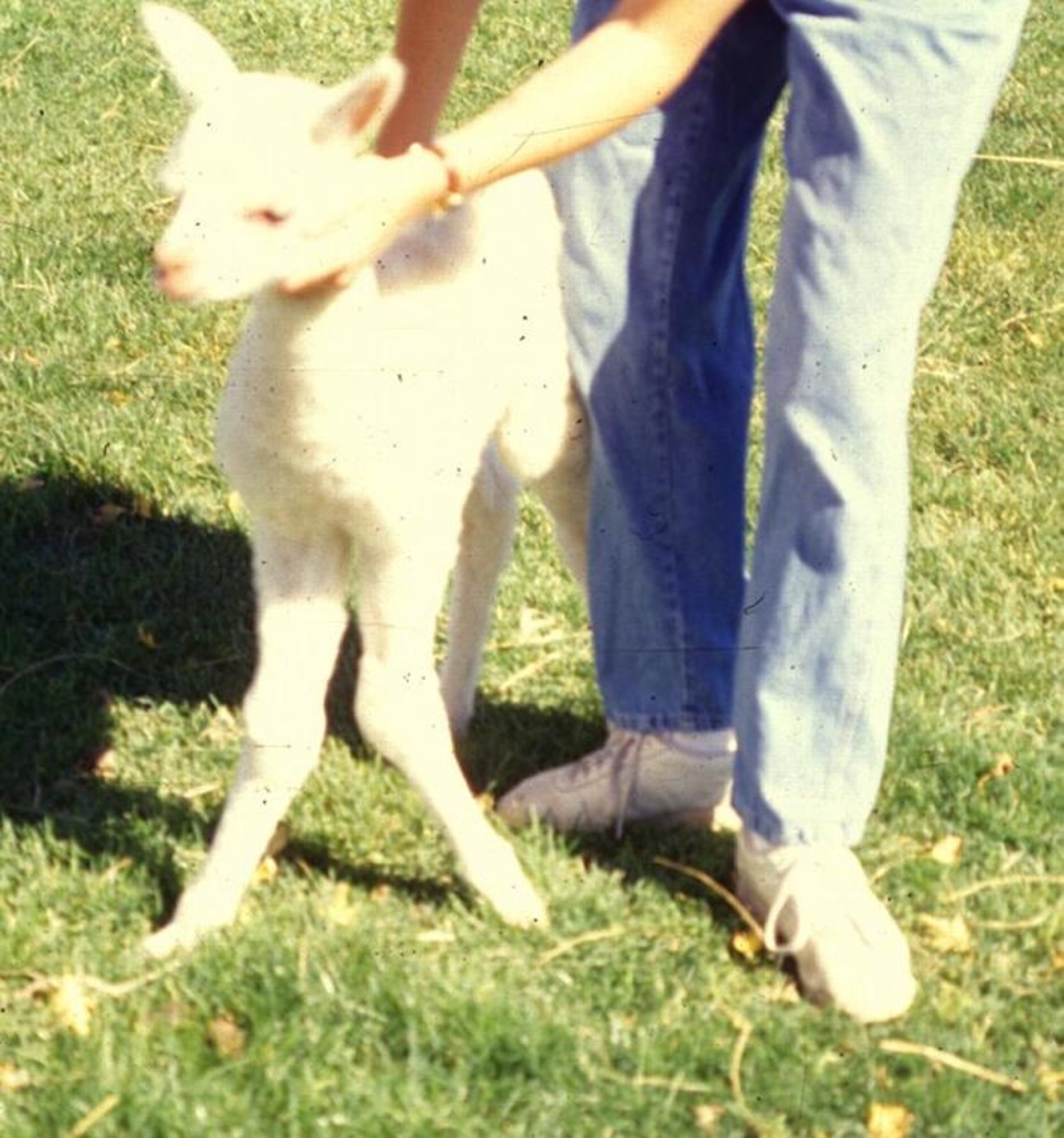
Photograph of a white alpaca with blue eyes. There is an association between blue eyes and deafness in some lines of white animals.
Courtesy of Dr. LaRue Johnson.


Photograph of a llama with short pinnae (so-called gopher ears), a heritable trait.
Courtesy of Dr. LaRue Johnson.
Ocular and ear conditions include juvenile cataracts (seen occasionally), blocked nasolacrimal ducts, and an association between blue eyes and deafness in some lines of white animals. Fused (tip or base) and short pinnae (“gopher ears”) are recognized heritable defects, the latter appearing to be a dominant trait.
Cardiac defects are relatively common, with ventricular septal defects being most typical.


Gross pathology photograph displaying a ventricular septal defect (VSD) in the heart of a llama. This is the most common type of heart defect in alpacas and llamas. Affected crias may die suddenly or may fail to thrive. Small defects may result in no overt signs. A holosystolic murmur may be auscultated with a point of maximal intensity on the right.
Courtesy of Dr. LaRue Johnson.


Photograph of a newborn llama cria with polydactyly, a common congenital condition with a presumed genetic basis.
Courtesy of Dr. LaRue Johnson.

Photograph of a young alpaca with an angular limb deformity (valgus deformity of both forelimbs at the carpus).
Courtesy of Dr. LaRue Johnson.
Numerous musculoskeletal defects have been identified, including syndactyly and polydactyly. Arthrogryposis, rotated talus, angular limb deformities of the front limbs, and tendon laxity are also seen.
Other congenital anomalies identified in llamas and alpacas include atresia ani, atresia coli, umbilical hernias, and several types of tail defects, including a pronounced lateral deviation of the tail at the base.
Urogenital defects are much more common in camelids than in other species. Important defects in females include uterus unicornis, hypoplastic ovaries, double cervices, segmental aplasia of the vagina or uterus, and clitoral hypertrophy, suggesting intersex conditions. Unilateral absence of a kidney is periodically seen, commonly in association with choanal atresia. Total absence of kidneys has also been seen. Congenital conditions in males include hypospadias, retained testicles, testicular hypoplasia, persistent frenulum, ectopic testicles, and corkscrew penis.
Dermatologic disease
Copper Deficiency of Llamas and Alpacas
Copper deficiency is characterized by depigmentation of fiber with a wiry or steely texture. Juvenile llamas and alpacas with copper deficiency grow poorly and are predisposed to infections. Confirmation of deficiency is best based on comparison of liver copper levels with normal ranges for species. Treatment requires dietary supplementation. However, excessive supplementation will cause copper toxicosis, which has been diagnosed more commonly than copper deficiency.
Dorsal Nasal Alopecia (Dark Nose Syndrome) of Llamas and Alpacas


Photograph of an alpaca with alopecia over the dorsal bridge of the nose. This may be due to rubbing, such as due to pruritus from ectoparasite activity and seems over-represented in dark-haired animals (hence the name dark nose syndrome).
Courtesy of Dr. LaRue Johnson.
Dorsal nasal alopecia, or dark nose syndrome, is characterized by dermatitis over the bridge of the nose. The skin is normal or variably scaly, hyperpigmented, and thickened. Dark-haired animals are predisposed, presumably because insects prefer the warmer surface of a dark background. In some animals, the condition may be secondary to rubbing the nose; in others, it may be a fly bite exacerbation, but many cases are due to burrowing mites. Diagnosis should be by analysis of multiple deep skin scrapings or biopsy. In cases unrelated to parasitism, administration of systemic or topical steroids produce some transient response, but steroids may cause abortion in camelids. In northern climates, the condition tends to spontaneously improve during winter months. Alopecia of the ears has also been seen, particularly in black alpacas.
Zinc-Responsive Dermatosis of Llamas and Alpacas


Photograph of a llama with zinc-responsive dermatosis.
Courtesy of Dr. LaRue Johnson.
Zinc-responsive dermatosis, also known as idiopathic hyperkeratosis, occurs in llamas and alpacas of any age. The lesions appear as nonpruritic papules with a tightly adherent crust. Papules progress to plaques and then large areas of thickening and crusting. Lesions are most common in the less densely haired areas of the perineum, ventral abdomen, inguinal region, medial thighs, axilla, and medial forearms, but the face may also be involved. The clinical signs may wax and wane. Diagnosis is by analysis of affected skin biopsy. Treatment is administration of zinc sulfate (1 g/day) or zinc methionine (2–4 g/day). Calcium supplementation should be minimized and alfalfa hay discontinued. Affected animals do not necessarily have zinc deficiency.
Munge of Llamas and Alpacas


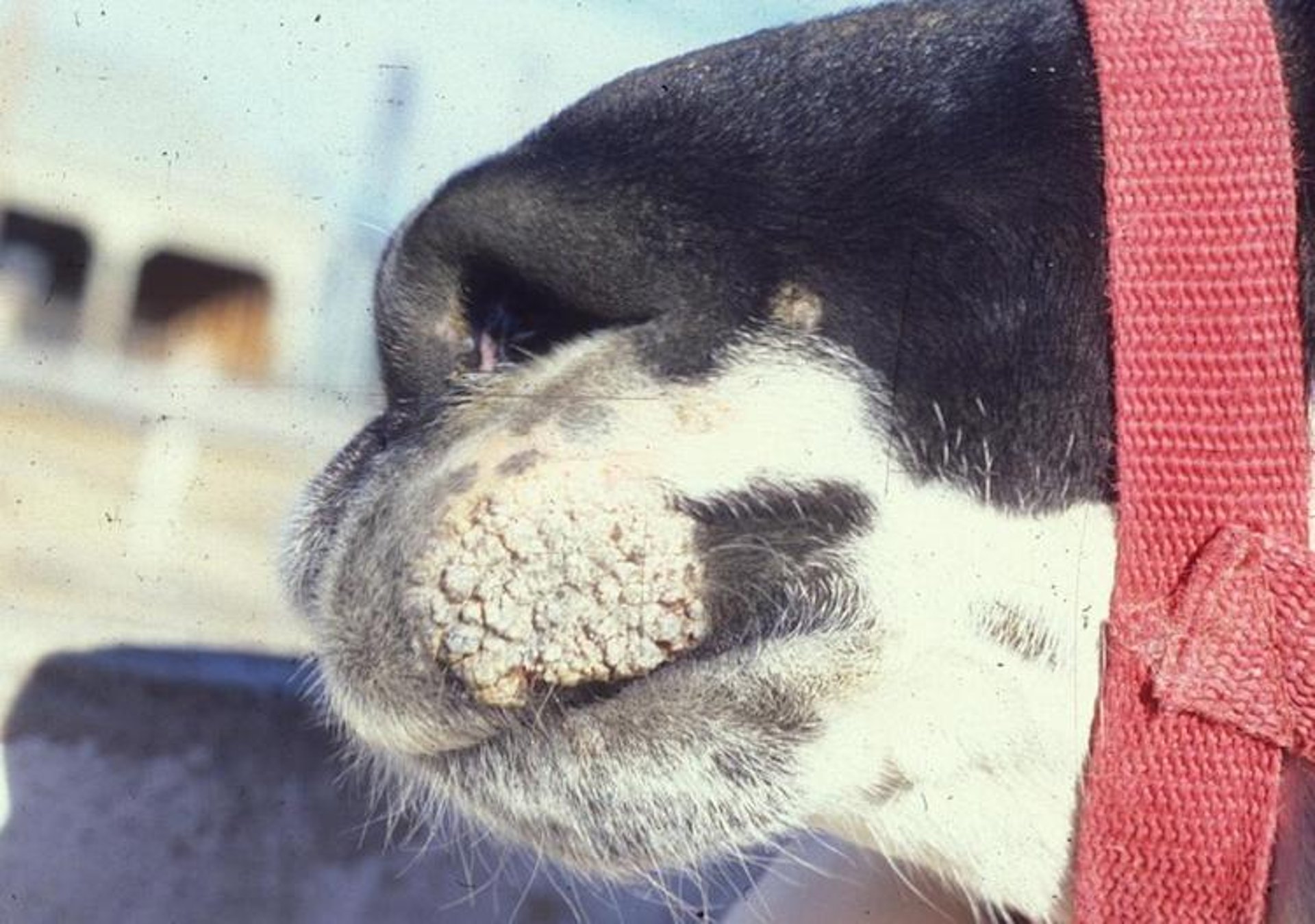
Photograph of a llama with perinasal munge. In severe cases, thick crusts may obstruct the nostrils.
Courtesy of Dr. LaRue Johnson.

Photograph of an older llama with perioral superficial hyperkeratotic dermatitis (munge). Munge appears similar to many other camelid skin disorders.
Courtesy of Dr. LaRue Johnson.


Photograph of the ear of a llama affected with dermatophytosis. Lesions are typically alopecic with thick crusts. Fungal infections from dermatophytes are potentially zoonotic.
Courtesy of Dr. LaRue Johnson.
Munge refers to severe dermatitis in camelids. This syndrome is characterized by variable degrees of heavy, adherent, hyperkeratotic crusts in paranasal and perioral regions. Sometimes, the bridge of the nose and periocular and periaural regions are affected. Inflammatory lesions may wax and wane. Differential diagnoses include viral contagious pustular dermatitis, dermatophilosis, dermatophytosis, bacterial dermatitis, and immune-mediated disease. Some cases of suspected munge turn out to be sarcoptic mange. Treatment is directed at resolving secondary bacterial infections and the primary problem, if known. Sarcoptic mange in camelids usually requires biopsy for confirmation, then treatment with antiparasitics.
Some animals do not respond to any therapy, including those affected with juvenile llama immune deficiency syndrome, a congenital condition affecting both llamas and alpacas. In these cases, an evaluation of the immune response is indicated, as well as further work-up for other medical conditions.
Bacterial Diseases
Brucellosis, tuberculosis, and Johne's disease (paratuberculosis) have been identified in camelids, although the naturally occurring incidence of these infections is low. Reported cases of both type C and D Clostridium perfringens have prompted the administration of toxoid vaccination as a routine measure in most herds. Although camelids are not apparently highly susceptible to tetanus, most herd vaccinations using the C/D toxoid include tetanus toxoid.
Clostridium perfringens type A is an important pathogen under stressful circumstances, especially in South America, and results in a high death rate in crias < 4 weeks old. Enterotoxigenic strains of C perfringens type A are believed to be particularly lethal. Clinical signs are similar to those of type A infections in other species, with a rapid onset of neurologic clinical signs followed shortly by death.
Anthrax has been diagnosed in camelids, but vaccination should only be done in endemic areas using a killed product.
Respiratory infections in North America caused by bacteria remain relatively rare, but in South America the condition referred to as alpaca fever is caused by Streptococcus zooepidemicus. The onset of this condition is often preceded by stressful conditions.
Individual cases and herd problems with abscesses caused by Corynebacterium pseudotuberculosis have been reported. Contact with sheep and shearing wounds are likely contributing factors.
Johne's disease, or paratuberculosis, caused by Mycobacterium avium subsp paratuberculosis, is becoming an increasingly important disease of camelids. Paratuberculosis causes a protein-losing enteropathy characterized in camelids by weight loss and edema, and sometimes, but not always, diarrhea. Clinical signs may appear long after infection. During the incubation period, the animal can shed infectious organisms in its feces. One study found a prevalence of 6% in the US. Diagnosis is through analysis of fecal culture and fecal PCR assay. No treatment exists. Affected animals should be culled or relocated elsewhere. Newborns should not be allowed to nurse from confirmed paratuberculosis-positive mothers. Any purchased colostrum or milk replacer should come from facilities confirmed as free from Johne's disease.
Tuberculosis is also being recognized increasingly in camelids, primarily in Europe. In the United Kingdom. Mycobacterium pinnipedii, a member of the Mycobacterium tuberculosis (Mtb) complex, is often cultured from affected animals. Mycobacterium bovis and Mycobacterium microti have also been cultured from camelids. Symptoms of tuberculosis in camelids are often nonspecific and include lethargy, decreased appetite, and weight loss. Occasional coughing or other mild respiratory symptoms can occur. Sudden death has been reported. Latency of the disease, as occurs in other species and humans, is thought to occur in camelids, but remains unstudied.
Diagnosis of tuberculosis can be challenging. The serologic tests lack sensitivity and specificity, and the tuberculin purified protein derivative (PPD) skin test, typically performed by intradermal injection in the axillary region of camelids, often produces both false-positive and false-negative results. During necropsy, granulomas are typically found in the lungs and sometimes in the lymph nodes, containing few acid-fast bacilli. Treatment in animals diagnosed antemortem is generally not attempted, in part because of the human health risks of being in long-term close proximity to affected animals.
Corynebacterium pseudotuberculosis, the cause of caseous lymphadenitis in ruminants, also affects camelids. Other Corynebacteria may be involved too. Animals typically develop large abscesses in the lymph nodes, most commonly the retropharyngeal, axillary or popliteal nodes, although any lymph nodes can be affected. Unlike a typical abscess, the affected lymph nodes are cool to the touch. The disease is highly contagious to other camelids and to ruminants and may be zoonotic. The organisms are spread into the environment when the abscesses break open and drain. Transmission can occur through ingestion, inhalation, or direct contact with wounds. Affected animals are usually otherwise bright and alert. Systemic infection, which occurs in domestic ruminants, has not been reported in camelids. Diagnosis is through culture of the abscessed material. Serologic analysis, used for diagnosis in domestic ruminants, has not been studied in camelids. Treatment usually involves surgical removal of the abscesses, although animals should still be considered infected even if the abscesses are removed. Antimicrobials are not recommended until after surgery.
Viral Diseases
West Nile virus is an arthropod-borne flavivirus. Camelids are dead-end hosts, and most animals that seroconvert never show clinical signs. However, if present, clinical signs include neurologic and include asymmetric ataxia, sudden blindness, paralysis, and head tremors. Care is supportive, and 50% of clinically affected animals recover fully. Antemortem diagnosis can be difficult, but a 4-fold increase in serum titers within two weeks in conjunction with neurologic signs are suggestive. Postmortem diagnosis can be done by PCR assay, viral isolation, or immunohistochemistry analysis from affected tissue. The use of equine vaccines against West Nile virus is debatable, in part because the disease is rare. Administration of three vaccines at 3-week intervals has been shown to provide titers in llamas and alpacas, but whether the titers are protective remains untested. The titers are also short-lived, and no challenge studies have been performed. Vaccine reactions have been reported ranging from injection site swellings to anaphylaxis. Prevention generally focuses on mosquito control, including the use of pesticides, removal of standing water, and movement of the animals into barns equipped with working fans at night.
Bovine viral diarrhea virus (BVDV)—a pestivirus and the causative agent of bovine viral diarrhea and mucosal disease complex—appears to be an emerging pathogen of camelids. Alpacas are empirically more susceptible than llamas. Multiple subgenotypes have been identified, but noncytopathic BVDV 1b appears most common. A unique camelid pestivirus has not yet been identified; however, it is suspected to exist. Clinical signs in camelids include ill thrift, lethargy, weight loss, nasal discharge, and pneumonia. Infection with BVDV also causes abortion, stillbirth, and weak premature neonates, but some animals will remain subclinically affected. Cattle may be a source of the disease. The pathophysiology of BVDV infection in camelids is different from ruminants and has not been fully elucidated. Transmission occurs through contact with any variety of infected body fluids and secretions. Persistently infected (PI) crias are important sources of transmission because they often have copious nasal secretions containing large amounts of virus.
Persistently infected crias can have acute or chronic disease, although the latter is more common. Persistently infected crias will be stunted, anemic, or leukopenic and have swollen joints or pneumonia that fail to respond to antimicrobials. Cases can be difficult to distinguish from failure of passive transfer of immunity (which may be a co-morbidity) or juvenile llama immunodeficiency syndrome, which is uncommon. Cerebellar hypoplasia, often seen in calves, has not been reported in camelids, nor has mucosal disease. In addition, necropsy findings may be minimal; this is another difference between camelids and cattle.
In camelids, PCR assay of whole blood is the currently recommended diagnostic method for BVDV. Virus isolation can also be done on blood or tissues; ELISA has not been validated in camelids. If results of virus isolation tests are positive on a live animal, the test should be repeated several weeks later to see whether the animal has cleared the infection or is persistently infected. Paired serum samples with 4-fold increases in antibodies are suggestive of active infection. Herd screening can be done via PCR assay on pooled blood samples. However, serum neutralization testing cannot be used on vaccinated animals and will not detect PI animals because they do not produce antibodies.
Vaccination using a killed BVDV cattle vaccine has been used but is still not widely recommended until more data are available. Vaccination also interferes with some of the diagnostic techniques. Prevention includes keeping a closed herd, repeated screening, and excellent hygiene.
Equine herpesvirus (EHV-1) can cause blindness, encephalitis, and death in camelids. The efficacy of equine vaccines is unclear; however, if used, they should be limited to killed vaccines. Because EHV-1 is highly contagious, prevention is important. Caretakers working with horses in areas where EHV-1 has been reported should change boots and clothing between camelid and equine holding facilities. Fomite transmission means that handwashing and equipment disinfection are essential.
Eastern equine encephalitis is caused by an alphavirus (Togaviridae) transmitted by mosquitoes. Camelids are dead-end hosts. Clinical signs are acute CNS disease, including head twitching, seizures, cranial nerve defects, and most commonly, sudden death. No treatment is available. Diagnosis is difficult antemortem, but increased protein concentration in CSF may be seen with the disease. Diagnosis at necropsy can be done using PCR assay and immunohistochemistry analysis on nervous system tissue. Vaccination using three doses of a bivalent killed equine vaccine produces titers, but the duration of protection is not known.
Foot and mouth disease (FMD) is caused by a picornavirus. Until recently, camelids were not thought to be susceptible. Recently Bactrian camels have been shown to be able not only to contract the disease but also to transmit it, but whether this is the case in New World camelids is unknown. Although camelids do not seem particularly susceptible to the disease, importation of camelids into the US from countries in South America with FMD has been blocked. The carrier status of infected animals is presumed to be of short duration. The hallmark of foot and mouth disease is vesicles on mucous membranes. Other causes of vesicles are vesicular stomatitis and hepatic photosensitization from eating certain plants.
Contagious ecthyma, also known as orf, is caused by a zoonotic parapoxvirus. Typically, patients present with crusty lesions on the nose and mouth. The disease can be contracted through direct contact with infected ruminants, by fomites, and from scabs in the environment. Handlers who see muzzle lesions should wear gloves and be attentive to hygiene. Usually, animals recover with supportive care.
Bluetongue, caused by an orbivirus, has begun to emerge as a clinical entity in camelids. Transmitted by Culicoides biting midges as well as in utero, from mother to fetus, the disease can cause high morbidity and mortality. Characterized by severe and sudden respiratory distress caused primarily by pulmonary edema, antemortem diagnosis can be challenging, and no data are available on whether vaccination with ruminant vaccines would be protective. Many camelids will seroconvert without showing clinical signs of the disease. Active disease requires PCR assay for diagnosis.
An outbreak in 2007 of respiratory disease, principally in alpacas, was found to be caused by alpaca respiratory coronavirus. Stress conditions often predispose camelids to the onset of clinical presentations that vary from mild upper respiratory tract disease to severe respiratory disease and death. Most camelids are seropositive for a presumptively nonpathogenic adenovirus specific to llamas.
Mycoplasma Infection

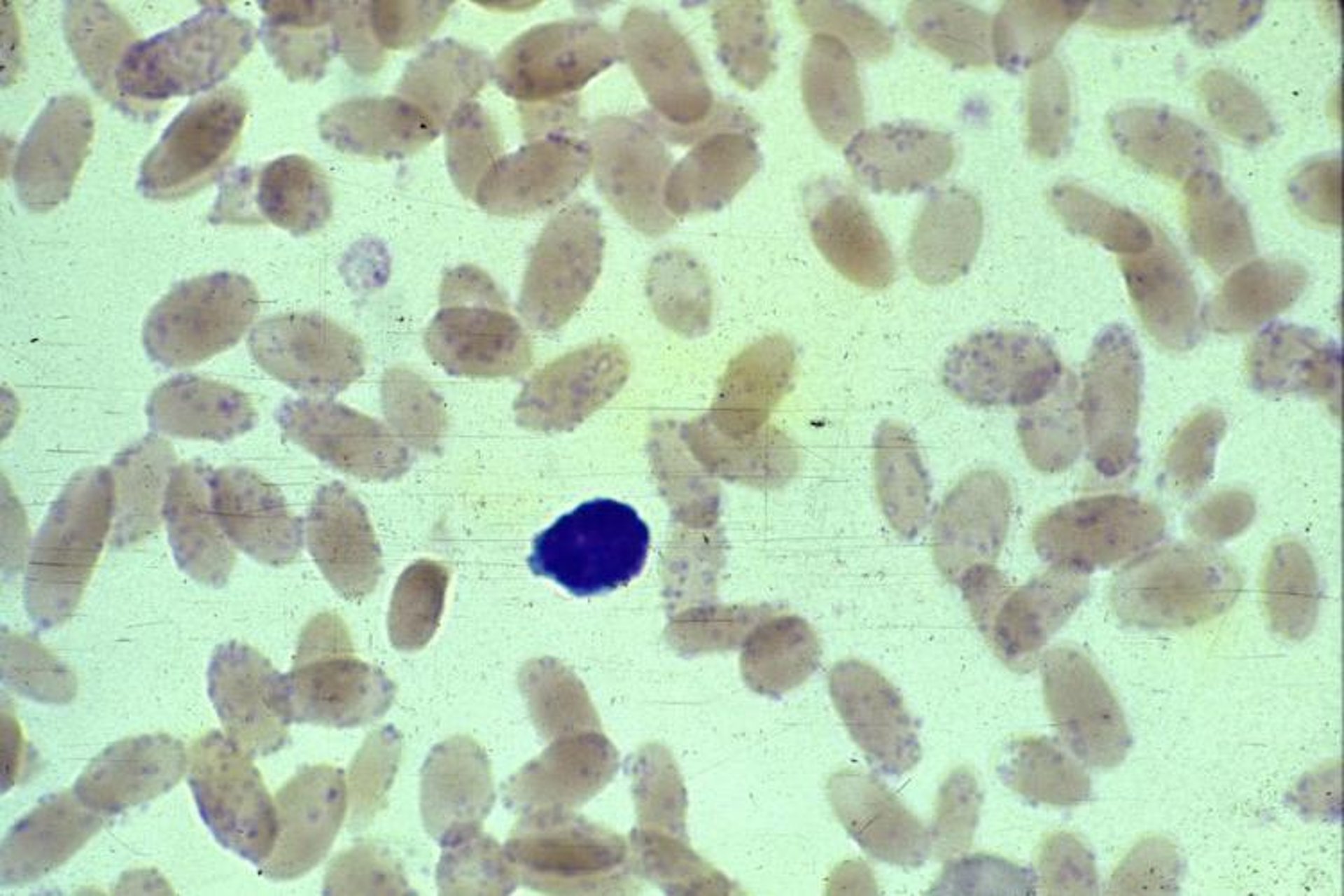
Photomicrograph of a peripheral blood smear from a llama with hemotropic mycoplasmosis. Mycoplasma haemolamae appear as blue-staining coccoid or ringlet forms singularly or in clusters or chains on the erythrocyte membrane. Cytologic examination has low sensitivity for detection of hemoplasmas. Artifact such as stain precipitate, basophilic stippling, or Howell-Jolly bodies can result in false positives. Commercial Romanowsky stain variant; camelid RBCs diameter = 7–8 mcm along the major axis.
Courtesy of Dr. LaRue Johnson.
Mycoplasma haemolamae (formerly Eperythrozoon) is an opportunistic blood-borne organism that can cause mild to fatal anemia. Some infected camelids will have no clinical signs. Diagnosis is through PCR assay or blood smear evaluation, and the presence of this organism should alert the veterinarian to other underlying diseases or stressors, such as malnutrition or immunosuppression. Little is known about Mycoplasma pathogenesis in camelids, but biting insects and vertical transmission are believed to occur. Treatment is with oxytetracycline antimicrobial therapy and, in severe cases, with blood transfusion, but many animals remain chronic carriers.
Enterotoxemia, caused by Clostridium perfringens, can be fatal in neonates. Prevention is through vaccination. Listeria monocytogenes has recently been shown to be the cause of death in neonatal camelids, too.
Fungal infections
Coccidioidomycosis, sometimes called valley fever, is caused by the fungi Coccidioides immitis and Coccidioides posadasii. The fungi grow only in certain parts of the US, specifically Arizona and California. The disease is insidious, and although management is possible for periods of time using various antifungals, overall prognosis is poor. Nonspecific clinical signs include lethargy and weight loss. Abortion attributable to coccidioidomycosis has also been reported. Diagnosis is via radiographs, transtracheal washes, or bronchoalveolar lavage. The disease causes the formation of granulomas in lungs, lymph nodes, and kidneys.
Fungal keratitis is fairly common in camelids. Aspergillus fumigatus and Fusarium solani are most often cultured. Animals present with stromal abscesses, corneal perforation, stromal ulcers or nonulcerative keratitis, and severe blepharospasm. Most are successfully treated with topical medications.
Medical procedures used in camelids
Jugular venipuncture can be challenging in camelids. A jugular furrow is not appreciable, and their neck skin is thick and covered in fiber. Clipping of the hair is generally not done as the hair takes a long time to regrow. If possible, venipuncture should be performed on the right side of the neck to avoid the esophagus. The external jugular vein is midway between the space occupied by the ventral processes of the cervical vertebrae and the trachea. These sites can be palpated by the thumb and fingers. Venipuncture is usually performed either high up on the neck, level with the angle of the mandible, or more distal at the base of the neck, at the level of the fifth cervical vertebra. The latter site has the advantageous of having thinner skin. Appropriate restraint is needed.


Photograph of the ear of a llama with an IV catheter inserted.
Courtesy of Dr. Ellen Wiedner.
In adult camelids, 16- and 18-gauge jugular catheters are commonly used. Either 3.5- or 5.0-inch catheters can be used. As with venipuncture, identifying the appropriate site on the right side of the neck is key to placement. The head should be in a neutral position, and lidocaine should be injected subcutaneously at the catheter site prior to insertion (approximately 0.3 mL, SC, once). Appropriate restraint is necessary.
Camelids do not have extensive muscling on their thighs and rump, so most intramuscular injections are performed in the cranial aspect of the neck, where the carotid artery is deeper and less likely to be punctured. Nevertheless, this area is still not particularly well-muscled, and other routes of administration should be considered, particularly if multiple injections or a series of injections are planned. Subcutaneous injections are typically given in the axillae or cranial to the scapulae.
Orogastric intubation requires use of a small speculum. A suitable speculum can be fashioned out of a 6-mL syringe case (the ends should be filed to remove sharp edges) and a foal nasogastric tube. Sufficient restraint is needed. The speculum is slipped into the interdental space, then a well-lubricated tube is inserted through the speculum. This technique can be used to administer oral medications, for transfaunation, or to relieve excess air or fluid.





