

Rhodococcus infection causes pyogranulomatous disease, typically suppurative pneumonia, lymphadenitis, and abscesses in other organs, and affects both animals and humans. It is caused by Rhodococcus equi (formerly Corynebacterium equi), an opportunistic, ubiquitous soilborne bacterium. It is found worldwide and is a pathogen of major importance to equine breeding activities.
Etiology of Rhodococcus Infection in Animals
Rhodococcus spp belong to the Actinobacteria class, taxonomically related to the genera Mycobacterium, Corynebacterium, Actinomyces, and Nocardia. Actinobacteria are pathogens associated with diverse diseases in animals and humans.
More than 40 species of rhodococci are known; however, R equi is the main cause of infections in humans and animals. R equi is a facultative intracellular, nonmotile, non-spore-forming, partially acid-fast, gram-positive bacterium. On Gram staining, bacteria appear as cocci or rod-shaped (pleomorphic) organisms.
These aerobic actinomycetes grow in non-enriched media such as nutrient agar and sheep blood agar. When cultured aerobically on blood agar incubated at 30°C–37°C [86°F–98.6°F], smooth, nonhemolytic, mucoid, large to coalescent, white-gray to salmon-pink colonies approximately 2 mm in diameter typically grow 48–72 hours after inoculation. NANAT (nalidixic acid, novobiocin, cycloheximide, and potassium tellurite) and CAZ-NB (ceftazidime, novobiocin, and cyclohexamide) selective media have been used to isolate the pathogen from feces, soil, or other contaminated samples.

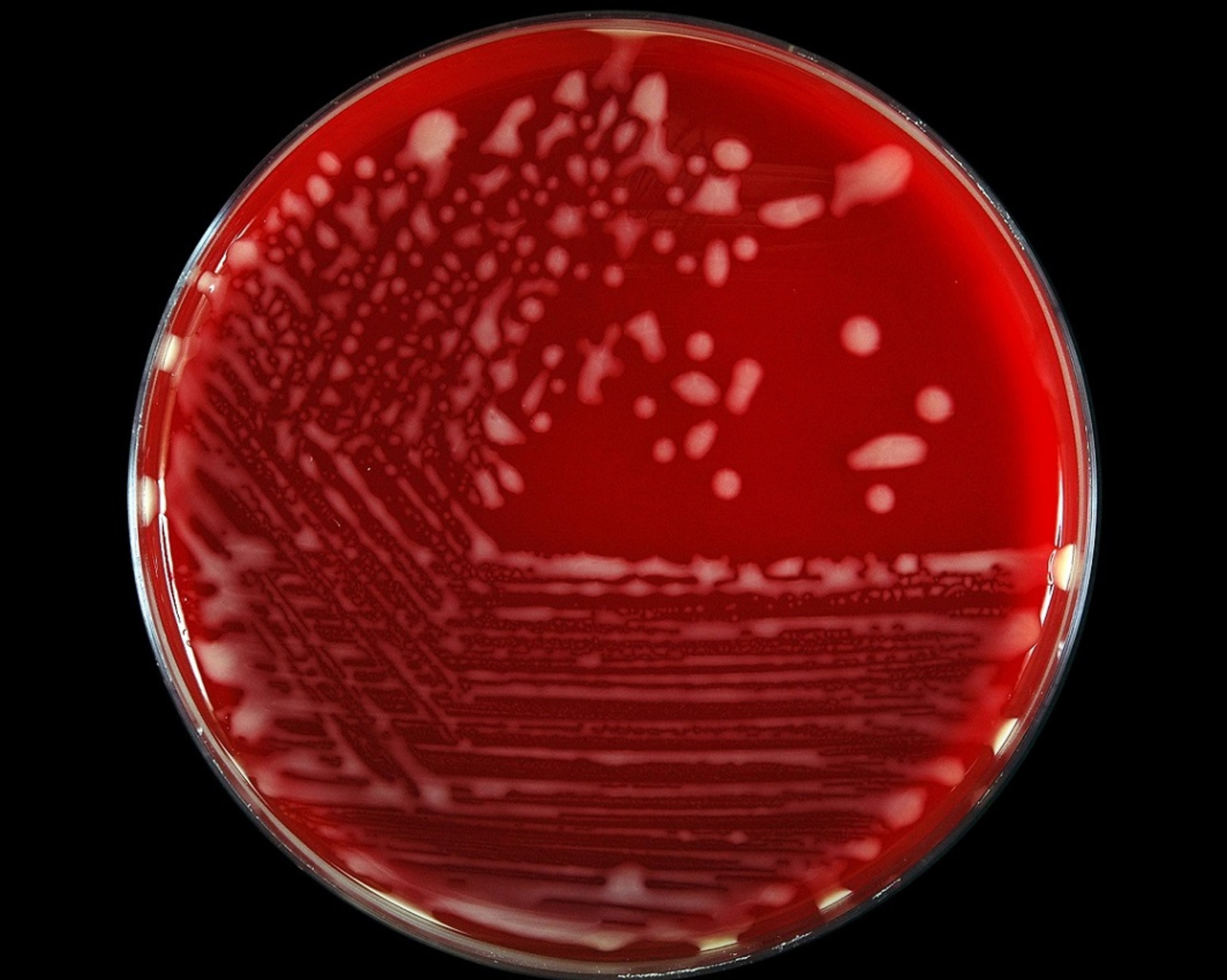
Courtesy of Dr. Márcio Garcia Ribeiro.
The ability of R equi to produce infections is related to different virulence factors, including capsular polysaccharide, a mycolic acid–containing lipid-rich cell wall structure and extracellular enzymes (phospholipase C and cholesterol oxidase). However, the major contributing virulence factor is its ability to multiply inside phagocytes, particularly in the presence of virulence-associated plasmids (VAPs). These large plasmids carry the vap pathogenicity island. To date, three host-adapted virulence plasmid types (pVAP, according to new unified nomenclature) of R equi are recognized: pVAPA (formerly VapA, virulent), pVAPB (formerly VapB, intermediately virulent), and recently identified pVAPN (“N” for neither A or B). pVAPA (gene vapA) seems to be the most important plasmid; however, the role of other multigene family members and their secreted proteins is not fully understood. The presence of VAPs is a critical determinant of R equi infectivity; however, a single property may not be sufficient to develop pathogenicity. Other virulence factors are probably involved as well, and the specific mechanism of interaction between VAP proteins and the host-pathogen remains incompletely elucidated. Strains that lack these three genes associated with virulence (vapA, vapB, vapN)—so-called plasmidless strains—are considered nonvirulent. The optimal condition for gene regulation and expression of the pathogen is a complex mechanism, influenced by the availability of certain elements (eg, iron, magnesium) and environmental factors (eg, temperature, pH), which could explain discrepancies in the prevalence of the disease in different geographic areas worldwide.
Epidemiology of Rhodococcus Infection in Animals
R equi is distributed worldwide , and the disease has a major economic impact on equine-breeding activities. The organism is commonly found in surface soil, feces of foals and other herbivores, and in farm environments. Soil is considered the main reservoir of the pathogen, which mainly uses herbivore feces as a growth substrate; it is eliminated in the feces of a wide variety of animal species, especially foals, swine, and other herbivores. R equi infections in foals are considered soil-associated. Particularly in foals, the organism has the ability to actively multiply in the intestinal tract when foals are is ~3 months old, and it can be isolated from the feces of adult horses. The pathogen may survive in the soil for greater than 12 months and can multiply at a wide range of temperatures (15°C–40°C [59°F–104°F]). R equi has been isolated from a large variety of domestic and wild species, including horses, swine, cattle, sheep, goats, dogs, cats, peccaries, buffalo, camelids, birds, and some wildlife; although horses, swine, and ruminants show some tropism (host-driven selection) of the organism.
Inhalation of soil dust particles is likely the major route of infection for pulmonary infections of domestic animals and humans. Infection via consumption of contaminated water or food are less frequent routes of R equi infection in animals, except for swine, wild boars, and peccaries, in which oral infection is apparently the main route.
Foals that develop pneumonia transmit R equi via aerosol transmission, and these patients may also swallow sputum, causing ulcerative colitis and mesenteric lymphadenitis. Traumatic percutaneous introduction of microorganisms, via direct contamination of wounds or penetration of mucous membranes, or secondary to scratches in cat fights, is the most common route of infection in companion animals. The presence of underlying systemic illness, including immunosuppression due to viral disease should be investigated in dogs (canine morbillivirus, formerly canine distemper virus) and cats (feline leukemia virus, feline immunodeficiency virus) with clinical rhodococcal disease.
In foals, clinical signs of R equi infection occur mainly between 2 weeks and 6 months of age, although signs of pulmonary disease typically peak in foals at 1–3 months of age. Disease in horses appears to be more prevalent in the presence of certain risk factors, such as large numbers of foals and mares, a transient equine population, high foal density, the birth of foals from mares shedding high numbers of the microorganism in the feces, and inadequate transfer of maternal antibodies by colostrum. Poor animal management, inadequate housing, the seasonal effect on foaling, and environmental conditions (temperature, dryness, dust, wind, soil pH, salinity, and concentrations of some elements) have also been reported as predisposing conditions.
Molecular epidemiologic studies based on the plasmid virulence profile of R equi isolated from animals and humans have revealed relative distinct tropism and geographic distribution worldwide. Most pVAPA (so-called equine type) variants are harbored by isolates that cause a typical life-threatening pyogranulomatous pneumonia and ulcerative colitis in foals from Europe, North and South America, Africa, and Japan. Curiously, a similar geographic distribution of pVAPB (porcine type) variants (formerly VapB types) is evident for isolates recovered from humans with pulmonary infections and for both lymphadenitis and apparently normal lymph nodes of swine, wild boars, and peccaries; with a predominance of variants 5 in Europe, 1 and 2 in Asia, and 8 in South America (particularly Brazil). pVAPN (bovine type), the third type that was recently recognized, has been predominantly recovered in isolates from lymph nodes of cattle and lungs of humans post mortem, especially patients living with HIV/AIDS; particularly isolates from Europe and the Americas. Occasionally, pVAPA and pVAPN types have been isolated from other animal species, such as dogs, cats, and goats. Plasmidless, or nonvirulent, R equi is found in production animal environments, as well as in soil or sand samples collected from human parks or yards, and even though no clinical signs are evident in domestic animals, nonvirulent strains have been reported in people living with HIV/AIDS.
Pathogenesis of Rhodococcus Infection in Animals
R equi is an opportunistic pathogen. The outcome of exposure to R equiis strongly influenced by the virulence and infective dose of the pathogen, as well as the age and immune status of the host. Virtually all foals are exposed to R equi shortly after birth, although most do not develop clinical signs. It is estimated that up to 90% of foals are infected by a subclinical form on horse-breeding farms where the disease is endemic. Adult horses are often resistant to infection or have clinical signs that spontaneously resolve because they are able to develop an effective immune response against the pathogen.
R equi invades the animal through the respiratory or digestive tracts, and occasionally through the skin, causing local or disseminated infections. It may be transmitted through hemolymphatic vessels, reaching different tissues and organs, causing pyogenic reactions in the liver, spleen, kidney, bones, brain, lymph nodes, and occasionally other organs.
The pathogenicity of R equi is attributed to its ability to invade, survive, and multiply inside neutrophils, especially, macrophages. It is able to evade the host's immune system likely by preventing phagosome-lysosome fusion (which prevents acidification and oxidation) or, via VAPs, which block the maturation of phagocytes. Uncontrolled intracellular multiplication of R equi in phagocytic cells leads to macrophage death by necrosis and release of a cascade of proinflammatory factors that ultimately produces abscesses and tissue destruction.
Apart from the presence of VAPs, other factors that contribute to R equipathogenesis and virulence include interactions with iron, the enzymes phospholipase C and cholesterol oxidase (so-called equi factors), and the presence of capsule and mycolic acid in the bacterial cell wall. In nonequine species, immunosuppressive conditions of the host may enable plasmidless strains to persist within phagocytes.
Passive humoral immunity transferred to foals by the ingestion of colostrum contributes to disease control. Naturally infected foals show an increased concentration of immunoglobulin (Ig) IgG isotypes (mainly IgGa, IgGb, and IgGT subisotypes), related to complement fixation and R equi opsonization. Nevertheless, the humoral response does not confer complete protection against R equiinfections. Consistent evidence supports the essential role of the cell-mediated immune response in clearing R equi infections, based mainly on secretion of various cytokines and direct cytotoxicity, including the action of T-lymphocytes CD4+ (helper) and CD8+ (cytotoxic), natural killer cells, interferon-gamma (a macrophage activator), and the production of some interleukins (eg, IL-4, IL-5, IL-13).
Clinical Findings of Rhodococcus Infection in Animals
Suppurative bronchopneumonia and ulcerative colitis in foals, lymphadenitis in cattle and swine, and cutaneous or organ abscesses are the most consistent clinical findings of rhodococcus infection in domestic animals. Rhodococcal infections are common in foals and swine but rare or uncommon in small ruminants, companion animals, birds, and wildlife species.
Horses
Bronchopneumonia with notable abscess formation is the major finding in foals with rhodococcus infection. Horses are typically affected at 2 weeks to 6 months old; however, most clinical signs are observed at 1–3 months old, possibly because of the decrease, at ~6 weeks of age, in passive immunity acquired via colostrum. On farms on which the disease is endemic, it is estimated that 5%–40% of infected foals may develop clinical signs, with a case fatality rate of up to 30%. Nevertheless, foals >6 months old may not show clinical signs. ( See also page Rhodococcus equi Pneumonia in Foals.)
Initially, affected foals develop nonspecific clinical signs—eg, mild fever, increased respiratory rate, inappetence, and lethargy; which may not be apparent unless foals are allowed to exercise. Worsening disease is characterized by more obvious signs of respiratory distress, including cough and strong inspiratory effort manifested by abdominal movement and nostril flaring; as well as tachycardia and tachypnea. On chest auscultation, inspiratory and expiratory wheezes and crackles may be audible, predominantly in the cranioventral region. Decreased airway sounds suggest lung consolidation, abscess formation, cavitary lesions, and pleural effusion. Mucous membranes may be pale, and cyanosis is present in severe cases. Weight loss and serous-to-mucopurulent nasal secretion are inconsistent clinical signs. Typically, an insidious onset occurs in foals because of the initial ability to compensate for respiratory lesions, making early diagnosis difficult.
Diarrhea, ulcerative colitis, colic, weight loss, mesenteric lymphadenitis, abdominal abscesses, typhlitis, and peritonitis are the main findings in foals affected by the abdominal form of rhodococcal disease. Foals rarely develop intestinal lesions without concomitant pulmonary signs; however, intestinal signs have been found in ~20% of foals with pulmonary rhodococcal infection.
Immune-mediated polysynovitis, caused by immune complex deposition in joints, affects 20%–30% of foals. Although any joint may be involved, the tibiotarsal and femoropatellar/femorotibial (stifle) joints are the most often affected. Usually, lameness is not apparent or is restricted to a stiff gait in affected foals. Examination of synovial fluid aspirates reveals nonseptic mononuclear pleocytosis, without isolation of R equi. Septic arthritis of foals is another arthropathy caused by R equi. Unlike immune-mediated polysynovitis, the septic lesion commonly causes severe signs of lameness. In such cases, synovial fluid aspirates reveal inflammation and typically enables microbiological isolation of the causative organism.
A variety of extrapulmonary signs of R equi infection occur in horses, including cellulitis and cutaneous abscesses, ulceration, intra-abdominal abscesses, lymphangitis, peripheral and visceral lymphadenomegaly, pleuritis, peritonitis, hepatitis, and hepatic encephalopathy. It is estimated that up to 50% of R equi–induced infections cause at least one extrapulmonary sign. Ocular signs, such as hypopyon and uveitis, may be observed in ~10% of cases. Osteomyelitis causing ataxia, decubitus, and limb paralysis is uncommon. Rarely, R equi is associated with abortion, placentitis, and infertility in mares, and it has been sporadically isolated from equine semen. Immune-mediated hemolytic anemia and immune-mediated thrombocytopenia have also been reported.
Clinical signs in adult horses are rare. The disease probably affects immunocompromised adult horses or animals coinfected with immunosuppressive agents, commonly infected by strains that harbor the pVAPA type. The predominant clinical signs in adult horses are similar to those in foals, including suppurative bronchopneumonia, lymphadenitis, enteritis, pleuritis, osteomyelitis, and the cutaneous form.
Swine and Similar Species
R equi infections may affect swine, peccaries, wild boars, feral pigs, and similar species and, in this group of animals, are restricted mainly to the lymphatic tract. Usually, pyogranulomatous cervical lymphadenitis is evident, although mesenteric, bronchial, and other lymph nodes may be involved. R equi has also been isolated from apparently normal lymph nodes. Occasionally, pneumonia has been reported. Gross lesions due to R equi infection that are found in lymph nodes examined routinely at the time of slaughter resemble those caused by mycobacteria infections, a major cause of swine lymphadenitis. ( See also page Tuberculosis in Pigs.)
Companion Animals
Rhodococcal disease in cats and dogs is rare, although it is reportedly more common in cats. Cutaneous and systemic clinical signs have been described. The most common route of infection in small animals is traumatic percutaneous introduction of the pathogen through contamination of wounds or via scratches in cat fights. Most affected cats have cutaneous lesions on one extremity, along with localized swelling, ulcers, and fistulas or multiple sinus tracts with purulent drainage. The lesions are commonly painful, although systemic signs are usually absent. Regional lymph nodes may be enlarged with purulent discharge. The systemic or disseminated form of R equiinfection has been reported, with pulmonary infections, hepatitis, and osteomyelitis. Pyothorax is usually secondary to dissemination of the organism from mediastinal lymph nodes, and these patients are presented with fever, anorexia, dyspnea, and weight loss. Such infections are accompanied by abdominal distention with palpable fluid, splenomegaly, hepatomegaly, and mesenteric lymphadenomegaly.
Ruminants
Lymphadenitis (mesenteric, submaxillary, and mediastinal), pneumonia, pyometra, ulcerative lymphangitis, and occasionally mastitis have been described in cattle and buffalo infected by R equi. Pneumonia and organ abscesses are the most common clinical findings in goats. Sporadic abortion and abscesses of organs have been reported in small ruminants.
Diagnosis of Rhodococcus Infection in Animals
Clinical examination and epidemiologic data
Hematologic and serum biochemical evaluation
Bacteriologic diagnosis
Diagnostic imaging
Serologic testing
Molecular diagnostic techniques
Histopathologic findings
Periodic clinical examinations, WBC counts, serum fibrinogen levels, microbiologic culture, diagnostic imaging, and serologic and molecular tests have been proposed as measures for early diagnosis, especially because of the insidious behavior of R equi–induced infections in foals.
Weekly physical examination, with an emphasis on thoracic auscultation and rectal temperature evaluation, is good clinical practice to prevent disease on farms. At least monthly monitoring of WBC counts (>13,000 cells/mcL) and serum fibrinogen concentrations (>400 mg/dL), in addition to thoracic radiography and ultrasonography evaluation, are valuable procedures for early diagnosis. Nevertheless, the efficacy of conventional serologic tests to identify infections in individual affected horses is poor or controversial.
Clinical and epidemiologic data are important for early diagnosis, although microbiologic isolation of R equi is required for conclusive diagnosis. Exudate from tracheobronchial-lavage, synovial and peritoneal fluid, skin, organs, and abscesses are the main clinical specimens sampled. Exudate from tracheobronchial lavage is the main clinical specimen for microbiologic culture in foals. Nonetheless, R equi may be present in the upper respiratory tract of healthy foals; therefore, the presence of R equi in the nasal region is not indicative of pulmonary infection. In addition, nasal swabs of foals are not recommended for diagnosis using nonselective culture media because of contamination with local microflora. Blood culture is a clinical specimen less commonly used for diagnosis, even though foals with positive blood culture are reportedly less likely to survive because such cultures indicate transmission of the bacterium.
Tracheobronchial fluid samples, swabs of cutaneous lesions, organs specimens, and abscess samples may be stained to obtain a presumptive diagnosis. The presence of pleomorphic intracellular gram-positive organisms supports a preliminary diagnosis, although careful evaluation is warranted because some clinical specimens may have a very small number of bacteria.

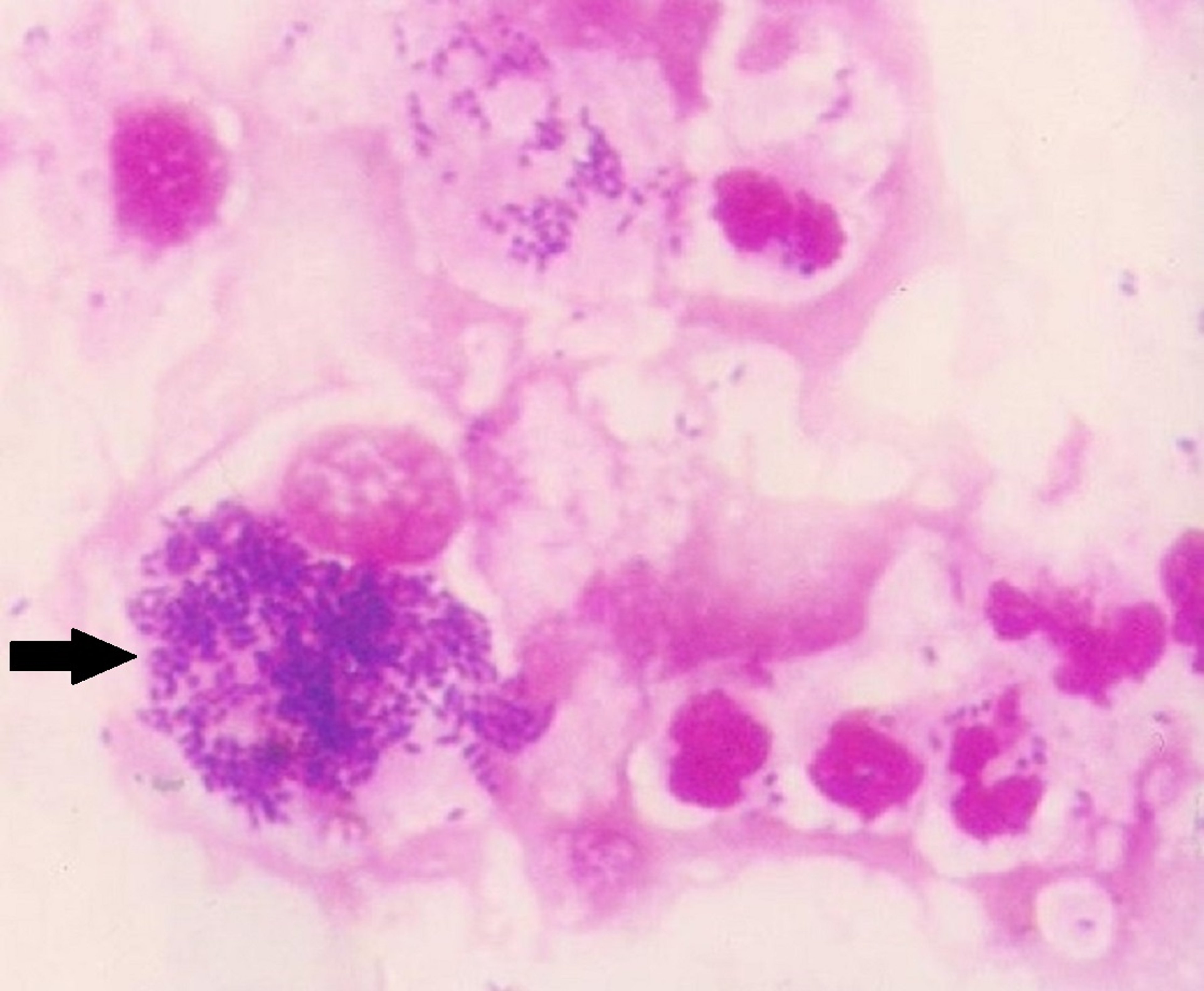
Courtesy of Dr. Márcio Garcia Ribeiro.
R equi is naturally isolated from feces in most foals, as well as production animals, particularly ruminants and swine. The pathogen has also been isolated from the feces of healthy cats living in a farm environment. Potentially contaminated material includes feces, soil, and sand of parks and yards, which requires microbiologic culture on selective media.
Neutrophilic leukocytosis, monocytosis, hyperfibrinogenemia, and hyperglobulinemia are been the most consistent hematologic findings in foals with rhodococcal infection. Serum amyloid A and plasma fibrinogen have been proposed as inflammatory biomarkers for diagnosis because concentrations of these acute-phase proteins are increased in foals infected by R equi. Abdominal and thoracic effusions are exudates found in animals with rhodoccocus infection and reveal increased neutrophils, lymphocytes counts and protein concentration.
Thoracic, abdominal, and joint radiography have been used in the imaging approach to diagnosis. Initial pneumonia is characterized by consolidation, and a mild to moderate diffuse bronchointerstitial pattern, revealing small nodules and possibly cavitary masses, which may be multiple and large in severe cases. Mediastinal lymphadenomegaly is occasionally observed. Thoracic ultrasonography often reveals lung consolidation and may be useful to identify disease in foals before noteworthy clinical signs appear. Computed tomography, magnetic resonance imaging, and scintigraphy are other imaging methods occasionally.
Use of serologic assays (eg, agar-gel immunodiffusion, radial immunodiffusion, synergistic hemolysis inhibition, and different ELISA assays) has been proposed in individual cases and in seroepidemiologic studies, particularly with horses. However, there is great variation in the titers (cutoff) and the performance of serologic tests, probably because of differences in antigen preparation, interference of maternal antibodies, and continuous exposure to R equi in the environment. In addition, serologic tests have failed to differentiate between healthy and sick foals and, therefore, are inappropriate for individual diagnosis.
Many molecular techniques have been used to detect the pathogen and/or VAPs—eg, conventional, multiplex, and real-time PCR assay, pulsed-field gel electrophoresis of DNA, matrix-associated laser desorption/ionization–time-of-flight mass spectrometry (MALDI-TOF MS), genome sequencing, multilocus sequence typing (MLST), and DNA-DNA hybridization. Detection of R equi–specific DNA by PCR assay is considered a rapid, suitable, and reliable means to confirm the diagnosis in foals. PCR assay, particularly the real-time technique, needs fewer microorganisms (10–100 CFUs/mL) to yield positive reactions. However, because R equi can be found in the upper respiratory tract of foals without pulmonary clinical signs, PCR assay may be positive in healthy animals. Thus, clinical and epidemiologic aspects, hematologic tests, imaging findings, microbiologic culture, and/or molecular assays should be considered in combination to confirm the diagnosis.
Lesions
Pneumonia, suppurative abscesses with necrotic areas, and regional lymphadenitis are the major gross lesions of rhodococcosis evident at necropsy. Typically, pulmonary lesions include multiple firm nodules, atelectasis, congestion, and miliary (isolated or multiple) and cavitary lesions. Multifocal enteritis, typhlitis, mesenteric lymphadenitis, and Peyer’s patches reaction occur in the enteric form of disease. Abdominal dissemination is characterized by peritonitis and visceral abscesses. Septic arthritis, hypopyon, and vertebral osteomyelitis are largely associated with hematogenous dissemination. Abortion, placentitis, and fetal infection are uncommon. R equi immune-mediated polysynovitis produces an increased synovial fluid volume in affected foals, but with preservation of the internal structure of the capsule; versus septic arthritis that is characterized by destruction of the joint capsule.

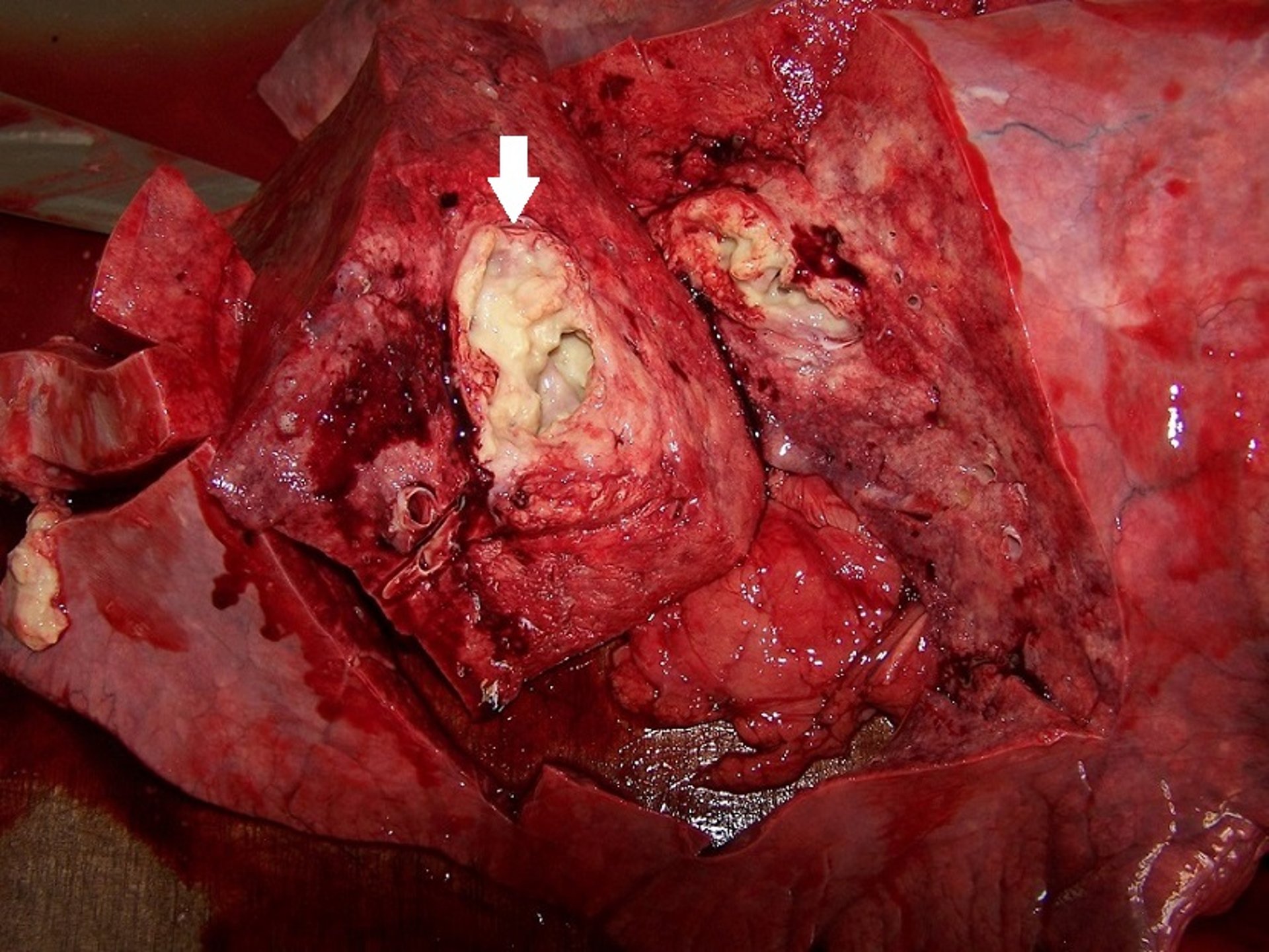
Courtesy of Dr. Márcio Garcia Ribeiro.
Histologically, lesions are characterized as pyogranulomatous with foci of necrosis. Numerous gram-positive pleomorphic organisms phagocytosed by macrophages, a variable number of multinucleate giant cells, and neutrophils are evident. Moderate infiltration of plasma cells and lymphocytes is also present.
The primary pathogens that should be differentiated from R equi as causal agents of pulmonary diseases in foals are Salmonella spp, Streptococcus equi and Streptococcus zooepidemicus, influenza virus, herpesvirus, and migrating stages of Parascaris equorum. The main differential diagnoses of enteric R equi infections are considered to be Salmonella spp and Clostridium spp, as well as Escherichia coli, Strongyloides westeri, rotavirus, and coronavirus. Septic arthritis due to R equi should be differentiated especially from that caused by Salmonella spp and Streptococcus equi. Swine lymphadenitis caused by mycobacteria should be distinguished from R equi because of the similar appearance of lymph nodes at slaughter.
Treatment of Rhodococcus Infection in Animals
Assessment of in vitro susceptibility pattern, followed by antimicrobial therapy
Supportive care
Treatment consists of appropriate antimicrobial therapy, surgical drainage, debridement, and supportive care. However, natural R equi infections are typically refractory to treatment, probably because of the intracellular location of the pathogen, development of pyogranulomatous lesions, and infection by multiple strains at once. In addition, the in vitro antimicrobial susceptibility pattern of isolates may vary geographically, which, in addition to differences of host susceptibility to the pathogen, may explain why the success of any given therapy varies among animal species.
In vitro antimicrobial susceptibility profiles of R equi strains recovered from infections in animals and humans usually reveal sensitivity to rifamycins (rifampin), macrolides (erythromycin, azithromycin, clarithromycin), aminoglycosides (gentamicin, neomycin), lincosamides (lincomycin), sulfonamides (sulfadiazine or sulfamethoxazole), and carbapenems (imipenem), although lipid-soluble drugs are considered a first choice because they achieve therapeutic levels in pulmonary tissue and within phagocytes, particularly alveolar macrophages.
Since the 1980s, the conventional antimicrobial protocol for R equiinfection in foals has been based on the combination of rifampin (5 mg/kg, PO, every 12 hours, or 10 mg/kg every 24 hours) and erythromycin (25 mg/kg, PO, every 8 hours; or 37.5 mg/kg, PO, every 12 hours). These drugs have a synergistic effect that decreases bacterial resistance rates. More recently, two newer-generation macrolides—clarithromycin (7.5 mg/kg, PO, every 12 hours) and azithromycin (10 mg/kg per day, PO, for 5–7 days, and then once every 2 days)—have been proposed as alternatives to treat foals because of their bioavailability, stability, and ability to penetrate cells and the pulmonary tract at higher concentrations than erythromycin. The rifampin-clarithromycin combination has shown better efficacy than rifampin-azithromycin or rifampin-erythromycin. Azithromycin has been used as an alternative to erythromycin in foals with adverse clinical signs after prolonged use of erythromycin, especially diarrhea. Many antimicrobials, including gamithromycin, show anecdotal success in treating food-producing animals with R equi. Selection of antibiotics should be based on culture and sensitivity. Local and state regulations regarding restrictions for drug use in food-producing animals should be followed.
The usual recommendation is longterm therapy (duration 3–12 weeks), depending on the animal species, tissues affected, and severity of clinical signs. Treatment may be extended in complicated cases such as foals with osteomyelitis, septic arthritis, and cavitary pulmonary lesions; however, after a long course of antimicrobial therapy, some animals may develop antimicrobial-associated colitis. R equi isolates resistant to the macrolides and rifampin are apparently uncommon; however, this has been an emergent issue and may be increasingly likely with the use of these drugs as monotherapy or with mass antimicrobial treatment of subclinical infections in foals that show lesions compatible with pulmonary rhodococcosis. Treatment should be continued until affected foals are clinically normal and other parameters used for diagnosis (fibrinogen concentration, WBC count, diagnostic imaging) have also returned to normal.
In small animals, combined therapy with rifampin (10 mg/kg per 24 hours, PO) and clarithromycin (7.5-12.5 mg/kg, PO, every 12 hours) for 2–6 weeks has been reported. The combination of lincomycin (20 mg/kg, PO, every 12 hours, for 7–10 days) and gentamicin (5–8 mg/kg per day, SC, IM, or IV, for 5 days) has been reported to be effective in some cats; however, a longer duration or second course of antimicrobial therapy may be necessary. Erythromycin (15 mg/kg, PO, every 12 hours, for 14 days) may be combined with rifampin or other drugs in the treatment of dogs and cats. Premafloxacin, an extended-spectrum quinolone, has been shown to have in vitro efficacy against R equi isolates.
Surgical debridement and drainage of abscesses are indicated in some patients with cutaneous lesions. Adequate hydration and nutrition are recommended as part of supportive care. NSAIDs may be used to control fever and to treat arthritis or other inflammatory manifestations.
Despite appropriate antimicrobial therapy and supportive care, animals with respiratory distress, tachycardia, severe thoracic imaging abnormalities, and osteomyelitis have a poor prognosis. A poor prognosis has also been associated with foals that have both pulmonary signs and concomitant extrapulmonary signs (eg, intra-abdominal abscessation, pleural effusion, hepatitis, nephritis).
Control and Prevention of Rhodococcus Infection in Animals
Control procedures are recommended to optimize the resistance of foals to R equi–induced infections. Ensuring adequate transfer of colostrum immunoglobulins in 1-day-old foals is crucial. Various measures to prevent and control disease, especially in foals—eg, decreasing of environmental exposure to R equi, use of screening tests for early identification of affected animals, antimicrobial prophylaxis, and use of passive (hyperimmune plasma, purified immunoglobulins) and active (vaccination) immunization—have been proposed.
The exposure of domestic animals, particularly foals, to R equi in the environment is suggested as the main risk factor for transmission. A high number of mares and foals on endemic farms leading to a higher rate of fecal shedding of R equi, appear to be predominant risk factors for equine disease. Thus, decreasing the number of mares and foals, as well as foal density, have been recommended on endemic farms.
Removal of excess feces from paddocks, stalls, and pastures could decrease the proliferation of R equi and, consequently, the risks of infection. Nonetheless, high concentrations of pathogenic R equi may be found in the feces of foals clinically affected, because foals commonly swallow sputum , which contains these virulent strains, and then shed the bacteria in feces. Therefore, foals with clinical signs should be isolated and their feces removed immediately as a measure to control the disease locally.
Direct involvement of dust as the main risk factor for transmission of rhodococcosis in production animals and horses is controversial. Nevertheless, irrigating paddocks and stalls, in addition to growing grass in foal environments that are excessively dusty, may be considered to decrease aerosolization.
On endemic breeding farms, regular physical examination (including thoracic auscultation), measurement of hematologic parameters (WBC count, serum amyloid A, and plasma fibrinogen levels), and diagnostic imaging procedures (chest radiography and ultrasonography) may permit early diagnosis and isolation of infected foals, enabling adequate control and effective treatment.
Administration of hyperimmune plasma is an alternative prophylactic measure to provide passive immunization of horses against R equi. It is based on the protective action of plasma components (immunoglobulin, interferon, complement factors, cytokines, and fibronectin). Hyperimmune plasma reduces the severity of clinical signs in foals; however, it does not have a curative effect or shorten the course of the disease. Administration protocols vary; however, hyperimmune plasma is most effective when administered before exposure to R equi. Most commonly, at least 1 L of hyperimmune plasma (or 20 mL/kg) , IV, is administered to foals 1–60 days old. The initial dose for foals is variably given at 1–7 days old, even though better results have been observed if the plasma is administered no later than the second day of life. However, because the level of protection provided by hyperimmune plasma may decrease weeks after the first dose, when foals are still susceptible to infection, a second dose often is required at ~2–4 weeks old. Nonetheless, because foals are challenged early (first days of life), the first dose is probably the most effective for protection. In addition, because the endemic condition of the disease apparently is not determined by a specific-farm R equi isolate, and because foals may be infected by multiple strains simultaneously, hyperimmune plasma that is produced through the immunization of horses on a given farm may be used on another breeding farm. The clinical severity of pneumonia in foals has been decreased by injecting foals with purified immunoglobulins obtained from horses immunized with specific VAPs.
Treating all foals by prophylactic administration of antimicrobials during the first weeks of age, when animals are most susceptible to R equi–induced infections, is another documented approach to control and prevention. Azithromycin, administered in the first two weeks of life, has been favored in this preventive approach because of its oral availability, long half-life, and ability to achieve adequate concentrations in phagocytic cells and the pulmonary tract. However, overuse of azithromycin might enhance selective pressure to macrolide-resistant isolates, an emergent global concern.
Different vaccines have been proposed to induce active immunity in mares and foals. Vaccination of mares against R equi does not provide adequate protection of foals against pneumonia or extrapulmonary infections caused by the transfer of immunoglobulins through colostrum in the first hours of life, even though specific antibody levels may be appreciably increased in colostrum.
Most foals naturally challenged with virulent R equi strains develop a protective and prolonged immune response. Because cell-mediated immunity is critical to confer protection against R equi infections of foals, active immunization of young animals is probably crucial to adequate protection. Nonetheless, poor neonatal response or relative immunologic immaturity, interference with maternal antibodies, and the intracellular location of R equi limit the action of conventional vaccines in foals in field conditions.
Killed vaccines have shown a lack of capacity in inducing a cellular immune response against R equi. Infection by R equi strains that lack vapA and vapB genes does not induce protection in foals, indicating that virulent strains are essential for effective vaccines. Studies in experimental and field conditions using oral immunization with Salmonella enterica serovar Typhimurium carrying the pVAPA antigen, a DNA vaccine containing vapA gene, an intrabronchial vaccine with attenuated R equi strain, and a deletion mutant vaccine have been proposed. In addition, efforts are ongoing to develop promising vaccines using transposons and recombinant and DNA vaccines containing VAP antigens. Nonetheless, to date, available vaccines against R equi infections have shown inadequate efficacy in the prevention and control of disease when used in either foals or mares.
Zoonotic Risk of Rhodococcus Infection in Animals
Human rhodococcosis is an opportunistic disease, related to occupation. In addition, it appears to be zoonotic in nature because, in contrast to certain host tropism of virulence plasmids for some animal species, the three pVAP types have been detected in humans, suggesting that animals are a source of infection in humans.
Traditionally, contact with soil or manure, or inhalation of aerosols contaminated by the production animal environment, have been the major routes of R equi transmission from animals to humans. Alternatively, infections in humans may occur by contamination through transcutaneous trauma, ingestion, or wound or mucous membranes. Recent evidence supports that consumption of undercooked pork or bovine products contaminated by R equi pVAPB or pVAPN types, respectively, may represent a probable route of infection in humans because of slaughter contamination of the meat with lymph node content or feces. Nonetheless, clinical signs have been reported in immunosuppressed patients infected by plasmidless R equi as well.
Extrapulmonary clinical signs have been occasionally recorded in humans, even though in recent years R equi has emerged as a pulmonary pathogen in immunosuppressed individuals or affected by underlying conditions, particularly transplant patients receiving immunosuppressive therapy and people living with HIV/AIDS, with or without a history of contact with production animals or their environment. In addition, infected companion animals with draining lesions may pose a risk to immunosuppressed owners. Therefore, in general, to prevent rhodococcosis, immunocompromised or debilitated people should avoid contact with diseased companion animals, production animals, or their environments, as well as consumption of undercooked pork and bovine products.
Key Points
R equi has emerged as a presumably foodborne zoonotic pathogen, opportunistic in nature, associated with pyogranulomatous clinical infections in animals and humans.
Three host-adapted virulence plasmid types (pVAPA, pVAPB, and pVAPN) are distinguished, with infections of equine, porcine, and bovine or caprine origin, respectively. Humans are infected by all three VAP types.
Suppurative pneumonia, lymphadenitis, abscesses in organs, and cutaneous-subcutaneous lesions are the main clinical signs in horses, production animals and dogs and cats.
Lipid-soluble antimicrobials are the first choice in treatment because they achieve therapeutic levels within infected phagocytes.


